
Burns and Truog
Burns and Truog
You might also like
- Nursing Care Plan - BronchitisDocument2 pagesNursing Care Plan - Bronchitisderic94% (36)
- Comm 1010 Informative Full-Sentence Speech Outline InstructionsDocument2 pagesComm 1010 Informative Full-Sentence Speech Outline Instructionsapi-270505782No ratings yet
- Phil335 Assignment 2 Phil Ethics EssayDocument9 pagesPhil335 Assignment 2 Phil Ethics Essayapi-291788435No ratings yet
- Ethical Concerns About Emerging Treatment Paradigms For Gender DysphoriaDocument37 pagesEthical Concerns About Emerging Treatment Paradigms For Gender DysphoriapoimartiNo ratings yet
- End of LifeCareDocument5 pagesEnd of LifeCareRachmat KamaluddinNo ratings yet
- NSG 106Document12 pagesNSG 106Anipah AmintaoNo ratings yet
- Treatment Recommendation in Vietnamese Medical Consultations (Final)Document19 pagesTreatment Recommendation in Vietnamese Medical Consultations (Final)Global Research and Development ServicesNo ratings yet
- Medical Futility: A Paradigm As Old As HippocratesDocument5 pagesMedical Futility: A Paradigm As Old As HippocratescindyNo ratings yet
- Treatment Recommendation in Vietnamese Medical Consultations (Final)Document18 pagesTreatment Recommendation in Vietnamese Medical Consultations (Final)Global Research and Development ServicesNo ratings yet
- Futilidad y Decir Que NoDocument21 pagesFutilidad y Decir Que NoBelisario AguayoNo ratings yet
- Theroleofpatients: Shared Decision-MakingDocument20 pagesTheroleofpatients: Shared Decision-MakingMaryela MenachoNo ratings yet
- Paternalism Modernised: Author's AbstractDocument4 pagesPaternalism Modernised: Author's AbstractAnthony KabadiNo ratings yet
- Performing Informed Consent in Transgender MedicineDocument8 pagesPerforming Informed Consent in Transgender MedicineJahlin HabbeiNo ratings yet
- Truth Tell CMAJDocument4 pagesTruth Tell CMAJmartinNo ratings yet
- Ten Common Questions (And Their Answers) On Medical FutilityDocument17 pagesTen Common Questions (And Their Answers) On Medical FutilitycindyNo ratings yet
- Medical Futility: 23 (Suppl. 11), 11-6-11-16 (2000)Document11 pagesMedical Futility: 23 (Suppl. 11), 11-6-11-16 (2000)cindyNo ratings yet
- In Support of Same-Sex Marriage: EditorialsDocument2 pagesIn Support of Same-Sex Marriage: EditorialsNatalina Dass Tera LodatoNo ratings yet
- Ethical IssueDocument22 pagesEthical Issuedhurgashny98No ratings yet
- Conscientious Objection and Emergency Contraception: Robert F. Card, State University of New York, OswegoDocument8 pagesConscientious Objection and Emergency Contraception: Robert F. Card, State University of New York, OswegoHola HombreNo ratings yet
- Miss Evers BoysDocument4 pagesMiss Evers Boysarij 20100% (4)
- Regarding Obesity As A Disease Evolving Policies and Their ImplicationsDocument13 pagesRegarding Obesity As A Disease Evolving Policies and Their ImplicationsZENIFF GOMEZ ARCIVENo ratings yet
- Garlic For Total Cholesterol ReductionDocument10 pagesGarlic For Total Cholesterol ReductionAndrew NugrohoNo ratings yet
- Elder Law News & Notes Feb 2010 Number 67Document4 pagesElder Law News & Notes Feb 2010 Number 67Kyle EspinozaNo ratings yet
- One Size Fits All RevisedDocument39 pagesOne Size Fits All RevisedMark Norriel CajandabNo ratings yet
- Thesis On Physician Assisted DeathDocument5 pagesThesis On Physician Assisted Deathbnjkstgig100% (2)
- SawickiDocument55 pagesSawickiAdrian GuzmanNo ratings yet
- 43849-Article Text-41744-1-10-20090701Document4 pages43849-Article Text-41744-1-10-20090701Ahmed H. Ali ElbestaweyNo ratings yet
- Thesis Euthanasia PaperDocument5 pagesThesis Euthanasia Paperbsqkr4kn100% (2)
- Euthanasia Research Paper ThesisDocument6 pagesEuthanasia Research Paper Thesisczozyxakf100% (1)
- Caring, Curing, Coping: Nurse, Physician, and Patient RelationshipsFrom EverandCaring, Curing, Coping: Nurse, Physician, and Patient RelationshipsNo ratings yet
- The Healing Touch: Keeping the Doctor-Patient Relationship Alive Under Managed CareFrom EverandThe Healing Touch: Keeping the Doctor-Patient Relationship Alive Under Managed CareRating: 5 out of 5 stars5/5 (1)
- Currently Medical Ethics For PhysiciansDocument16 pagesCurrently Medical Ethics For PhysiciansOmarNo ratings yet
- Assignment 3 WORDDocument7 pagesAssignment 3 WORDJoanna KwiatkowskiNo ratings yet
- Inappropr Ther STDocument13 pagesInappropr Ther STRESCATEURNo ratings yet
- Yates-Doerr. Contando Cuerpos...Document18 pagesYates-Doerr. Contando Cuerpos...María BergeroNo ratings yet
- Ethics and The Legalization of Physician-Assisted Suicide - An American College of Physicians Position PaperDocument12 pagesEthics and The Legalization of Physician-Assisted Suicide - An American College of Physicians Position PaperRoberto López MataNo ratings yet
- Research Reportwiener1998Document12 pagesResearch Reportwiener1998maglangitmarvincNo ratings yet
- Euthanasia Research Paper Thesis StatementDocument4 pagesEuthanasia Research Paper Thesis Statementgbxqaf9v100% (2)
- Annotated Bibliography Medical EthicsDocument7 pagesAnnotated Bibliography Medical Ethicsapi-311220399No ratings yet
- Research Paper On Physician Assisted DeathDocument8 pagesResearch Paper On Physician Assisted Deathrsjpinynd100% (1)
- Profesionalismo MedicoDocument15 pagesProfesionalismo MedicoR4pT0r666No ratings yet
- First Draft 1 1302Document9 pagesFirst Draft 1 1302api-742824399No ratings yet
- Christopher Boorse (Auth.), James M. Humber, Robert F. Almeder ( - What Is Disease - (1997, Humana) (10.1007 - 978!1!59259-451-1) - Libgen - LiDocument358 pagesChristopher Boorse (Auth.), James M. Humber, Robert F. Almeder ( - What Is Disease - (1997, Humana) (10.1007 - 978!1!59259-451-1) - Libgen - LiLeon TrellesNo ratings yet
- Did The Doctor Do The Right Thing EditedDocument4 pagesDid The Doctor Do The Right Thing EditedmmhNo ratings yet
- Research Paper On Euthanasia FreeDocument6 pagesResearch Paper On Euthanasia Freeqbqkporhf100% (1)
- Against Euthanasia ThesisDocument4 pagesAgainst Euthanasia Thesispzblktgld100% (2)
- Questionable Cancer TherapiesDocument21 pagesQuestionable Cancer Therapiesvaxya100% (2)
- ÉTICA - Aula 1 - A Piece of My Mind Winners and Loosers JAMADocument2 pagesÉTICA - Aula 1 - A Piece of My Mind Winners and Loosers JAMAFelipe DiasNo ratings yet
- Student 1 Week 4 Discussion: Amanda Dubreuiel PostedDocument3 pagesStudent 1 Week 4 Discussion: Amanda Dubreuiel PostedAlpha RalakNo ratings yet
- Tutorial - ETHICS - 01-01-P1&2 - Introduction To Ethics and Biomedical Ethics & Ethical Issues in Doctor-Patient RelationshipsDocument43 pagesTutorial - ETHICS - 01-01-P1&2 - Introduction To Ethics and Biomedical Ethics & Ethical Issues in Doctor-Patient RelationshipsRenNo ratings yet
- Medical EthicsDocument6 pagesMedical Ethicsdobuol gorNo ratings yet
- Final Project 4 RewriteDocument11 pagesFinal Project 4 Rewriteapi-710396108No ratings yet
- Habit 5 PDFDocument2 pagesHabit 5 PDFPrashant PatilNo ratings yet
- Patient Rights: January 2016Document10 pagesPatient Rights: January 2016CharanNo ratings yet
- Refusal To Treat A PatientDocument4 pagesRefusal To Treat A Patientzwecker4458No ratings yet
- Medical EthicsDocument5 pagesMedical EthicsAdhyambo MakyaNo ratings yet
- Lecture Research EthicsDocument1 pageLecture Research EthicsAngel HeartNo ratings yet
- A Clear Case For Conscience in Healthcare Practice: Giles BirchleyDocument6 pagesA Clear Case For Conscience in Healthcare Practice: Giles BirchleyFuraya FuisaNo ratings yet
- Illich 1975 Medicalization of LiDocument6 pagesIllich 1975 Medicalization of Liaardvark62No ratings yet
- Professional Integrity and The Role of Medical Students in Professional Self-RegulationDocument5 pagesProfessional Integrity and The Role of Medical Students in Professional Self-RegulationMaría Jesús Carrión MansillaNo ratings yet
- Essay Lol Draft Haha M, EdicinesDocument3 pagesEssay Lol Draft Haha M, EdicinestheultimatetrovianNo ratings yet
- DNR and Medical FutilityDocument13 pagesDNR and Medical Futilityapi-216057141No ratings yet
- Duffy (A Minor) - V - National Maternity Hospital (2012) IEHC 354Document51 pagesDuffy (A Minor) - V - National Maternity Hospital (2012) IEHC 354SANDHYANo ratings yet
- Gillon (2003) Four ScenariosDocument3 pagesGillon (2003) Four ScenariosSANDHYANo ratings yet
- Quality of Dying in ICU Ways To Make It BetterDocument1 pageQuality of Dying in ICU Ways To Make It BetterSANDHYANo ratings yet
- Justice Baker (2017) A Matter of Life and DeathDocument9 pagesJustice Baker (2017) A Matter of Life and DeathSANDHYANo ratings yet
- Quebec UpdateDocument3 pagesQuebec UpdateSANDHYANo ratings yet
- HSE Guidance Re CPR and DNAR Decision Making During The COVID 19 PandemicDocument15 pagesHSE Guidance Re CPR and DNAR Decision Making During The COVID 19 PandemicSANDHYANo ratings yet
- HSE Background Note To Guidance On CPR and DNAR in Decision Making During The COVID 19 PandemicDocument1 pageHSE Background Note To Guidance On CPR and DNAR in Decision Making During The COVID 19 PandemicSANDHYANo ratings yet
- Editorial (2017) NEW FRONTIERS IN END-OF-LIFE ETHICSDocument2 pagesEditorial (2017) NEW FRONTIERS IN END-OF-LIFE ETHICSSANDHYANo ratings yet
- Powell T. Et Al (2017) A Good DeathDocument2 pagesPowell T. Et Al (2017) A Good DeathSANDHYANo ratings yet
- Madden Deirdre (2013) Is There A Right To A "Good Death"Document12 pagesMadden Deirdre (2013) Is There A Right To A "Good Death"SANDHYANo ratings yet
- DOH Procedural Values For Decision-Making in A PandemicDocument6 pagesDOH Procedural Values For Decision-Making in A PandemicSANDHYANo ratings yet
- White, B. Et Al (2017) The Role of Law in Decisions To Withhold AndlDocument8 pagesWhite, B. Et Al (2017) The Role of Law in Decisions To Withhold AndlSANDHYANo ratings yet
- AMA CEJF Statement Re Physician-Assisted Suicide A18-Ceja5Document8 pagesAMA CEJF Statement Re Physician-Assisted Suicide A18-Ceja5SANDHYANo ratings yet
- Rivera-Lopez E (2017) Is Medically Assisted Death A Special ObligationDocument7 pagesRivera-Lopez E (2017) Is Medically Assisted Death A Special ObligationSANDHYANo ratings yet
- DOH Ethical Framework For Decision Making in A PandemicDocument19 pagesDOH Ethical Framework For Decision Making in A PandemicSANDHYANo ratings yet
- Donnelly Sonya (2009) The Evolution of The Law On Assisted Suicide in The United Kingdom and The Possible ImplicationDocument15 pagesDonnelly Sonya (2009) The Evolution of The Law On Assisted Suicide in The United Kingdom and The Possible ImplicationSANDHYANo ratings yet
- DOH Ethical Considerations Relating To Lon-Term Residential Care Facilities in The Constext of COVID 19Document11 pagesDOH Ethical Considerations Relating To Lon-Term Residential Care Facilities in The Constext of COVID 19SANDHYANo ratings yet
- Dying at Home Cultural and Religious PreferencesDocument2 pagesDying at Home Cultural and Religious PreferencesSANDHYANo ratings yet
- Lung SoundsDocument6 pagesLung SoundsQuinn Madalang100% (1)
- American Medical Association - ICD-10-CM Documentation - Essential Charting Guidance To Support Medical Necessity 2019-American Medical Association (2018)Document1,229 pagesAmerican Medical Association - ICD-10-CM Documentation - Essential Charting Guidance To Support Medical Necessity 2019-American Medical Association (2018)johnharnsberry100% (1)
- The Five Eras of ChiropracticDocument8 pagesThe Five Eras of ChiropracticSam100% (1)
- The Impact of An Online Educational Game On Breast Cancer Awareness Among University Female Students, Malaysia: A Pilot StudyDocument11 pagesThe Impact of An Online Educational Game On Breast Cancer Awareness Among University Female Students, Malaysia: A Pilot StudySteve GannabanNo ratings yet
- lEGAL MEDICINE Sex CrimesDocument12 pageslEGAL MEDICINE Sex Crimesralna_florano1467No ratings yet
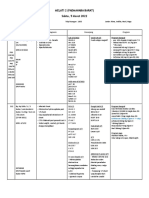
- Operan Jaga 5 Maret 2022Document29 pagesOperan Jaga 5 Maret 2022Rafaela LennyNo ratings yet
- EpisiotomyDocument3 pagesEpisiotomyAlexandra Chiriac AntonNo ratings yet
- Running Head: Fast Tracks in The Emergency Department 1Document11 pagesRunning Head: Fast Tracks in The Emergency Department 1FikriNo ratings yet
- On Catatonia Seizures and BradycardiaDocument1 pageOn Catatonia Seizures and BradycardiaFlorin TudoseNo ratings yet
- Thyroid Disorder Research PaperDocument5 pagesThyroid Disorder Research Paperapi-254922343No ratings yet
- Pharma Formulation Challenges & Innovations-2Document8 pagesPharma Formulation Challenges & Innovations-2Sundaram ShuklaNo ratings yet
- OncologyDocument3 pagesOncologyMichtropolisNo ratings yet
- A SepsisDocument5 pagesA SepsisAi KogaNo ratings yet
- Cues Nursing Diagnosis Scientific Reason Planning Intervention Rationale EvaluationDocument6 pagesCues Nursing Diagnosis Scientific Reason Planning Intervention Rationale EvaluationKatrina Ponce86% (7)
- 10 1080@1744666X 2019 1705785Document85 pages10 1080@1744666X 2019 1705785infectologia larazaNo ratings yet
- Basic Life Support Training Manualnew PDFDocument88 pagesBasic Life Support Training Manualnew PDFkekoho4589100% (1)
- Diagnostic CentreDocument14 pagesDiagnostic CentreJonas AsiaNo ratings yet
- NCP For Deficient Fluid VolumeDocument2 pagesNCP For Deficient Fluid VolumeRedwing_Dc_854758% (12)
- Assessments of Safe Medication Administration in Nursing EducationDocument12 pagesAssessments of Safe Medication Administration in Nursing EducationMichael AmandyNo ratings yet
- Drug SupplyDocument441 pagesDrug SupplyJIBRIL ALINo ratings yet
- Lympografi LainDocument39 pagesLympografi LainYuda FhunkshyangNo ratings yet
- Juan Dela Cruz, RRT: Personal InformationDocument3 pagesJuan Dela Cruz, RRT: Personal InformationShiela Leomo-VillaramaNo ratings yet
- 1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingDocument14 pages1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingKamx Mohammed100% (1)
- Perbandingan Dexa Dan MethylprednisoloneDocument2 pagesPerbandingan Dexa Dan MethylprednisoloneRai Jaine DarmantaNo ratings yet
- Male Infertility PDFDocument7 pagesMale Infertility PDFFaizatul ImanNo ratings yet
- Case Discussion Day 2 - MatulaDocument1 pageCase Discussion Day 2 - MatulaTRISHA MATULANo ratings yet
- Natara LandrauDocument2 pagesNatara Landraudmarkee4No ratings yet
- Headache Clinic CRFDocument12 pagesHeadache Clinic CRFNasirNo ratings yet









































































































Download as pdf or txt
You might also like
- Nursing Care Plan - BronchitisDocument2 pagesNursing Care Plan - Bronchitisderic94% (36)
- Comm 1010 Informative Full-Sentence Speech Outline InstructionsDocument2 pagesComm 1010 Informative Full-Sentence Speech Outline Instructionsapi-270505782No ratings yet
- Phil335 Assignment 2 Phil Ethics EssayDocument9 pagesPhil335 Assignment 2 Phil Ethics Essayapi-291788435No ratings yet
- Ethical Concerns About Emerging Treatment Paradigms For Gender DysphoriaDocument37 pagesEthical Concerns About Emerging Treatment Paradigms For Gender DysphoriapoimartiNo ratings yet
- End of LifeCareDocument5 pagesEnd of LifeCareRachmat KamaluddinNo ratings yet
- NSG 106Document12 pagesNSG 106Anipah AmintaoNo ratings yet
- Treatment Recommendation in Vietnamese Medical Consultations (Final)Document19 pagesTreatment Recommendation in Vietnamese Medical Consultations (Final)Global Research and Development ServicesNo ratings yet
- Medical Futility: A Paradigm As Old As HippocratesDocument5 pagesMedical Futility: A Paradigm As Old As HippocratescindyNo ratings yet
- Treatment Recommendation in Vietnamese Medical Consultations (Final)Document18 pagesTreatment Recommendation in Vietnamese Medical Consultations (Final)Global Research and Development ServicesNo ratings yet
- Futilidad y Decir Que NoDocument21 pagesFutilidad y Decir Que NoBelisario AguayoNo ratings yet
- Theroleofpatients: Shared Decision-MakingDocument20 pagesTheroleofpatients: Shared Decision-MakingMaryela MenachoNo ratings yet
- Paternalism Modernised: Author's AbstractDocument4 pagesPaternalism Modernised: Author's AbstractAnthony KabadiNo ratings yet
- Performing Informed Consent in Transgender MedicineDocument8 pagesPerforming Informed Consent in Transgender MedicineJahlin HabbeiNo ratings yet
- Truth Tell CMAJDocument4 pagesTruth Tell CMAJmartinNo ratings yet
- Ten Common Questions (And Their Answers) On Medical FutilityDocument17 pagesTen Common Questions (And Their Answers) On Medical FutilitycindyNo ratings yet
- Medical Futility: 23 (Suppl. 11), 11-6-11-16 (2000)Document11 pagesMedical Futility: 23 (Suppl. 11), 11-6-11-16 (2000)cindyNo ratings yet
- In Support of Same-Sex Marriage: EditorialsDocument2 pagesIn Support of Same-Sex Marriage: EditorialsNatalina Dass Tera LodatoNo ratings yet
- Ethical IssueDocument22 pagesEthical Issuedhurgashny98No ratings yet
- Conscientious Objection and Emergency Contraception: Robert F. Card, State University of New York, OswegoDocument8 pagesConscientious Objection and Emergency Contraception: Robert F. Card, State University of New York, OswegoHola HombreNo ratings yet
- Miss Evers BoysDocument4 pagesMiss Evers Boysarij 20100% (4)
- Regarding Obesity As A Disease Evolving Policies and Their ImplicationsDocument13 pagesRegarding Obesity As A Disease Evolving Policies and Their ImplicationsZENIFF GOMEZ ARCIVENo ratings yet
- Garlic For Total Cholesterol ReductionDocument10 pagesGarlic For Total Cholesterol ReductionAndrew NugrohoNo ratings yet
- Elder Law News & Notes Feb 2010 Number 67Document4 pagesElder Law News & Notes Feb 2010 Number 67Kyle EspinozaNo ratings yet
- One Size Fits All RevisedDocument39 pagesOne Size Fits All RevisedMark Norriel CajandabNo ratings yet
- Thesis On Physician Assisted DeathDocument5 pagesThesis On Physician Assisted Deathbnjkstgig100% (2)
- SawickiDocument55 pagesSawickiAdrian GuzmanNo ratings yet
- 43849-Article Text-41744-1-10-20090701Document4 pages43849-Article Text-41744-1-10-20090701Ahmed H. Ali ElbestaweyNo ratings yet
- Thesis Euthanasia PaperDocument5 pagesThesis Euthanasia Paperbsqkr4kn100% (2)
- Euthanasia Research Paper ThesisDocument6 pagesEuthanasia Research Paper Thesisczozyxakf100% (1)
- Caring, Curing, Coping: Nurse, Physician, and Patient RelationshipsFrom EverandCaring, Curing, Coping: Nurse, Physician, and Patient RelationshipsNo ratings yet
- The Healing Touch: Keeping the Doctor-Patient Relationship Alive Under Managed CareFrom EverandThe Healing Touch: Keeping the Doctor-Patient Relationship Alive Under Managed CareRating: 5 out of 5 stars5/5 (1)
- Currently Medical Ethics For PhysiciansDocument16 pagesCurrently Medical Ethics For PhysiciansOmarNo ratings yet
- Assignment 3 WORDDocument7 pagesAssignment 3 WORDJoanna KwiatkowskiNo ratings yet
- Inappropr Ther STDocument13 pagesInappropr Ther STRESCATEURNo ratings yet
- Yates-Doerr. Contando Cuerpos...Document18 pagesYates-Doerr. Contando Cuerpos...María BergeroNo ratings yet
- Ethics and The Legalization of Physician-Assisted Suicide - An American College of Physicians Position PaperDocument12 pagesEthics and The Legalization of Physician-Assisted Suicide - An American College of Physicians Position PaperRoberto López MataNo ratings yet
- Research Reportwiener1998Document12 pagesResearch Reportwiener1998maglangitmarvincNo ratings yet
- Euthanasia Research Paper Thesis StatementDocument4 pagesEuthanasia Research Paper Thesis Statementgbxqaf9v100% (2)
- Annotated Bibliography Medical EthicsDocument7 pagesAnnotated Bibliography Medical Ethicsapi-311220399No ratings yet
- Research Paper On Physician Assisted DeathDocument8 pagesResearch Paper On Physician Assisted Deathrsjpinynd100% (1)
- Profesionalismo MedicoDocument15 pagesProfesionalismo MedicoR4pT0r666No ratings yet
- First Draft 1 1302Document9 pagesFirst Draft 1 1302api-742824399No ratings yet
- Christopher Boorse (Auth.), James M. Humber, Robert F. Almeder ( - What Is Disease - (1997, Humana) (10.1007 - 978!1!59259-451-1) - Libgen - LiDocument358 pagesChristopher Boorse (Auth.), James M. Humber, Robert F. Almeder ( - What Is Disease - (1997, Humana) (10.1007 - 978!1!59259-451-1) - Libgen - LiLeon TrellesNo ratings yet
- Did The Doctor Do The Right Thing EditedDocument4 pagesDid The Doctor Do The Right Thing EditedmmhNo ratings yet
- Research Paper On Euthanasia FreeDocument6 pagesResearch Paper On Euthanasia Freeqbqkporhf100% (1)
- Against Euthanasia ThesisDocument4 pagesAgainst Euthanasia Thesispzblktgld100% (2)
- Questionable Cancer TherapiesDocument21 pagesQuestionable Cancer Therapiesvaxya100% (2)
- ÉTICA - Aula 1 - A Piece of My Mind Winners and Loosers JAMADocument2 pagesÉTICA - Aula 1 - A Piece of My Mind Winners and Loosers JAMAFelipe DiasNo ratings yet
- Student 1 Week 4 Discussion: Amanda Dubreuiel PostedDocument3 pagesStudent 1 Week 4 Discussion: Amanda Dubreuiel PostedAlpha RalakNo ratings yet
- Tutorial - ETHICS - 01-01-P1&2 - Introduction To Ethics and Biomedical Ethics & Ethical Issues in Doctor-Patient RelationshipsDocument43 pagesTutorial - ETHICS - 01-01-P1&2 - Introduction To Ethics and Biomedical Ethics & Ethical Issues in Doctor-Patient RelationshipsRenNo ratings yet
- Medical EthicsDocument6 pagesMedical Ethicsdobuol gorNo ratings yet
- Final Project 4 RewriteDocument11 pagesFinal Project 4 Rewriteapi-710396108No ratings yet
- Habit 5 PDFDocument2 pagesHabit 5 PDFPrashant PatilNo ratings yet
- Patient Rights: January 2016Document10 pagesPatient Rights: January 2016CharanNo ratings yet
- Refusal To Treat A PatientDocument4 pagesRefusal To Treat A Patientzwecker4458No ratings yet
- Medical EthicsDocument5 pagesMedical EthicsAdhyambo MakyaNo ratings yet
- Lecture Research EthicsDocument1 pageLecture Research EthicsAngel HeartNo ratings yet
- A Clear Case For Conscience in Healthcare Practice: Giles BirchleyDocument6 pagesA Clear Case For Conscience in Healthcare Practice: Giles BirchleyFuraya FuisaNo ratings yet
- Illich 1975 Medicalization of LiDocument6 pagesIllich 1975 Medicalization of Liaardvark62No ratings yet
- Professional Integrity and The Role of Medical Students in Professional Self-RegulationDocument5 pagesProfessional Integrity and The Role of Medical Students in Professional Self-RegulationMaría Jesús Carrión MansillaNo ratings yet
- Essay Lol Draft Haha M, EdicinesDocument3 pagesEssay Lol Draft Haha M, EdicinestheultimatetrovianNo ratings yet
- DNR and Medical FutilityDocument13 pagesDNR and Medical Futilityapi-216057141No ratings yet
- Duffy (A Minor) - V - National Maternity Hospital (2012) IEHC 354Document51 pagesDuffy (A Minor) - V - National Maternity Hospital (2012) IEHC 354SANDHYANo ratings yet
- Gillon (2003) Four ScenariosDocument3 pagesGillon (2003) Four ScenariosSANDHYANo ratings yet
- Quality of Dying in ICU Ways To Make It BetterDocument1 pageQuality of Dying in ICU Ways To Make It BetterSANDHYANo ratings yet
- Justice Baker (2017) A Matter of Life and DeathDocument9 pagesJustice Baker (2017) A Matter of Life and DeathSANDHYANo ratings yet
- Quebec UpdateDocument3 pagesQuebec UpdateSANDHYANo ratings yet
- HSE Guidance Re CPR and DNAR Decision Making During The COVID 19 PandemicDocument15 pagesHSE Guidance Re CPR and DNAR Decision Making During The COVID 19 PandemicSANDHYANo ratings yet
- HSE Background Note To Guidance On CPR and DNAR in Decision Making During The COVID 19 PandemicDocument1 pageHSE Background Note To Guidance On CPR and DNAR in Decision Making During The COVID 19 PandemicSANDHYANo ratings yet
- Editorial (2017) NEW FRONTIERS IN END-OF-LIFE ETHICSDocument2 pagesEditorial (2017) NEW FRONTIERS IN END-OF-LIFE ETHICSSANDHYANo ratings yet
- Powell T. Et Al (2017) A Good DeathDocument2 pagesPowell T. Et Al (2017) A Good DeathSANDHYANo ratings yet
- Madden Deirdre (2013) Is There A Right To A "Good Death"Document12 pagesMadden Deirdre (2013) Is There A Right To A "Good Death"SANDHYANo ratings yet
- DOH Procedural Values For Decision-Making in A PandemicDocument6 pagesDOH Procedural Values For Decision-Making in A PandemicSANDHYANo ratings yet
- White, B. Et Al (2017) The Role of Law in Decisions To Withhold AndlDocument8 pagesWhite, B. Et Al (2017) The Role of Law in Decisions To Withhold AndlSANDHYANo ratings yet
- AMA CEJF Statement Re Physician-Assisted Suicide A18-Ceja5Document8 pagesAMA CEJF Statement Re Physician-Assisted Suicide A18-Ceja5SANDHYANo ratings yet
- Rivera-Lopez E (2017) Is Medically Assisted Death A Special ObligationDocument7 pagesRivera-Lopez E (2017) Is Medically Assisted Death A Special ObligationSANDHYANo ratings yet
- DOH Ethical Framework For Decision Making in A PandemicDocument19 pagesDOH Ethical Framework For Decision Making in A PandemicSANDHYANo ratings yet
- Donnelly Sonya (2009) The Evolution of The Law On Assisted Suicide in The United Kingdom and The Possible ImplicationDocument15 pagesDonnelly Sonya (2009) The Evolution of The Law On Assisted Suicide in The United Kingdom and The Possible ImplicationSANDHYANo ratings yet
- DOH Ethical Considerations Relating To Lon-Term Residential Care Facilities in The Constext of COVID 19Document11 pagesDOH Ethical Considerations Relating To Lon-Term Residential Care Facilities in The Constext of COVID 19SANDHYANo ratings yet
- Dying at Home Cultural and Religious PreferencesDocument2 pagesDying at Home Cultural and Religious PreferencesSANDHYANo ratings yet
- Lung SoundsDocument6 pagesLung SoundsQuinn Madalang100% (1)
- American Medical Association - ICD-10-CM Documentation - Essential Charting Guidance To Support Medical Necessity 2019-American Medical Association (2018)Document1,229 pagesAmerican Medical Association - ICD-10-CM Documentation - Essential Charting Guidance To Support Medical Necessity 2019-American Medical Association (2018)johnharnsberry100% (1)
- The Five Eras of ChiropracticDocument8 pagesThe Five Eras of ChiropracticSam100% (1)
- The Impact of An Online Educational Game On Breast Cancer Awareness Among University Female Students, Malaysia: A Pilot StudyDocument11 pagesThe Impact of An Online Educational Game On Breast Cancer Awareness Among University Female Students, Malaysia: A Pilot StudySteve GannabanNo ratings yet
- lEGAL MEDICINE Sex CrimesDocument12 pageslEGAL MEDICINE Sex Crimesralna_florano1467No ratings yet
- Operan Jaga 5 Maret 2022Document29 pagesOperan Jaga 5 Maret 2022Rafaela LennyNo ratings yet
- EpisiotomyDocument3 pagesEpisiotomyAlexandra Chiriac AntonNo ratings yet
- Running Head: Fast Tracks in The Emergency Department 1Document11 pagesRunning Head: Fast Tracks in The Emergency Department 1FikriNo ratings yet
- On Catatonia Seizures and BradycardiaDocument1 pageOn Catatonia Seizures and BradycardiaFlorin TudoseNo ratings yet
- Thyroid Disorder Research PaperDocument5 pagesThyroid Disorder Research Paperapi-254922343No ratings yet
- Pharma Formulation Challenges & Innovations-2Document8 pagesPharma Formulation Challenges & Innovations-2Sundaram ShuklaNo ratings yet
- OncologyDocument3 pagesOncologyMichtropolisNo ratings yet
- A SepsisDocument5 pagesA SepsisAi KogaNo ratings yet
- Cues Nursing Diagnosis Scientific Reason Planning Intervention Rationale EvaluationDocument6 pagesCues Nursing Diagnosis Scientific Reason Planning Intervention Rationale EvaluationKatrina Ponce86% (7)
- 10 1080@1744666X 2019 1705785Document85 pages10 1080@1744666X 2019 1705785infectologia larazaNo ratings yet
- Basic Life Support Training Manualnew PDFDocument88 pagesBasic Life Support Training Manualnew PDFkekoho4589100% (1)
- Diagnostic CentreDocument14 pagesDiagnostic CentreJonas AsiaNo ratings yet
- NCP For Deficient Fluid VolumeDocument2 pagesNCP For Deficient Fluid VolumeRedwing_Dc_854758% (12)
- Assessments of Safe Medication Administration in Nursing EducationDocument12 pagesAssessments of Safe Medication Administration in Nursing EducationMichael AmandyNo ratings yet
- Drug SupplyDocument441 pagesDrug SupplyJIBRIL ALINo ratings yet
- Lympografi LainDocument39 pagesLympografi LainYuda FhunkshyangNo ratings yet
- Juan Dela Cruz, RRT: Personal InformationDocument3 pagesJuan Dela Cruz, RRT: Personal InformationShiela Leomo-VillaramaNo ratings yet
- 1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingDocument14 pages1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingKamx Mohammed100% (1)
- Perbandingan Dexa Dan MethylprednisoloneDocument2 pagesPerbandingan Dexa Dan MethylprednisoloneRai Jaine DarmantaNo ratings yet
- Male Infertility PDFDocument7 pagesMale Infertility PDFFaizatul ImanNo ratings yet
- Case Discussion Day 2 - MatulaDocument1 pageCase Discussion Day 2 - MatulaTRISHA MATULANo ratings yet
- Natara LandrauDocument2 pagesNatara Landraudmarkee4No ratings yet
- Headache Clinic CRFDocument12 pagesHeadache Clinic CRFNasirNo ratings yet