Download as pdf or txt
You might also like
- 05.11.02 Thyroid and ParathyroidDocument10 pages05.11.02 Thyroid and Parathyroidbo gum park100% (1)
- Immunology Paper 1 Past PapersDocument15 pagesImmunology Paper 1 Past PapersRehab KhaledNo ratings yet
- Moderator: MR S Chirkut /prof Hafejee Commentators:V Pillay / F Joyalemi 5 Sept 2015Document20 pagesModerator: MR S Chirkut /prof Hafejee Commentators:V Pillay / F Joyalemi 5 Sept 2015Kishan Naidu100% (1)
- 047 Endocrinology Physiology Parathyroid Gland CalcitoninDocument4 pages047 Endocrinology Physiology Parathyroid Gland Calcitoninیوسف رمضانNo ratings yet
- 13 Pharmacology Endocrine Part 1Document11 pages13 Pharmacology Endocrine Part 1ChrisNo ratings yet
- 4.1d - Pathology of The Pituitary - Nov.10 - Dr. GalangDocument4 pages4.1d - Pathology of The Pituitary - Nov.10 - Dr. GalangMiel Raphael AranillaNo ratings yet
- Surgical Management of Parathyroid Disease: Endocrine SurgeryDocument7 pagesSurgical Management of Parathyroid Disease: Endocrine SurgeryNiatazya Mumtaz SagitaNo ratings yet
- (SURG II) 6.03 Thyroid and Parathyroid - Dr. DizonDocument12 pages(SURG II) 6.03 Thyroid and Parathyroid - Dr. Dizonwgpyc8m8x5No ratings yet
- Lesson - 6.3 - Hypothalamus Putuitary Endocrine Part - 3 LmsDocument9 pagesLesson - 6.3 - Hypothalamus Putuitary Endocrine Part - 3 LmsJohanna MarieNo ratings yet
- Parathyroid Gland Clinical Chemistry (Lecture) : Lesson 8Document3 pagesParathyroid Gland Clinical Chemistry (Lecture) : Lesson 8Cherry Ann ColechaNo ratings yet
- Cc2 l7 Other GlandsDocument2 pagesCc2 l7 Other GlandsRose Denisse EstrellaNo ratings yet
- Surgery ParathyroidDocument11 pagesSurgery ParathyroidMATTHEW EARL MALUMAYNo ratings yet
- Describe and Explained Organs Belong To Endocrine SystemDocument4 pagesDescribe and Explained Organs Belong To Endocrine SystemnilaahanifahNo ratings yet
- Anatomy and Physiology of The Thyroid and Parathyroid GlandsDocument14 pagesAnatomy and Physiology of The Thyroid and Parathyroid GlandsSidiq AboobakerNo ratings yet
- Nihms 1613113Document20 pagesNihms 1613113João GasparNo ratings yet
- Pediatric Endocrine DisordersDocument15 pagesPediatric Endocrine Disorderscandiaangeltherese1318238No ratings yet
- Pituitary DiseasesDocument129 pagesPituitary Diseaseshrg79qzwc2No ratings yet
- Feline Hyperthyroidism 7586 ArticleDocument4 pagesFeline Hyperthyroidism 7586 ArticleAngel ValdiviaNo ratings yet
- Parathyroid Imaging PalestroDocument11 pagesParathyroid Imaging PalestroLadipo Temitope AyodejiNo ratings yet
- Guidelines For NHS Shortlist and InterviewDocument22 pagesGuidelines For NHS Shortlist and InterviewabduljajiNo ratings yet
- ThyroglobulinDocument17 pagesThyroglobulinfemunoz11No ratings yet
- PD22 HAP1 L04 FinalDocument49 pagesPD22 HAP1 L04 FinalKa Yan LAUNo ratings yet
- Thyroid Gland Clinical Chemistry 2 (Laboratory) : LessonDocument4 pagesThyroid Gland Clinical Chemistry 2 (Laboratory) : LessonCherry Ann ColechaNo ratings yet
- Tiroide RobbinsDocument24 pagesTiroide RobbinsAndrea PescosolidoNo ratings yet
- Clinical Chemistry 2 Lec - W10 - Introduction To Endocrine GlandsDocument3 pagesClinical Chemistry 2 Lec - W10 - Introduction To Endocrine GlandsEmalchris AcadsNo ratings yet
- CC2 Lec06Document8 pagesCC2 Lec06Haki TozakiNo ratings yet
- Adrenal Cortex DR - GomezDocument13 pagesAdrenal Cortex DR - Gomezvicbart11No ratings yet
- Cc1 Pituitary Bookbased SummaryDocument6 pagesCc1 Pituitary Bookbased SummaryPrecious EvangelistaNo ratings yet
- Path Endocrine OutlineDocument46 pagesPath Endocrine Outlineaya derweshNo ratings yet
- Thyroid GlandDocument9 pagesThyroid GlandZach ReyesNo ratings yet
- Group 3 - Endocrine System TRANSESDocument8 pagesGroup 3 - Endocrine System TRANSESategwen20No ratings yet
- Endocrine System: Organs and Their FunctionDocument61 pagesEndocrine System: Organs and Their FunctionSherifaNo ratings yet
- A&P - 2. The Hypothalamo-Pituitary Axis (9p) PDFDocument9 pagesA&P - 2. The Hypothalamo-Pituitary Axis (9p) PDFSreejith Jagal KishoreNo ratings yet
- Endocrinology Lectures 1 3 DR - LigonDocument14 pagesEndocrinology Lectures 1 3 DR - LigonJealine Marie BernabeNo ratings yet
- Bi2018 PDFDocument6 pagesBi2018 PDFgarrobosNo ratings yet
- Endocrine OctoberDocument70 pagesEndocrine OctoberMohamed FarahatNo ratings yet
- Endocrine Pancreas: Parathyroid TumoursDocument11 pagesEndocrine Pancreas: Parathyroid Tumoursshashi mittalNo ratings yet
- BI 232 Lab 13Document12 pagesBI 232 Lab 13Cj LinceNo ratings yet
- Introduction To EndocrinologyDocument8 pagesIntroduction To EndocrinologyAlecx LipatanNo ratings yet
- Ilovepdf Merged-2Document20 pagesIlovepdf Merged-2Alecx LipatanNo ratings yet
- Calcium Metabolism and Disorders ODocument14 pagesCalcium Metabolism and Disorders OvmdcabanillaNo ratings yet
- Chemical Coordination and Integration by - Dr. Sunita SaxenaDocument66 pagesChemical Coordination and Integration by - Dr. Sunita SaxenaDivya AgarawalNo ratings yet
- Midterms MSLectureDocument1 pageMidterms MSLectureMae Arra Lecobu-anNo ratings yet
- Enlargement of The Thyroid Gland: Embryology & Anatomy Surgical AnatomyDocument4 pagesEnlargement of The Thyroid Gland: Embryology & Anatomy Surgical AnatomyKiara GovenderNo ratings yet
- W4-15 Endocrine and Alimentary Layers of The Neck Lecture PDFDocument75 pagesW4-15 Endocrine and Alimentary Layers of The Neck Lecture PDFSAHIL AGARWALNo ratings yet
- Anatomy of ParathyroidDocument2 pagesAnatomy of ParathyroidNnanyelugo AdaobiNo ratings yet
- Endocrine System-1Document16 pagesEndocrine System-1Je Lan NieNo ratings yet
- TIRMODDocument66 pagesTIRMODYaniNo ratings yet
- Endocrinologie: Curs 2Document96 pagesEndocrinologie: Curs 2Ioana Maria RușețNo ratings yet
- Hypothyroidism by DR SarmaDocument124 pagesHypothyroidism by DR SarmaAjinkyaNo ratings yet
- Endocrine System HistologyDocument34 pagesEndocrine System HistologyAnjiZareerNo ratings yet
- Surgical Anatomy of The Parathyroid Glands - Uptodate 2022Document8 pagesSurgical Anatomy of The Parathyroid Glands - Uptodate 2022juanrangoneNo ratings yet
- Heparin: AnticoagulantsDocument8 pagesHeparin: AnticoagulantsThierd Cañete III100% (1)
- 1-7 BaileysDocument7 pages1-7 BaileysAura NirwanaNo ratings yet
- 1 s2.0 S0085253815518541 MainDocument6 pages1 s2.0 S0085253815518541 MainaripNo ratings yet
- Week 8 Thyroid DisordersDocument2 pagesWeek 8 Thyroid DisordersJiro MarianoNo ratings yet
- Parathyroid Gland, Anatom, Histology, and Physiology (A Short Review)Document7 pagesParathyroid Gland, Anatom, Histology, and Physiology (A Short Review)julioNo ratings yet
- ENDOCRINOLOGY Notes 2 PDFDocument131 pagesENDOCRINOLOGY Notes 2 PDFkomal pattabiNo ratings yet
- Endo ReviewerDocument5 pagesEndo ReviewerZIAN LABADIANo ratings yet
- Endo NotesDocument213 pagesEndo Notesdiko_nalNo ratings yet
- English For NursesDocument63 pagesEnglish For NursesDyah Elvi Meiedietik88% (17)
- Studi Kasus: Pemalsuan Daging Sapi Dengan Daging Babi Hutan Di Kota Bogor Lailatun Nida, Herwin Pisestyani, Chaerul BasriDocument10 pagesStudi Kasus: Pemalsuan Daging Sapi Dengan Daging Babi Hutan Di Kota Bogor Lailatun Nida, Herwin Pisestyani, Chaerul Basriclarentina aristawatiNo ratings yet
- Anti-Inflammatory Properties of BromelainDocument7 pagesAnti-Inflammatory Properties of BromelainKent AaronNo ratings yet
- Quiz No 3 Tle 10Document2 pagesQuiz No 3 Tle 10Israel Marquez100% (1)
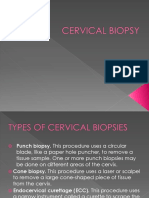
- Cervical BiopsyDocument17 pagesCervical BiopsyNestley TiongsonNo ratings yet
- Phlebolymphology: Vol 28 - No. 1 - 2021 - P1-36 No. 103Document39 pagesPhlebolymphology: Vol 28 - No. 1 - 2021 - P1-36 No. 103Jing CruzNo ratings yet
- Topodiagnostic & Electrophysiological Testing of Facial NerveDocument43 pagesTopodiagnostic & Electrophysiological Testing of Facial NerveAyesha Fayyaz100% (1)
- Siemens-Healthineers Mi Pet-Ct Biograph-Mct Product Brochure 1800000005821165Document20 pagesSiemens-Healthineers Mi Pet-Ct Biograph-Mct Product Brochure 1800000005821165Fando0% (1)
- Neu 2013 3197Document8 pagesNeu 2013 3197Sri MarniantiNo ratings yet
- Aloe Vera: A Potential Herb and Its Medicinal ImportanceDocument25 pagesAloe Vera: A Potential Herb and Its Medicinal ImportanceSusan Sitha Irma YuhanitaNo ratings yet
- Empr Prescriber's EditionDocument420 pagesEmpr Prescriber's EditionPatel Pratyk100% (1)
- Alginate TherapyDocument12 pagesAlginate TherapySMJ DRDNo ratings yet
- NAME: Neema Tamang Roll No:-20 Subject:-Surgery Assignment Topic:-Pneumothorax Faculty: HA 2Document9 pagesNAME: Neema Tamang Roll No:-20 Subject:-Surgery Assignment Topic:-Pneumothorax Faculty: HA 2Shreekrishna BudhathokiNo ratings yet
- Stroke LectureDocument23 pagesStroke LectureJayson RNNo ratings yet
- Guidelines Esh Practice BPM Gls jh2021Document10 pagesGuidelines Esh Practice BPM Gls jh2021Amira AlmutairiNo ratings yet
- Lymphatic SystemDocument25 pagesLymphatic Systemumar khanNo ratings yet
- Practice HPIDocument3 pagesPractice HPImedicalmatins100% (1)
- 757 - Penyakit Ginjal KronikDocument30 pages757 - Penyakit Ginjal KronikPujhi Meisya SoniaNo ratings yet
- Steroid Tapering and Supportive Treatment Guidance V1.0Document1 pageSteroid Tapering and Supportive Treatment Guidance V1.0yogaNo ratings yet
- Phang Mooi CMEDocument35 pagesPhang Mooi CMERaju AjmeraNo ratings yet
- Chain of Infection Content: 1. Chain of Infection. 2. Roles and Functions of The Nurse in The Chain of Infection. Chain of InfectionDocument3 pagesChain of Infection Content: 1. Chain of Infection. 2. Roles and Functions of The Nurse in The Chain of Infection. Chain of InfectionRespicio Christian Aejay G.No ratings yet
- Pathophysiology of Type 1 DiabetesDocument13 pagesPathophysiology of Type 1 DiabetesPelle MozzaNo ratings yet
- Visual ImpairmentDocument57 pagesVisual ImpairmentNavami KrishnaNo ratings yet
- 1nlrwmtqn4ac0etxquill3q3 3 4Document2 pages1nlrwmtqn4ac0etxquill3q3 3 4anmol kumarNo ratings yet
- Drugs Used in CPR - Lesson PlanDocument12 pagesDrugs Used in CPR - Lesson Planmonika makwana100% (2)
- MR Dieny & Yunri Jumat, 19 Nov 2021Document23 pagesMR Dieny & Yunri Jumat, 19 Nov 2021YunriNo ratings yet
- Man and MedicineDocument33 pagesMan and MedicineMithilesh Kumar yadavNo ratings yet
- Hyperthermia HandoutDocument1 pageHyperthermia Handoutapi-332422697No ratings yet
- Protein TherapeuticsDocument14 pagesProtein TherapeuticsSumanth Kumar ReddyNo ratings yet