Download as pdf or txt
You might also like
- CH 20 Manter Gatz S Essentials of Clinical Neuroanatomy and NeurophysiologyDocument27 pagesCH 20 Manter Gatz S Essentials of Clinical Neuroanatomy and Neurophysiologyasarg214100% (1)
- Management of Unsafe Type of Chronic Suppurative Otitis Media With Extracranial Complications at A Tertiary Care CenterDocument6 pagesManagement of Unsafe Type of Chronic Suppurative Otitis Media With Extracranial Complications at A Tertiary Care CenterLarasati Gilang Fuzi AstutiNo ratings yet
- Updated Management Strategies For Mastoiditis and PDFDocument7 pagesUpdated Management Strategies For Mastoiditis and PDFJr SparkNo ratings yet
- JOralMaxillofacRadiol8116-3384216 092402Document5 pagesJOralMaxillofacRadiol8116-3384216 092402Khaerani SaharNo ratings yet
- PDF Abses BezoldDocument5 pagesPDF Abses BezoldNiia D'girlsNo ratings yet
- Cholesterol GranulomaDocument2 pagesCholesterol GranulomazainabNo ratings yet
- 2021 Publication Case Report - Frontal MucoceleDocument3 pages2021 Publication Case Report - Frontal MucoceleMade RusmanaNo ratings yet
- Dent Update 2022 49 646-649Document4 pagesDent Update 2022 49 646-649Fatma HarmadaniNo ratings yet
- Lapsus Journal OriginalDocument5 pagesLapsus Journal Originalrozi piresNo ratings yet
- Case Bezold AbscessDocument3 pagesCase Bezold AbscessCarimaGhalieNo ratings yet
- Management of Chronic SuppurativeDocument8 pagesManagement of Chronic SuppurativeShebaTariganNo ratings yet
- 1 s2.0 S2210261220304284 MainDocument6 pages1 s2.0 S2210261220304284 MainNurul SalsabilaNo ratings yet
- Updated Management Strategies For Mastoiditis and Mastoid AbscessDocument6 pagesUpdated Management Strategies For Mastoiditis and Mastoid AbscessRonnyPujaKusumaNo ratings yet
- Article 6 2 6Document9 pagesArticle 6 2 6Gabriel LazarNo ratings yet
- ورقه بروف احمد سليمانDocument6 pagesورقه بروف احمد سليمانdr.m.m.yousifNo ratings yet
- Gejala Gangguan JiwaDocument8 pagesGejala Gangguan Jiwakevin stefanoNo ratings yet
- American Journal of Emergency Medicine: Case ReportDocument2 pagesAmerican Journal of Emergency Medicine: Case ReportqalbiNo ratings yet
- 10º-Adenoid Cystic Carcinoma of Alveolar Mucosa A Rare CaseDocument3 pages10º-Adenoid Cystic Carcinoma of Alveolar Mucosa A Rare Casecihece7650No ratings yet
- Adenomatoid Odontogenic Tumor, An Uncommon TumorDocument3 pagesAdenomatoid Odontogenic Tumor, An Uncommon TumorHarshavardhan ReddyNo ratings yet
- MRD 000606Document3 pagesMRD 000606Brianda Mass MenosNo ratings yet
- Desmoplastic Ameloblastoma A Case Report PDFDocument4 pagesDesmoplastic Ameloblastoma A Case Report PDF116 Bani GidelNo ratings yet
- Mastoiditis Case 1Document9 pagesMastoiditis Case 1fahrizan atjoNo ratings yet
- Ameloblastoma in Maxilla-Case of ReportDocument6 pagesAmeloblastoma in Maxilla-Case of Reportmatias112No ratings yet
- JDattaMegheInstMedSciUniv144426-5775248 160232Document3 pagesJDattaMegheInstMedSciUniv144426-5775248 160232srigiri surathNo ratings yet
- Referensi Lapsus No. 4Document4 pagesReferensi Lapsus No. 4citra annisa fitriNo ratings yet
- An Outstanding Ear - Otitis Externa With Cellulitis Versus MastoiditisDocument3 pagesAn Outstanding Ear - Otitis Externa With Cellulitis Versus MastoiditisandrianoawNo ratings yet
- Unicystic Ameloblastoma - Investigation Into An Enigma: IOSR Journal of Dental and Medical Sciences February 2020Document5 pagesUnicystic Ameloblastoma - Investigation Into An Enigma: IOSR Journal of Dental and Medical Sciences February 2020dr.filipcristian87No ratings yet
- AnnMaxillofacSurg91188-1852428 050844Document4 pagesAnnMaxillofacSurg91188-1852428 050844farihNo ratings yet
- Ijcmr 692 Jun 14Document2 pagesIjcmr 692 Jun 14Jeyachandran MariappanNo ratings yet
- CHRONICEARCH1Document8 pagesCHRONICEARCH1Fatih AbdullahNo ratings yet
- Medial Orbital Epidermoid Cyst: Case ReportDocument3 pagesMedial Orbital Epidermoid Cyst: Case ReportTeodorNo ratings yet
- Oral Liposarcoma in ElderlyDocument8 pagesOral Liposarcoma in ElderlyWinda KhosasiNo ratings yet
- Cholesteatoma of External Auditory CanalDocument5 pagesCholesteatoma of External Auditory CanallolNo ratings yet
- Aggressive Orthokeratinized Odontogenic CystDocument5 pagesAggressive Orthokeratinized Odontogenic CystSooraj SNo ratings yet
- Ijohns 2018081616134070Document5 pagesIjohns 2018081616134070alifaNo ratings yet
- Bilateral Ectopic Third Molars in Maxillary Sinus Associated With Dentigerous Cyst Identified With Ophthalmic, Nasal and Maxillary Complication: A Rare Case ReportDocument4 pagesBilateral Ectopic Third Molars in Maxillary Sinus Associated With Dentigerous Cyst Identified With Ophthalmic, Nasal and Maxillary Complication: A Rare Case ReporttasbetulNo ratings yet
- Angiomyolipoma of The Hard Palate: Clinical ReportDocument2 pagesAngiomyolipoma of The Hard Palate: Clinical ReportKezia Rachellea MustakimNo ratings yet
- Min 2018Document7 pagesMin 2018CindyNo ratings yet
- Osteo Blast OmaDocument5 pagesOsteo Blast OmamandetoperdiyuwanNo ratings yet
- A Case Report of Hydatid Disease in Long BoneDocument4 pagesA Case Report of Hydatid Disease in Long BoneVarun ArunagiriNo ratings yet
- Histopathological Insight of An Adenomatoid Odontogenic Lesion - A Cyst, Tumor or Hamartoma?Document6 pagesHistopathological Insight of An Adenomatoid Odontogenic Lesion - A Cyst, Tumor or Hamartoma?gunawan121982No ratings yet
- Calcifying Odontogenic Cyst With Atypica PDFDocument5 pagesCalcifying Odontogenic Cyst With Atypica PDFHerminaElenaNo ratings yet
- Streptococcus Constellatus: Causing Bony Destruction Secondary To Odontogenic Infection: Three Rare CasesDocument3 pagesStreptococcus Constellatus: Causing Bony Destruction Secondary To Odontogenic Infection: Three Rare CasesabdulrazaqNo ratings yet
- Oliver Syndrome With Extensive Aplasia Cutis Congenita A Case Report and Literature ReviewDocument11 pagesOliver Syndrome With Extensive Aplasia Cutis Congenita A Case Report and Literature ReviewInternational Journal of Innovative Science and Research Technology100% (1)
- Acute Mastoiditis With Temporomandibular Joint EffusionDocument2 pagesAcute Mastoiditis With Temporomandibular Joint EffusionWidyan Putra AnantawikramaNo ratings yet
- External CholesteatomDocument5 pagesExternal CholesteatomIvana SupitNo ratings yet
- Bony Ankylosis Mimicking Benign ChondromaDocument4 pagesBony Ankylosis Mimicking Benign ChondromaAnumita DekaNo ratings yet
- Whitish-Yellow Tumor On Its Characteristic Cut Surface: A Case Report of Congenital Granular Cell EpulisDocument2 pagesWhitish-Yellow Tumor On Its Characteristic Cut Surface: A Case Report of Congenital Granular Cell Epulisemmanuellagrace06No ratings yet
- Meningoencephalocele of The Temporal Bone-A Case Report: DR.B.V.N Muralidhar Reddy, DR K.V.V.RamjiDocument6 pagesMeningoencephalocele of The Temporal Bone-A Case Report: DR.B.V.N Muralidhar Reddy, DR K.V.V.RamjiNityaNo ratings yet
- Surgical Treatment of Central Giant Cells Lesions With Right HemimaxillectomyDocument5 pagesSurgical Treatment of Central Giant Cells Lesions With Right HemimaxillectomyIJAERS JOURNALNo ratings yet
- PDF 20230328 205355 0000Document1 pagePDF 20230328 205355 0000Durva JainNo ratings yet
- Pseudo-Ankylosis Caused by Osteoma of The Coronoid Process: Case Report - Tumors/CystsDocument3 pagesPseudo-Ankylosis Caused by Osteoma of The Coronoid Process: Case Report - Tumors/CystsSaurabh SatheNo ratings yet
- Lateral Periodontal Cysts Arising in Periapical Sites: A Report of Two CasesDocument5 pagesLateral Periodontal Cysts Arising in Periapical Sites: A Report of Two CasesTrianita DivaNo ratings yet
- BBRC Vol 14 No 04 2021-03Document4 pagesBBRC Vol 14 No 04 2021-03Dr Sharique AliNo ratings yet
- Journal of Oral and Maxillofacial Surgery, Medicine, and PathologyDocument7 pagesJournal of Oral and Maxillofacial Surgery, Medicine, and PathologyOMFS FKG UnimusNo ratings yet
- Otogenic Deep Neck Abscess: A Rare Complication of Cholesteatoma With Acute MastoiditisDocument6 pagesOtogenic Deep Neck Abscess: A Rare Complication of Cholesteatoma With Acute MastoiditisGondo RukemNo ratings yet
- Jnma 60 251 657Document4 pagesJnma 60 251 657Thai HuyNo ratings yet
- Cabt 12 I 3 P 330Document4 pagesCabt 12 I 3 P 330abeer alrofaeyNo ratings yet
- Jurnal SP KTK 2Document4 pagesJurnal SP KTK 2thasya sumerahNo ratings yet
- Complications in UveitisFrom EverandComplications in UveitisFrancesco PichiNo ratings yet
- Campy IJMMmanuscriptDocument7 pagesCampy IJMMmanuscriptAri Tri UtamiNo ratings yet
- Successful Treatment of Lichen Amyloidosis Using A Fixed Combination of Halobetasol-Propionate and Tazarotene LotionDocument2 pagesSuccessful Treatment of Lichen Amyloidosis Using A Fixed Combination of Halobetasol-Propionate and Tazarotene LotionAri Tri UtamiNo ratings yet
- Pakistan Journal of Health SciencesDocument5 pagesPakistan Journal of Health SciencesAri Tri UtamiNo ratings yet
- A Tympanic Membrane Cholesteatoma A Case Report and Literature Review - SCR 2019 5 123Document3 pagesA Tympanic Membrane Cholesteatoma A Case Report and Literature Review - SCR 2019 5 123Ari Tri UtamiNo ratings yet
- The Recent Outbreak of Acute Severe Hepatitis in Children of Unknown Origin What Is Known So Far Journal of HepatologyDocument6 pagesThe Recent Outbreak of Acute Severe Hepatitis in Children of Unknown Origin What Is Known So Far Journal of HepatologyAri Tri UtamiNo ratings yet
- Basic Principles of GrowthDocument29 pagesBasic Principles of GrowthMohsin HabibNo ratings yet
- Cranial Nerve ExaminationDocument6 pagesCranial Nerve ExaminationAlthea Aubrey AgbayaniNo ratings yet
- PD 11 12 Q1 0601 Developing Efficient Learning PSDocument30 pagesPD 11 12 Q1 0601 Developing Efficient Learning PSClifford TrijoNo ratings yet
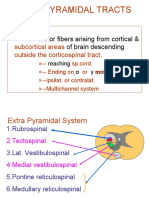
- Extrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingDocument21 pagesExtrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingAsfoor gake1No ratings yet
- Brain Left and Right Hemisphere PPT PresentationDocument10 pagesBrain Left and Right Hemisphere PPT PresentationAnushka Ridhi HiraNo ratings yet
- Neuroscience: For The Journal, See - "Brain Science" Redirects Here. For Other Aspects of Brain Science, See, ,, andDocument7 pagesNeuroscience: For The Journal, See - "Brain Science" Redirects Here. For Other Aspects of Brain Science, See, ,, andDexterNo ratings yet
- NCM 120 Procedural Checklist NEURODocument60 pagesNCM 120 Procedural Checklist NEUROLorenz Jude CańeteNo ratings yet
- Jack Hamm - Cartooning The Head & Figure - TextDocument131 pagesJack Hamm - Cartooning The Head & Figure - TextKumud BaliyanNo ratings yet
- BioPsych Handout 4 RESTRUCTUREDDocument7 pagesBioPsych Handout 4 RESTRUCTUREDMarial JavierNo ratings yet
- Le Fort FractureDocument22 pagesLe Fort FractureNikunj SorathiyaNo ratings yet
- Bibliography The Master and His EmissaryDocument68 pagesBibliography The Master and His Emissarymaja7979No ratings yet
- Mastoidectomy VS Tympanoplasty - A Conceptual Renaissance. Preamble To An Original Method of Mastoidectom PDFDocument5 pagesMastoidectomy VS Tympanoplasty - A Conceptual Renaissance. Preamble To An Original Method of Mastoidectom PDFPutu Reza Sandhya PratamaNo ratings yet
- ACFrOgCYzyAtlOdYv5jafLv-AubsWO2slT5n-CLAKbsxs37xlcq301vUs KfW9yPahBUJ3tJd68DH3Rf-H3JFeaJn BOx82c QRBoNJMxjZCNQIg-sy KVTI5Rx7OB93lfvgdTKZs1 3ImlTKcEhDocument37 pagesACFrOgCYzyAtlOdYv5jafLv-AubsWO2slT5n-CLAKbsxs37xlcq301vUs KfW9yPahBUJ3tJd68DH3Rf-H3JFeaJn BOx82c QRBoNJMxjZCNQIg-sy KVTI5Rx7OB93lfvgdTKZs1 3ImlTKcEhEmmanuel David PereaNo ratings yet
- Chapter 9 Injuries To The Head, Neck, and Face Student NotesDocument13 pagesChapter 9 Injuries To The Head, Neck, and Face Student Notesapi-287615830No ratings yet
- FULL Download Ebook PDF Fundamentals of Human Neuropsychology 7th Edition PDF EbookDocument41 pagesFULL Download Ebook PDF Fundamentals of Human Neuropsychology 7th Edition PDF Ebookjennifer.lawver532100% (51)
- Ujian Bab 1 Form 3: Stimuli and ResponsesDocument2 pagesUjian Bab 1 Form 3: Stimuli and Responsesalya sophiaNo ratings yet
- Imaging in OtorhinolaryngologyDocument38 pagesImaging in OtorhinolaryngologyNurin AlifatiNo ratings yet
- J.Surgical Approaches To Pineal Region Tumors.2001Document13 pagesJ.Surgical Approaches To Pineal Region Tumors.2001Kysy CodonNo ratings yet
- Brainpower: Complex Organ Controls Your Every Thought and MoveDocument19 pagesBrainpower: Complex Organ Controls Your Every Thought and Movelucille100% (2)
- Ent LuminaireDocument127 pagesEnt LuminaireFirdouse ShajiNo ratings yet
- ThyroidDocument7 pagesThyroidverawoNo ratings yet
- Histology: Neuron Cells Types and StructureDocument7 pagesHistology: Neuron Cells Types and StructureAli HayderNo ratings yet
- 7 The BrainDocument19 pages7 The BrainZidane ZizouNo ratings yet
- Human Anatomy Head and Neck 8Th Edition BD Chaurasia Online Ebook Texxtbook Full Chapter PDFDocument69 pagesHuman Anatomy Head and Neck 8Th Edition BD Chaurasia Online Ebook Texxtbook Full Chapter PDFalfredo.slone379100% (9)
- Color Atlas of BrainDocument8 pagesColor Atlas of BrainMWNo ratings yet
- Contrastive Analysis of Idioms Expressing "Body Parts" in The English, Kyrgyz and Russian LanguagesDocument63 pagesContrastive Analysis of Idioms Expressing "Body Parts" in The English, Kyrgyz and Russian LanguagesMirlan Chekirov100% (10)
- Buccinator Myomucosal Flap-1Document6 pagesBuccinator Myomucosal Flap-1JamesNo ratings yet
- Ent Rajeev Dhawan Full NotesDocument80 pagesEnt Rajeev Dhawan Full Notesrandomuploader053No ratings yet
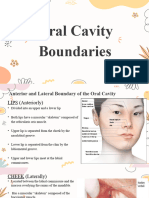
- Oral Cavity BoundariesDocument8 pagesOral Cavity BoundariesLean Edrielle BillonesNo ratings yet