Download as pdf or txt
You might also like
- Tinnitus Cure Guide: The Ultimate Tinnitus Miracle Cure & Relief GuideFrom EverandTinnitus Cure Guide: The Ultimate Tinnitus Miracle Cure & Relief GuideRating: 3.5 out of 5 stars3.5/5 (9)
- AP Psych All Concept MapsDocument18 pagesAP Psych All Concept MapsNathan Hudson100% (14)
- A0bea-Naturalscience03 Cam Term1 TestDocument4 pagesA0bea-Naturalscience03 Cam Term1 TestMARTA100% (3)
- Ent Hearing Tests, Vestibular TestsDocument13 pagesEnt Hearing Tests, Vestibular TestsSuleman MuhammadNo ratings yet
- Ear Canal Granuloma: Presentator: Anggoro Eka Raditya Moderator: Dr. Yayan MitayaniDocument76 pagesEar Canal Granuloma: Presentator: Anggoro Eka Raditya Moderator: Dr. Yayan MitayaniAldy Bima100% (1)
- Thomas Gold (Auth.) - The Deep Hot Biosphere - The Myth of Fossil Fuels-Copernicus (1999) PDFDocument248 pagesThomas Gold (Auth.) - The Deep Hot Biosphere - The Myth of Fossil Fuels-Copernicus (1999) PDFRaúl Bolmaro100% (2)
- Family Case Analysis 2Document98 pagesFamily Case Analysis 2Carl Elexer Cuyugan Ano50% (2)
- (Ugo Fisch, Thomas Linder) Temporal Bone Dissectio PDFDocument66 pages(Ugo Fisch, Thomas Linder) Temporal Bone Dissectio PDFTiara Audina Darmawan100% (1)
- TinnitusDocument10 pagesTinnitusGissell GarciaNo ratings yet
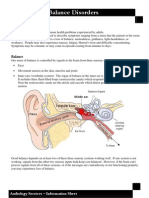
- Dizziness and Balance DisordersDocument4 pagesDizziness and Balance DisordersEcaterina ChiriacNo ratings yet
- Document 32Document3 pagesDocument 32Play ListNo ratings yet
- Vertigo and DizzinessDocument14 pagesVertigo and Dizzinessa7mad thunaibatNo ratings yet
- Vestibularneuritis: John C. Goddard,, Jose N. FayadDocument5 pagesVestibularneuritis: John C. Goddard,, Jose N. Fayaddarmayanti ibnuNo ratings yet
- Etiology and Diagnosis of Tinnitus - UpToDateDocument18 pagesEtiology and Diagnosis of Tinnitus - UpToDateAdri NolascoNo ratings yet
- Doctor'S View On Vertigo Causes: Charles Patrick Davis, MD, PHDDocument14 pagesDoctor'S View On Vertigo Causes: Charles Patrick Davis, MD, PHDFransisca FebrianaNo ratings yet
- Tinnitus 1Document36 pagesTinnitus 1Wael ShamyNo ratings yet
- What Is VertigoDocument12 pagesWhat Is VertigoManayu WidaswariNo ratings yet
- What Is Cervical SpondylosisDocument7 pagesWhat Is Cervical SpondylosisBibhash MishraNo ratings yet
- Mineire'sDocument16 pagesMineire'sShaykh Evangelista BacualNo ratings yet
- Low BackDocument7 pagesLow BackMuhammad FahmyNo ratings yet
- Vestibular Neutitis & Labyrinthitis PDFDocument6 pagesVestibular Neutitis & Labyrinthitis PDFFika Khulma SofiaNo ratings yet
- 21 DizzinessDocument2 pages21 DizzinesscrichmdNo ratings yet
- Types of VertigoDocument3 pagesTypes of VertigoAkanksha PashineyNo ratings yet
- Jawahar Navodaya Vidyalaya Kagal KolhapurDocument27 pagesJawahar Navodaya Vidyalaya Kagal KolhapurSujay NirmaleNo ratings yet
- DR Zuraida Zainun MSC (Medical Audiology), MD Senior Lecturer Audiology Prgramme School of Helth Sciences Universiti Sains MalaysiaDocument43 pagesDR Zuraida Zainun MSC (Medical Audiology), MD Senior Lecturer Audiology Prgramme School of Helth Sciences Universiti Sains MalaysiaHaniym ZawawiNo ratings yet
- NR 509 Midterm PPDocument76 pagesNR 509 Midterm PPLou EscobarNo ratings yet
- Vertigo: Dizziness Is A Symptom Which Can Describe Many Different SensationsDocument8 pagesVertigo: Dizziness Is A Symptom Which Can Describe Many Different SensationsSri Sri WahNo ratings yet
- Evaluation of The PatientDocument13 pagesEvaluation of The PatientHannah LeiNo ratings yet
- Tinnitus 101 What You Absolutely Need To Know About TinnitusDocument13 pagesTinnitus 101 What You Absolutely Need To Know About TinnitusivarnorNo ratings yet
- Tinnitus 2Document35 pagesTinnitus 2Wael ShamyNo ratings yet
- A Positive Response To Ankylosing Spondylitis: Guidebook For PatientsDocument18 pagesA Positive Response To Ankylosing Spondylitis: Guidebook For PatientsdipanshuroyNo ratings yet
- Vdocuments - MX - Biology Investigatory Project by Rajni PriyaDocument25 pagesVdocuments - MX - Biology Investigatory Project by Rajni PriyaRoshan AbbasNo ratings yet
- Hiperakusis Dan TinnitusDocument11 pagesHiperakusis Dan TinnitusavininditaNo ratings yet
- Final Myofascial PainDocument3 pagesFinal Myofascial PainAamir BugtiNo ratings yet
- Hearing Disorders and Audiogram InterpretationDocument27 pagesHearing Disorders and Audiogram InterpretationGaluhNo ratings yet
- 12 Critical QuestionsDocument2 pages12 Critical QuestionsramopavelNo ratings yet
- Initial Evaluation of VertigoDocument11 pagesInitial Evaluation of VertigoIraNo ratings yet
- Neck and Low Back PainDocument128 pagesNeck and Low Back Painralu_balajNo ratings yet
- Trouble Getting A Diagnosis - 72Document5 pagesTrouble Getting A Diagnosis - 72Cristian DobrescuNo ratings yet
- Case Study Title PDFDocument20 pagesCase Study Title PDFZerimar Dela CruzNo ratings yet
- Dizziness: Presented By: Rawan Shaher Al-AssafDocument47 pagesDizziness: Presented By: Rawan Shaher Al-AssafRazan Shaher Al Assaf100% (1)
- Vertigo and DizzinessDocument50 pagesVertigo and DizzinessRyanIndraSaputraNo ratings yet
- TinnitusDocument11 pagesTinnitusChad ViajarNo ratings yet
- Welgamp OLADocument14 pagesWelgamp OLASofiaNo ratings yet
- LBP 2Document12 pagesLBP 2Attika DiniNo ratings yet
- Hal 1-2Document4 pagesHal 1-2frita1986No ratings yet
- "Approach To The Patient With Vertigo" "Evaluation of Syncope in Adults"Document8 pages"Approach To The Patient With Vertigo" "Evaluation of Syncope in Adults"Fila DelviaNo ratings yet
- Vestibular Neuritis HandoutDocument3 pagesVestibular Neuritis HandoutPrisilia QurratuAiniNo ratings yet
- Cervical SpondylosisDocument8 pagesCervical SpondylosisRicha AgarwallaNo ratings yet
- Vertigo and Its Management PDFDocument21 pagesVertigo and Its Management PDFNitya KrishnaNo ratings yet
- Neuro EquilibriumDocument6 pagesNeuro EquilibriumNeuro EquilibriumNo ratings yet
- Syndromes of The Head Anc Neck of Dental Origin - Pain Caused by Mandibular DysfunctionDocument11 pagesSyndromes of The Head Anc Neck of Dental Origin - Pain Caused by Mandibular DysfunctionGuoyiNo ratings yet
- Observation of The Patient When They Walk in - : HistoryDocument19 pagesObservation of The Patient When They Walk in - : Historyajaykumar soddalaNo ratings yet
- The Breakthrough Back Pain Healing and Relief Plan: The book that unlocked the secrets of back pain care, sciatica pain relief naturally via diet, exercises & understanding the mind-body connectionFrom EverandThe Breakthrough Back Pain Healing and Relief Plan: The book that unlocked the secrets of back pain care, sciatica pain relief naturally via diet, exercises & understanding the mind-body connectionNo ratings yet
- Case 8 VertigoDocument10 pagesCase 8 VertigoElizabeth HoNo ratings yet
- Peripheral VertigoDocument5 pagesPeripheral VertigoAlin CiubotaruNo ratings yet
- VertigoDocument41 pagesVertigoAnonymous 4Oe8clFY100% (1)
- LBP EmedicineDocument15 pagesLBP EmedicinenararyasriNo ratings yet
- Vertigo: A Review of Common Peripheral and Central Vestibular DisordersDocument7 pagesVertigo: A Review of Common Peripheral and Central Vestibular DisordersPutra ImanullahNo ratings yet
- Neck Pain: D - P. P. M, A P, D - PDocument9 pagesNeck Pain: D - P. P. M, A P, D - PRichaNo ratings yet
- Medical Approach To Dizzy PatientsDocument52 pagesMedical Approach To Dizzy PatientsYudith Kattiarni Aisyah, MDNo ratings yet
- Text Book Reading "Posttraumatic Balance Disorder": Pembimbing Dr. Untung Gunarto, Sp. SDocument11 pagesText Book Reading "Posttraumatic Balance Disorder": Pembimbing Dr. Untung Gunarto, Sp. SsilvanaNo ratings yet
- Síndrome Vestibular Periférico: Revista de Medicina de La Universidad de Navarra January 2003Document14 pagesSíndrome Vestibular Periférico: Revista de Medicina de La Universidad de Navarra January 2003Nataly Fernanda100% (1)
- Otosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOtosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Ear Eczema 22 06 15Document6 pagesEar Eczema 22 06 15wahyunhyNo ratings yet
- Nice For Hearing LossDocument17 pagesNice For Hearing LossMaram AbdullahNo ratings yet
- Ent Miniosce Group A3Document25 pagesEnt Miniosce Group A3frabziNo ratings yet
- The Book of Healing Mind Body and Soul Recent UpdateDocument567 pagesThe Book of Healing Mind Body and Soul Recent UpdateYoram RazNo ratings yet
- Ear, Nose and Throat (Ent) AssessmentDocument6 pagesEar, Nose and Throat (Ent) AssessmentObama kindaNo ratings yet
- Cerumen ImpactionDocument6 pagesCerumen ImpactionNin DuskNo ratings yet
- NICU Care Plan On Birth AsphyxiaDocument17 pagesNICU Care Plan On Birth AsphyxiaKhushbu KatariaNo ratings yet
- Colour Atlas of Mouth, Throat and Ear Disorders in Children 1985Document84 pagesColour Atlas of Mouth, Throat and Ear Disorders in Children 1985Vitaliy ZhevachevskyyNo ratings yet
- Science Class 8 Sound and HearingDocument4 pagesScience Class 8 Sound and Hearingtripti aggarwalNo ratings yet
- Second Lesson Plan Final 1Document8 pagesSecond Lesson Plan Final 1Lhai DeliNo ratings yet
- OM001-14 Otowave 102 Operating Manual PDFDocument50 pagesOM001-14 Otowave 102 Operating Manual PDFFaazaNo ratings yet
- Sound Lesson 4Document11 pagesSound Lesson 4api-283310252No ratings yet
- Otic Instillation and IrrigationDocument22 pagesOtic Instillation and IrrigationSilpa Jose TNo ratings yet
- All Checklists Compiled UpdatedDocument30 pagesAll Checklists Compiled UpdatedSnow WhiteNo ratings yet
- Imaging in Otosclerosis: A Pictorial ReviewDocument8 pagesImaging in Otosclerosis: A Pictorial ReviewChlo14No ratings yet
- Neric 711 CouplerDocument30 pagesNeric 711 Coupleranandr50100% (1)
- The Activity and Co-Activity of The Senses by Dr. Hermann PoppelbaumDocument2 pagesThe Activity and Co-Activity of The Senses by Dr. Hermann PoppelbaumGucciGrumpsNo ratings yet
- Vestibular Questionnaire: Fill in The Blank SpacesDocument2 pagesVestibular Questionnaire: Fill in The Blank SpacesyaddNo ratings yet
- Earmolds ManualDocument97 pagesEarmolds ManualdawksNo ratings yet
- Product Data: Head and Torso Simulator Types 4128 C and 4128 D Handset Positioner For HATS Type 4606Document8 pagesProduct Data: Head and Torso Simulator Types 4128 C and 4128 D Handset Positioner For HATS Type 4606GilbertoAndresDuarteNo ratings yet
- OtosclerosisDocument3 pagesOtosclerosisSuryadi P. Dwipayana, Ida BgsNo ratings yet
- 3rd QTRDocument5 pages3rd QTRAple RigorNo ratings yet
- Operation Manual: Impedance Audiometer AT235/AT235hDocument117 pagesOperation Manual: Impedance Audiometer AT235/AT235hCarlos Eduardo Mendez AlvarezNo ratings yet