Download as doc, pdf, or txt
You might also like
- Cl-Molec Cap Assay Check ListDocument74 pagesCl-Molec Cap Assay Check ListAndreína Gabriela Sánchez González0% (1)
- Lab Policies Sysmex XS 1000i Procedure Lab 1501 PDFDocument26 pagesLab Policies Sysmex XS 1000i Procedure Lab 1501 PDFRana RoyNo ratings yet
- Urinalysis and Body Fluids for Cls & MltFrom EverandUrinalysis and Body Fluids for Cls & MltNo ratings yet
- 2.2.4. Eye Health Clinical Audit - Indicators List: Section One: Primary Eye Care ChecksDocument2 pages2.2.4. Eye Health Clinical Audit - Indicators List: Section One: Primary Eye Care ChecksCynthia Jaramillo Machuca100% (1)
- Acute Renal FailureDocument34 pagesAcute Renal Failureaibaloca67% (9)
- 2.5 Antibody ScreeningDocument5 pages2.5 Antibody ScreeningBALAJINo ratings yet
- 6.1.3 Quality Control of Blood ComponentsDocument4 pages6.1.3 Quality Control of Blood ComponentsBALAJINo ratings yet
- Blood Tube Collection GuideDocument365 pagesBlood Tube Collection GuideFeliciadlT100% (1)
- QC-7 Hematology Westgard Rules in Good Performance LaboratoryDocument38 pagesQC-7 Hematology Westgard Rules in Good Performance LaboratoryWita100% (1)
- Clinical1 Quality Control - 10Document36 pagesClinical1 Quality Control - 10Khansa Qureshi100% (1)
- RBCDocument66 pagesRBCFarah mansourNo ratings yet
- Criteria For Specimen AcceptabilityDocument3 pagesCriteria For Specimen AcceptabilityFatwa100% (1)
- Quality Control2Document32 pagesQuality Control2Mustafa KhandgawiNo ratings yet
- Use of Fresh Blood For Quality Control: Erythrocyte Sedimentation RateDocument6 pagesUse of Fresh Blood For Quality Control: Erythrocyte Sedimentation RateTriana AmaliaNo ratings yet
- Clia & Cap Regulatory TrainingDocument23 pagesClia & Cap Regulatory TrainingWilliam David HommelNo ratings yet
- Chapter 14 - Routine and Point of Care Testing in HematologyDocument10 pagesChapter 14 - Routine and Point of Care Testing in HematologyNathaniel Sim100% (1)
- Hematology PDFDocument85 pagesHematology PDFammarNo ratings yet
- 01 Introduction To Lab StandardsDocument23 pages01 Introduction To Lab Standardsyousrazeidan1979No ratings yet
- AABB AccreditationDocument8 pagesAABB Accreditationgabababa100% (1)
- MANI Quality Control in Hematology AnalysersDocument65 pagesMANI Quality Control in Hematology Analyserscandiddreams100% (1)
- Levey Jennings & Westgard RulesDocument31 pagesLevey Jennings & Westgard RulesMyra Kiriyuu100% (2)
- D Dimer Preanalytical Analytical Postanalytical Variables and Clinical ApplicationsDocument31 pagesD Dimer Preanalytical Analytical Postanalytical Variables and Clinical ApplicationsfaizmundzirNo ratings yet
- Hematology Week 1 CBCDocument4 pagesHematology Week 1 CBCMICHELLE RAPELONo ratings yet
- ISO 15189 - 2012 Technical RequirementsDocument104 pagesISO 15189 - 2012 Technical RequirementsAhmed AdemNo ratings yet
- Laboratory Turnaround TimeDocument17 pagesLaboratory Turnaround TimeNicole HoNo ratings yet
- Enseval Examination of Bacterial Contamination in Blood Components Biomerieux PDFDocument21 pagesEnseval Examination of Bacterial Contamination in Blood Components Biomerieux PDFCik KahadiNo ratings yet
- Primary Sample Collection Manual GD-QSPMDocument51 pagesPrimary Sample Collection Manual GD-QSPMLalit Surykant Chavan100% (1)
- CLS Internship ManualDocument216 pagesCLS Internship ManualtaghamdNo ratings yet
- BOC Study Guide: The MostDocument17 pagesBOC Study Guide: The MostDeanne LambanNo ratings yet
- The Peripheral Blood FilmDocument5 pagesThe Peripheral Blood FilmanggaririnNo ratings yet
- Lab Math Lec (Prelims)Document7 pagesLab Math Lec (Prelims)Merra VenzuelaNo ratings yet
- Laboratory Hematology CriteriaDocument7 pagesLaboratory Hematology CriteriaRosNo ratings yet
- Automation in Clinical ChemistryDocument28 pagesAutomation in Clinical ChemistryJoyce VitalNo ratings yet
- Procedures/Guidelines For The Microbiology LaboratoryDocument61 pagesProcedures/Guidelines For The Microbiology LaboratorySadao MatsumotoNo ratings yet
- Sysmex SEED 4 2013 Automated Haematology Sample Interferences Flagging and Results Interpretation - Part 1 enDocument8 pagesSysmex SEED 4 2013 Automated Haematology Sample Interferences Flagging and Results Interpretation - Part 1 enPieter Du Toit-Enslin50% (2)
- IQCPDocument1 pageIQCPPrabhu Selvaraj100% (1)
- CRP Versus ESRDocument12 pagesCRP Versus ESRLuke LauNo ratings yet
- Common Medical Laboratory Errors PDFDocument2 pagesCommon Medical Laboratory Errors PDFRosalyn100% (1)
- Flow Cell Wash Kit Exp wsh004 WFC - 9120 - v1 - Revb - 08dec2020 MinionDocument9 pagesFlow Cell Wash Kit Exp wsh004 WFC - 9120 - v1 - Revb - 08dec2020 MinionErikk DangNo ratings yet
- GP33 Manual ClsiDocument3 pagesGP33 Manual ClsiGonzalez ArturoNo ratings yet
- Blood Bak Process MapDocument1 pageBlood Bak Process MapspanwzNo ratings yet
- Transfusion Practice Guidelines For Clinic and Laboratory PersonnelDocument98 pagesTransfusion Practice Guidelines For Clinic and Laboratory PersonnelZhayreal Zaki100% (1)
- HematologySlides2020 FullSizeDocument812 pagesHematologySlides2020 FullSizeNikos SyrigosNo ratings yet
- Urinalysis and Body Fluid CollectionsDocument48 pagesUrinalysis and Body Fluid CollectionsladydianamacNo ratings yet
- IH Hospital Wide QI Master Spreadsheet 2023Document115 pagesIH Hospital Wide QI Master Spreadsheet 2023Uranchimeg MyagmarchimedNo ratings yet
- Blood Bank SOP 2015Document52 pagesBlood Bank SOP 2015ddophlaak labdeptNo ratings yet
- Laboratory Testing Turn-Around Times PolicyDocument5 pagesLaboratory Testing Turn-Around Times PolicyGHL AdaroNo ratings yet
- CLIAbrochure8 PDFDocument12 pagesCLIAbrochure8 PDFAlexandr Chuvakov100% (1)
- 300-5208 B BFM Clsi SopDocument23 pages300-5208 B BFM Clsi SopnjujjnjnjjnnjNo ratings yet
- III. Quality Assessment & ManagementDocument3 pagesIII. Quality Assessment & ManagementDee Gee100% (1)
- Laboratory Quality ControlDocument63 pagesLaboratory Quality Control"DocAxi" Maximo B Axibal Jr MD FPSPNo ratings yet
- Mycology SOP 2nd Ed 2019Document144 pagesMycology SOP 2nd Ed 2019Deepak Muralidhara NadigNo ratings yet
- Platlets DisorderDocument177 pagesPlatlets DisorderFatimah A Al-dawoodNo ratings yet
- Job Description:: Phlebotomists DutiesDocument7 pagesJob Description:: Phlebotomists DutiesRajeev PareekNo ratings yet
- Delta Checks For Random Error Detection in Hematology TestsDocument8 pagesDelta Checks For Random Error Detection in Hematology Testsimran ahmed siddiquiNo ratings yet
- 03 - SOP Clinical PathologyDocument88 pages03 - SOP Clinical PathologyKailash PrajapatNo ratings yet
- Prof. Joy V. Lorin-Picar Davao Del Norte State College: New Visayas, Panabo CityDocument91 pagesProf. Joy V. Lorin-Picar Davao Del Norte State College: New Visayas, Panabo CityJeLo ReaNdelarNo ratings yet
- KKHL c6 SP 03 Sop For Iqc and Eqa Final 1Document23 pagesKKHL c6 SP 03 Sop For Iqc and Eqa Final 1GABULA MIKENo ratings yet
- Quality Control 2023 +CLIA 2024Document125 pagesQuality Control 2023 +CLIA 2024bashira khalidyNo ratings yet
- Quality Assurance in Hematology Group 11Document51 pagesQuality Assurance in Hematology Group 11Mandy A. DelfinNo ratings yet
- Systemic MycosesDocument4 pagesSystemic MycosesdeblackaNo ratings yet
- Thyroid Testing Using RaiDocument8 pagesThyroid Testing Using RaideblackaNo ratings yet
- Investigation of Haemolytic Transfusion ReactionsDocument2 pagesInvestigation of Haemolytic Transfusion ReactionsdeblackaNo ratings yet
- SOP For StoolDocument4 pagesSOP For StooldeblackaNo ratings yet
- Disease Prevention and ControlDocument36 pagesDisease Prevention and ControldeblackaNo ratings yet
- Sexually Transmitted InfectionsDocument1 pageSexually Transmitted InfectionsdeblackaNo ratings yet
- Group 7 AssignmentDocument30 pagesGroup 7 AssignmentdeblackaNo ratings yet
- A Comparative Study of European Rare DisDocument7 pagesA Comparative Study of European Rare DisFabiana RaynalNo ratings yet
- Neurology StrokeDocument1,531 pagesNeurology StrokelguerreroNo ratings yet
- A Study About The Relocation of Badjao Community in Totolan 4Document17 pagesA Study About The Relocation of Badjao Community in Totolan 4welpNo ratings yet
- National Programme For Prevention and Control of CancerDocument18 pagesNational Programme For Prevention and Control of CancerPrabhakaran AranganathanNo ratings yet
- The Antifungal Activity of OnionDocument28 pagesThe Antifungal Activity of OnionJeanetteEoniceRodriguez100% (1)
- Nomenklatur IBS Edit THTDocument291 pagesNomenklatur IBS Edit THTriezki_pattikratonMDNo ratings yet
- Total Knee ReplacementDocument49 pagesTotal Knee Replacementefancoolhand09No ratings yet
- Practice Exam Kit For The Mblex: Your Test StatisticsDocument24 pagesPractice Exam Kit For The Mblex: Your Test StatisticslevarjaoNo ratings yet
- Diet TiroidDocument6 pagesDiet TiroidAhmad Umar AfNo ratings yet
- Related Teenshealth Links: Health Problems SeriesDocument13 pagesRelated Teenshealth Links: Health Problems SeriesMario BadayosNo ratings yet
- Ehrlichiosis and Anaplasmosis: Zoonotic Species: ImportanceDocument14 pagesEhrlichiosis and Anaplasmosis: Zoonotic Species: Importancerodrigo lopez jimenezNo ratings yet
- Gingiva Diseases Of89Document3 pagesGingiva Diseases Of89محمد العراقيNo ratings yet
- Engineering Design An Introduction 2nd Edition Karsnitz Test Bank Full Chapter PDFDocument36 pagesEngineering Design An Introduction 2nd Edition Karsnitz Test Bank Full Chapter PDFRobertFordicwr100% (17)
- Antimicrobial Prescribing Delafloxacin For Acute Bacterial Skin and Skin Structure Infections PDF 1158232915141Document6 pagesAntimicrobial Prescribing Delafloxacin For Acute Bacterial Skin and Skin Structure Infections PDF 1158232915141carlettino7No ratings yet
- 9D-NLS Features and Warranty (2021)Document10 pages9D-NLS Features and Warranty (2021)Danutz ChirilaNo ratings yet
- Revised Hema Outline Aug 2, 2020Document9 pagesRevised Hema Outline Aug 2, 2020Edna Uneta RoblesNo ratings yet
- Final Test FK - 1 - Ang - 2019 - Juli 2020Document3 pagesFinal Test FK - 1 - Ang - 2019 - Juli 2020CahayaNo ratings yet
- Case No 6Document3 pagesCase No 6Valenzuela, Ivy Lyn B.No ratings yet
- Citation, Title, and Abstract ScreeningDocument2 pagesCitation, Title, and Abstract ScreeningsdfdsfNo ratings yet
- Inroduction To AmputationDocument67 pagesInroduction To AmputationAlfred JacksonNo ratings yet
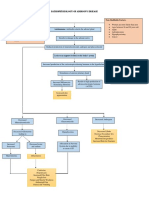
- Pathophysiology of Addison'S Disease: Non-Modifiable Factors: Modifiable FactorsDocument2 pagesPathophysiology of Addison'S Disease: Non-Modifiable Factors: Modifiable FactorsHanna NocumNo ratings yet
- Leopard Gecko Diseases and CareDocument5 pagesLeopard Gecko Diseases and CareUrielNo ratings yet
- Schizophrenia: Diagnosis and SymptomsDocument11 pagesSchizophrenia: Diagnosis and SymptomsLuas PelegriniNo ratings yet
- Brain SpectDocument10 pagesBrain SpectKevinNo ratings yet
- OSCES 5e MMSDocument125 pagesOSCES 5e MMSFlórian Jefferson100% (1)
- Jurnal Stroke HemoragikDocument10 pagesJurnal Stroke HemoragikAri StefanusNo ratings yet
- Script TBDocument10 pagesScript TBMelrhean GraceNo ratings yet
- Nine Effective Home Remedies For EaracheDocument1 pageNine Effective Home Remedies For EarachekaralyntNo ratings yet