Download as pdf or txt
You might also like
- 2-Day Diabetes Diet: Diet Just 2 Days a Week and Dodge Type 2 DiabetesFrom Everand2-Day Diabetes Diet: Diet Just 2 Days a Week and Dodge Type 2 DiabetesRating: 3 out of 5 stars3/5 (1)
- Alternate Day Fasting and Endurance Exercise Combine To Reduce Body Weight and Favorably Alter Plasma Lipids in Obese HumansDocument10 pagesAlternate Day Fasting and Endurance Exercise Combine To Reduce Body Weight and Favorably Alter Plasma Lipids in Obese HumansAndres CaceresNo ratings yet
- Effects of 8-Hour Time Restricted Feeding On Body Weight and Metabolic Disease Risk Factors in Obese Adults A Pilot Study, 2018Document9 pagesEffects of 8-Hour Time Restricted Feeding On Body Weight and Metabolic Disease Risk Factors in Obese Adults A Pilot Study, 2018Dana MuresanNo ratings yet
- Intermittent Fasting Combined With Calorie Restriction Is Effective For Weight Loss and Cardio-Protection in Obese WomenDocument9 pagesIntermittent Fasting Combined With Calorie Restriction Is Effective For Weight Loss and Cardio-Protection in Obese Womenpriya1832No ratings yet
- Gabel Et Al. 2020Document29 pagesGabel Et Al. 2020nutrijudemetrioNo ratings yet
- 2022 - JCEM - Metabolic Efficacy of Time-Restricted Eating in AdultsDocument14 pages2022 - JCEM - Metabolic Efficacy of Time-Restricted Eating in AdultsLuiz Fernando Fonseca VieiraNo ratings yet
- HHS Public AccessDocument18 pagesHHS Public AccessAllegra BNo ratings yet
- Restricao Diaria Ou Intermitente PDFDocument9 pagesRestricao Diaria Ou Intermitente PDFAna Carolina Basso MorenoNo ratings yet
- JI X HDL PESQUISA BIBLIOGRAFICADocument8 pagesJI X HDL PESQUISA BIBLIOGRAFICAJúlia MunizNo ratings yet
- A Randomized Trial of A Low-Carbohydrate Diet For Obesity - NEJMDocument16 pagesA Randomized Trial of A Low-Carbohydrate Diet For Obesity - NEJMMateo PeychauxNo ratings yet
- Dietary JournalDocument8 pagesDietary JournalRachmania BudiatiNo ratings yet
- Effects of A Meal Replacement On Body CompositionDocument10 pagesEffects of A Meal Replacement On Body CompositionGiffariNo ratings yet
- Is Time-Restricted Eating (8/16) Beneficial For Body Weight and Metabolism of Obese and Overweight Adults? A Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocument14 pagesIs Time-Restricted Eating (8/16) Beneficial For Body Weight and Metabolism of Obese and Overweight Adults? A Systematic Review and Meta-Analysis of Randomized Controlled TrialsEvan LauNo ratings yet
- Lin Et Al 2023 Time Restricted Eating Without Calorie Counting For Weight Loss in A Racially Diverse PopulationDocument12 pagesLin Et Al 2023 Time Restricted Eating Without Calorie Counting For Weight Loss in A Racially Diverse PopulationSarah VõNo ratings yet
- Jcem 1617Document7 pagesJcem 1617Sebastian GiovanniniNo ratings yet
- Intermittent Fast Timing AARAGON AND SCHOENFELDDocument6 pagesIntermittent Fast Timing AARAGON AND SCHOENFELDahmed noomanNo ratings yet
- Diet Review Intermittent Fasting Weight Loss PDFDocument9 pagesDiet Review Intermittent Fasting Weight Loss PDFKenyatta BushNo ratings yet
- Obesity - 2017 - Anton - Flipping The Metabolic Switch Understanding and Applying The Health Benefits of FastingDocument15 pagesObesity - 2017 - Anton - Flipping The Metabolic Switch Understanding and Applying The Health Benefits of FastingEckyThumpNo ratings yet
- Effect of A Low-Glycaemic Index - Low-Fat - High Protein Diet On The Atherogenic Metabolic Risk Profile of Abdominally Obese MenDocument12 pagesEffect of A Low-Glycaemic Index - Low-Fat - High Protein Diet On The Atherogenic Metabolic Risk Profile of Abdominally Obese MenAmida OaxacaNo ratings yet
- 2014 - Johansson - Neovius - Hemmingsson - Effects of Anti Obesity Drugs Diet and Exercise On Weight LossDocument10 pages2014 - Johansson - Neovius - Hemmingsson - Effects of Anti Obesity Drugs Diet and Exercise On Weight LossPatricioNo ratings yet
- Carbohydrates Research-5Document8 pagesCarbohydrates Research-5api-466416222No ratings yet
- Dieta CetogênicaDocument11 pagesDieta CetogênicaSilvanaGomesNo ratings yet
- Ntrs 513-Final PaperDocument8 pagesNtrs 513-Final Paperapi-203339953No ratings yet
- Esfahani Et al-2011-IUBMB Life PDFDocument7 pagesEsfahani Et al-2011-IUBMB Life PDFLisiane PerinNo ratings yet
- Intermittent Fasting Vs Daily Calorie Restriction For Type 2 Diabetes Prevention: A Review of Human FindingsDocument10 pagesIntermittent Fasting Vs Daily Calorie Restriction For Type 2 Diabetes Prevention: A Review of Human FindingsAmry Irsyada YusufNo ratings yet
- Contemporary Clinical Trials: SciencedirectDocument11 pagesContemporary Clinical Trials: SciencedirectYusuf YNo ratings yet
- Artigo - Metabolic ImpactsDocument11 pagesArtigo - Metabolic ImpactsRaissa Porta da Cruz RaissaNo ratings yet
- PDF Philippine-CONSENSUS-STATEMENT-FINAL-BJMeditsDocument21 pagesPDF Philippine-CONSENSUS-STATEMENT-FINAL-BJMeditsElly JoyNo ratings yet
- Low Carb StudyDocument15 pagesLow Carb StudycphommalNo ratings yet
- Tinsley 2018Document8 pagesTinsley 2018mpharmqaNo ratings yet
- AbacateDocument9 pagesAbacateMaria SantosNo ratings yet
- Randomized Controlled Trial of The Medifast 5 & 1 Plan For Weight LossDocument8 pagesRandomized Controlled Trial of The Medifast 5 & 1 Plan For Weight Losszainab asalNo ratings yet
- Estudio Controlado de Fideos Instantaneos y Avena InstantaneaDocument8 pagesEstudio Controlado de Fideos Instantaneos y Avena InstantaneaChristian Cornejo RiveraNo ratings yet
- Weight Loss Meta AnalysisDocument6 pagesWeight Loss Meta AnalysisYusuf YNo ratings yet
- Postul Intermitent (Intermittent Fasting) Pentru SlabireDocument3 pagesPostul Intermitent (Intermittent Fasting) Pentru SlabireSeb SaabNo ratings yet
- Calorie Restriction With or Without Exercise On Insulin Sensitivity Beta Cell Functions Ectopic LipidDocument8 pagesCalorie Restriction With or Without Exercise On Insulin Sensitivity Beta Cell Functions Ectopic Lipidadibahfauzi85No ratings yet
- 1 s2.0 S0026049511003404 MainDocument8 pages1 s2.0 S0026049511003404 MainFrankis De Jesus Vanegas RomeroNo ratings yet
- NutrientsDocument17 pagesNutrientsNenden ApriliyantiNo ratings yet
- Micronutrieint Loss ObeseDocument10 pagesMicronutrieint Loss ObeseYazen JoudehNo ratings yet
- Diabetes MellitusDocument8 pagesDiabetes Mellitusi_anitaNo ratings yet
- SerumDocument6 pagesSerumdindaNo ratings yet
- Out 11Document7 pagesOut 11AnamNo ratings yet
- Ajcn 109553Document7 pagesAjcn 109553VincentNo ratings yet
- Popular Diets: A Scientific Review: Executive SummaryDocument5 pagesPopular Diets: A Scientific Review: Executive SummaryKarina ValenzuelaNo ratings yet
- The Effect of Intermittent Ener - Michelle HarvieDocument14 pagesThe Effect of Intermittent Ener - Michelle Harvierdomingues.acarvalhoNo ratings yet
- 5 Studies On The Paleo Diet - Does It Work?Document26 pages5 Studies On The Paleo Diet - Does It Work?Alpesh JadhavNo ratings yet
- Comparison of High-Fat and High-Protein Diets With A High-Carbohydrate Diet in Insulin-Resistant Obese WomenDocument9 pagesComparison of High-Fat and High-Protein Diets With A High-Carbohydrate Diet in Insulin-Resistant Obese WomenDanielle AliceNo ratings yet
- Does A Ketogenic Diet Have Beneficial Effects On Quality of Life, Physical Activity or Biomarkers in PatientsDocument10 pagesDoes A Ketogenic Diet Have Beneficial Effects On Quality of Life, Physical Activity or Biomarkers in PatientsMNo ratings yet
- Weight-Loss Diets For The Prevention and Treatment of ObesityDocument3 pagesWeight-Loss Diets For The Prevention and Treatment of ObesityRupita SitanggangNo ratings yet
- Ketogenic DietsDocument23 pagesKetogenic DietsNorma Edith López DíazGuerreroNo ratings yet
- Terapia Comportamental Da ObesidadeDocument16 pagesTerapia Comportamental Da ObesidadeVanessa MaiaNo ratings yet
- Effects of Intermittent and Continuous Calorie Restriction On Body Weight and Metabolism Over 50 WK: A Randomized Controlled TrialDocument13 pagesEffects of Intermittent and Continuous Calorie Restriction On Body Weight and Metabolism Over 50 WK: A Randomized Controlled TrialSarah OctaviaNo ratings yet
- Moderate CarbohydrateDocument9 pagesModerate CarbohydrateAndrea TorrealdayNo ratings yet
- Review of Low-Carb Vs High-Carb DietsDocument15 pagesReview of Low-Carb Vs High-Carb Dietswtbliss100% (8)
- Dietary TX of Obesity 08Document14 pagesDietary TX of Obesity 08chigolinNo ratings yet
- Increased Consumption of Dairy Foods and Protein During Diet - and Exercise-Induced Weight Loss Promotes Fat Mass Loss and Lean Mass Gain in Overweight and Obese Premenopausal WomenDocument9 pagesIncreased Consumption of Dairy Foods and Protein During Diet - and Exercise-Induced Weight Loss Promotes Fat Mass Loss and Lean Mass Gain in Overweight and Obese Premenopausal Womenines.queiros.nutricionistaNo ratings yet
- Research Open Access: Michelle Wien, Keiji Oda and Joan SabatéDocument9 pagesResearch Open Access: Michelle Wien, Keiji Oda and Joan SabatéAnonymous SvlxqQeiNo ratings yet
- Artículo Inglés 2024Document11 pagesArtículo Inglés 2024021220072No ratings yet
- Wiliam Yancy PDFDocument7 pagesWiliam Yancy PDFDeaz Fazzaura PutriNo ratings yet
- PIIS2589537023000172Document12 pagesPIIS2589537023000172Gerry FonziNo ratings yet
- Is Obesity or Adiposity-Based Chronic Disease Curable: The Set Point Theory, The Environment, and Second-Generation MedicationsDocument9 pagesIs Obesity or Adiposity-Based Chronic Disease Curable: The Set Point Theory, The Environment, and Second-Generation MedicationsGerry FonziNo ratings yet
- PIIS2666524722003226Document9 pagesPIIS2666524722003226Gerry FonziNo ratings yet
- The Christmas Holidays Are Immediately Followed by A Period of HypercholesterolemiaDocument7 pagesThe Christmas Holidays Are Immediately Followed by A Period of HypercholesterolemiaGerry FonziNo ratings yet
- AHA Advisory OKs Eating Cholesterol in ModerationDocument3 pagesAHA Advisory OKs Eating Cholesterol in ModerationGerry FonziNo ratings yet
- 8 Traits of A Successful Medical Practice: MGMA 2018Document2 pages8 Traits of A Successful Medical Practice: MGMA 2018Gerry FonziNo ratings yet
- Type of Diabetes in Pregnancy Impacts Risk For ChildDocument2 pagesType of Diabetes in Pregnancy Impacts Risk For ChildGerry FonziNo ratings yet
- Hypothesis Testing - Chi Squared TestDocument16 pagesHypothesis Testing - Chi Squared TestEdwin Mudzamiri04No ratings yet
- Dissertation Uni Heidelberg MedizinDocument4 pagesDissertation Uni Heidelberg MedizinWriteMyPaperOneDayCanada100% (1)
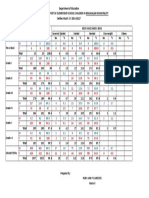
- Physical Fitness Score Card - Latest 2021Document1 pagePhysical Fitness Score Card - Latest 2021Kyla M. ManaloNo ratings yet
- Priya B.Sc. NursingDocument41 pagesPriya B.Sc. NursingVigneshMuchiNo ratings yet
- EOT2 G12 Gen Boys HSDocument3 pagesEOT2 G12 Gen Boys HSHasan ShkoukaniNo ratings yet
- Presentation ObesityDocument70 pagesPresentation ObesityIbrahim Mahmoud AliNo ratings yet
- Glycemic IndexDocument5 pagesGlycemic IndexftmtanNo ratings yet
- The PURPLE SEAL 6-06-11 ISBN 9780974172415 International Edition E-Mail AttachmentDocument185 pagesThe PURPLE SEAL 6-06-11 ISBN 9780974172415 International Edition E-Mail AttachmentGeorge Washington Singleton IIINo ratings yet
- Guideline Book 2017Document204 pagesGuideline Book 2017tonirian99No ratings yet
- Nutri & Diet MidtermDocument4 pagesNutri & Diet MidtermronronNo ratings yet
- 1310475807binder1Document39 pages1310475807binder1CoolerAdsNo ratings yet
- Nutritional Assessment Form For Outdoor PatientsDocument2 pagesNutritional Assessment Form For Outdoor PatientsAnas siddiqui0% (1)
- Essay Competition (Eng)Document2 pagesEssay Competition (Eng)Mazwin AjaatNo ratings yet
- Childhood Overweight On The Rise in LAC - 2023 ReportDocument54 pagesChildhood Overweight On The Rise in LAC - 2023 Reportceles83No ratings yet
- Nutritional Status TemplateDocument1 pageNutritional Status TemplateShangkiee Amora-TamborNo ratings yet
- GSK Sotrovimab Fact Sheet For HCP 12222021Document34 pagesGSK Sotrovimab Fact Sheet For HCP 12222021Jillian SmithNo ratings yet
- Coronary Heart DiseaseDocument18 pagesCoronary Heart DiseasesamjaisheelNo ratings yet
- 663-Article Text-1457-2-10-20210208Document11 pages663-Article Text-1457-2-10-20210208masadrag98No ratings yet
- Advocacy MemoDocument2 pagesAdvocacy Memoapi-370731005No ratings yet
- Behavioral Aspects of Overweight and ObesityDocument9 pagesBehavioral Aspects of Overweight and ObesitypeterNo ratings yet
- Introduction To NutritionDocument206 pagesIntroduction To NutritionMompati LetsweletseNo ratings yet
- Healthmedicinet I 2017 1Document676 pagesHealthmedicinet I 2017 1tuni santeNo ratings yet
- Peer Reviewed Article - The Effect of Fast Food Restaurants On Obesity and Weight GainDocument6 pagesPeer Reviewed Article - The Effect of Fast Food Restaurants On Obesity and Weight Gainapi-710695274No ratings yet
- Antidiabetic Effect of Ipomoea Batatas in Normal ADocument11 pagesAntidiabetic Effect of Ipomoea Batatas in Normal AFara AzzahraNo ratings yet
- (Download PDF) Medical Nutrition Therapy A Case Study Approach 5Th Edition PDF Full Chapter PDFDocument42 pages(Download PDF) Medical Nutrition Therapy A Case Study Approach 5Th Edition PDF Full Chapter PDFzippelwudil100% (10)
- Skipping Breakfast Introduction 1 2Document38 pagesSkipping Breakfast Introduction 1 2Adrian PanlicanNo ratings yet
- Listening: The Biggest Loser Is A RealityDocument18 pagesListening: The Biggest Loser Is A RealityMaria Adelaide Maia TorresNo ratings yet
- EXTENDED ESSAY ASSINGMENT (PS102) S11195702 Romanu SavitaDocument10 pagesEXTENDED ESSAY ASSINGMENT (PS102) S11195702 Romanu SavitaSavita RomanuNo ratings yet
- Earthworms Supplemented Poultry Feed AsDocument4 pagesEarthworms Supplemented Poultry Feed AsShah NawazNo ratings yet
- 7TPE1 Physical Fitness TestDocument2 pages7TPE1 Physical Fitness TestErrol AlejandroNo ratings yet