Download as docx, pdf, or txt
You might also like
- Confined Space Rescue Plan: Reason For EntryDocument4 pagesConfined Space Rescue Plan: Reason For EntrybalasubramaniamNo ratings yet
- INCIDENT INVESTIGATION REPORT Hadeed Shaikh 500080705Document2 pagesINCIDENT INVESTIGATION REPORT Hadeed Shaikh 500080705hadeed shaikh100% (1)
- JAPL-F-HE-001-Weekly Grader Inspection ChecklistDocument2 pagesJAPL-F-HE-001-Weekly Grader Inspection ChecklistAli Hassan100% (1)
- 675Document2 pages675Rameese MuhammedNo ratings yet
- Safety Incident Report FormDocument3 pagesSafety Incident Report FormDiego MatillaNo ratings yet
- Monthly Mass Meeting Agenda + Invitation 12 PageDocument1 pageMonthly Mass Meeting Agenda + Invitation 12 PageamitNo ratings yet
- JSO Cable Drum (02 Sept.'07)Document2 pagesJSO Cable Drum (02 Sept.'07)Francis Enriquez TanNo ratings yet
- HiraDocument18 pagesHiraPanchdev KumarNo ratings yet
- Concrete WorkDocument3 pagesConcrete WorkAbdul Ghaffar100% (1)
- Incident RegisterDocument1 pageIncident RegisterJagadeesh GunupuruNo ratings yet
- Water Proofing JSADocument9 pagesWater Proofing JSARamNo ratings yet
- Safety Weekly Stats Report Upto 02-Oct - 2021Document1 pageSafety Weekly Stats Report Upto 02-Oct - 2021Sabre Alam100% (1)
- Heat Stress Awareness Drill June 2022Document18 pagesHeat Stress Awareness Drill June 2022Subbu AbuNo ratings yet
- HR HR TEM007 GEN ALL Visitor Induction Rev1.0Document2 pagesHR HR TEM007 GEN ALL Visitor Induction Rev1.0Doni TriatmojoNo ratings yet
- HIRA RCC Work (3) Approed by ClientDocument11 pagesHIRA RCC Work (3) Approed by ClientHARSHADNo ratings yet
- Report of An Injury or Dangerous Occurrence: Part A Part CDocument2 pagesReport of An Injury or Dangerous Occurrence: Part A Part CVeronica Navarro CorbiNo ratings yet
- Hirac (Small Power Installation)Document4 pagesHirac (Small Power Installation)tanaNo ratings yet
- Annexure 9 - Declaration by The Subcontractor For HSE ComplianceDocument1 pageAnnexure 9 - Declaration by The Subcontractor For HSE ComplianceShamim Mahmudur RahmanNo ratings yet
- Heat Stress Management PlanDocument4 pagesHeat Stress Management Planthennarasu100% (1)
- Daily Safety Report TemplateDocument1 pageDaily Safety Report TemplateMarkNo ratings yet
- 2.8c Risk Assessment - 001 Site Survey of Land Rev. July 2019Document7 pages2.8c Risk Assessment - 001 Site Survey of Land Rev. July 2019sadafnoor997No ratings yet
- Plant EQUIPMENT Check SheetDocument1 pagePlant EQUIPMENT Check SheetSparrow Green StudiosNo ratings yet
- Qcs 2010 Section 11 Part 1.7 Regulatory Document - FIRE and FLAMMABLEDocument75 pagesQcs 2010 Section 11 Part 1.7 Regulatory Document - FIRE and FLAMMABLEbryanpastor106100% (1)
- Steel Shield Temporary Fencing Risk Assessment and Method Statement For ErectionDocument7 pagesSteel Shield Temporary Fencing Risk Assessment and Method Statement For ErectionIrfan Prima AldiNo ratings yet
- Night Work PermitDocument3 pagesNight Work PermitArmando AballeNo ratings yet
- PR 15 Hira Procedure Bim& Tim r1Document17 pagesPR 15 Hira Procedure Bim& Tim r1Purna Chandra BaruaNo ratings yet
- Lessons Learnt - Trench CollapseDocument2 pagesLessons Learnt - Trench CollapseEhab SaadNo ratings yet
- Contractor Safety Induction Attendance SheetDocument2 pagesContractor Safety Induction Attendance SheetBalogun Isaac100% (1)
- Incident Investigation ReportDocument2 pagesIncident Investigation Reportsudeesh kumarNo ratings yet
- Environmental, Health and Safety Risks AnalysisDocument2 pagesEnvironmental, Health and Safety Risks AnalysisKrishna Patil100% (1)
- Presentation: "Emergency Preparedness"Document63 pagesPresentation: "Emergency Preparedness"vidhya sagarNo ratings yet
- Risk Assessment - PPE - ClothingDocument2 pagesRisk Assessment - PPE - Clothingbearingworks123No ratings yet
- Nebosh Igc 3 Report-1-1 - 1Document17 pagesNebosh Igc 3 Report-1-1 - 1Muhammad ShahzaibNo ratings yet
- Factory Act Form No. 32Document1 pageFactory Act Form No. 32Gopala krishnaNo ratings yet
- Brazing (Oxygen and Acetylene)Document6 pagesBrazing (Oxygen and Acetylene)My Zain100% (1)
- RA - (LPG System)Document26 pagesRA - (LPG System)Md ShahinNo ratings yet
- Risk Assessment of Manual HandlingDocument2 pagesRisk Assessment of Manual HandlingMAB AliNo ratings yet
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky Bis100% (1)
- Emergency Response Plan Final NotesDocument6 pagesEmergency Response Plan Final Notesviren thakkar100% (1)
- Fire Prevention PolicyDocument4 pagesFire Prevention Policymuhammadkashik100% (1)
- SOP Traffic ManagementDocument9 pagesSOP Traffic ManagementSyed AhmadNo ratings yet
- JHA For To Carryout Activities During Unloading of Product From Ship Rev00Document4 pagesJHA For To Carryout Activities During Unloading of Product From Ship Rev00Sreekumar100% (1)
- ACCIDENT and INCIDENT INVESTIGATION PROCEDUREDocument16 pagesACCIDENT and INCIDENT INVESTIGATION PROCEDUREvladNo ratings yet
- Task Risk AssesmentDocument3 pagesTask Risk Assesmentafsalkareem100% (1)
- Emergency Response Team: Reporting Flow ChartDocument1 pageEmergency Response Team: Reporting Flow Chartmohamadhakim.19789100% (1)
- 09-Safety Training Attendance SheetDocument1 page09-Safety Training Attendance SheetSainu Kalathingal0% (1)
- Safety Observation Formate - 01Document3 pagesSafety Observation Formate - 01Peter LuvisNo ratings yet
- Emergency Response Team Organizational Chart: ERT RolesDocument4 pagesEmergency Response Team Organizational Chart: ERT RolesoshbsgtorregosaNo ratings yet
- Risk Assessment For Blinding Concrete - 01Document6 pagesRisk Assessment For Blinding Concrete - 01Bulent Ak100% (1)
- JSEA-ICS-004 Cable Laying and PullingDocument13 pagesJSEA-ICS-004 Cable Laying and PullingJayson EscamillanNo ratings yet
- F.hse.07 Work PermitDocument4 pagesF.hse.07 Work PermitMOJIBNo ratings yet
- Mock Drill ReportDocument2 pagesMock Drill ReportSudamBeheraNo ratings yet
- OHS-PR-09-03-F02 HIRA - 003 Temporary Perimeter Fencing Rev. 2021Document7 pagesOHS-PR-09-03-F02 HIRA - 003 Temporary Perimeter Fencing Rev. 2021MuhammadAsimMuneerNo ratings yet
- Project EHS KPI - 24 Agustus 2013Document1 pageProject EHS KPI - 24 Agustus 2013Crystin Rotua Hasmi PanjaitanNo ratings yet
- August Ventures PVT LTD Format For Induction TrainingDocument1 pageAugust Ventures PVT LTD Format For Induction TrainingDeepak GNo ratings yet
- SWMS Loading and Unloading Vehicles WHS.127 V002.1Document18 pagesSWMS Loading and Unloading Vehicles WHS.127 V002.1Amit BhattNo ratings yet
- Accident Incident Report FormDocument3 pagesAccident Incident Report FormTuan Nguyen100% (1)
- Agenda National Safety Day CelebrationDocument3 pagesAgenda National Safety Day CelebrationDhilip AnNo ratings yet
- Laboratory Incident Report FormDocument1 pageLaboratory Incident Report FormnatalieshirleyNo ratings yet
- 6 Accident Incident Report FormatDocument2 pages6 Accident Incident Report Formatmadhav jadeNo ratings yet
- JSA-Batching-Plant - Doc HPGR SMDDocument2 pagesJSA-Batching-Plant - Doc HPGR SMDMalefane Cortez TlatlaneNo ratings yet
- HSE Documentation INDEXDocument2 pagesHSE Documentation INDEXMalefane Cortez TlatlaneNo ratings yet
- Weekly Stats Calculator 2023 - Week 00Document1 pageWeekly Stats Calculator 2023 - Week 00Malefane Cortez TlatlaneNo ratings yet
- DAILY HSE Officer's Work PlanDocument2 pagesDAILY HSE Officer's Work PlanMalefane Cortez TlatlaneNo ratings yet
- 0824 Nhvim Heavy Vehicle Trailer Inspection ChecklistDocument1 page0824 Nhvim Heavy Vehicle Trailer Inspection ChecklistMalefane Cortez TlatlaneNo ratings yet
- DSTIDocument3 pagesDSTIMalefane Cortez TlatlaneNo ratings yet
- HSE Multiple KPIs Visualization in ExcelDocument2 pagesHSE Multiple KPIs Visualization in ExcelMalefane Cortez TlatlaneNo ratings yet
- Jobs Safety Analysis or Steps of Job Safety Analysis or Example With Scenario Work at HeightDocument7 pagesJobs Safety Analysis or Steps of Job Safety Analysis or Example With Scenario Work at HeightMalefane Cortez TlatlaneNo ratings yet
- Risk Assessment TemplateDocument2 pagesRisk Assessment TemplateMalefane Cortez TlatlaneNo ratings yet
- 07 Hazard Identification RegisterDocument9 pages07 Hazard Identification RegisterMalefane Cortez TlatlaneNo ratings yet
- HSE Operational Control Procedure For Disposal of SewageDocument1 pageHSE Operational Control Procedure For Disposal of SewageMalefane Cortez TlatlaneNo ratings yet
- Excavation Inspection ChecklistDocument3 pagesExcavation Inspection ChecklistMalefane Cortez TlatlaneNo ratings yet
- September Dinaledi Compliance Audits Report 6Document37 pagesSeptember Dinaledi Compliance Audits Report 6Malefane Cortez TlatlaneNo ratings yet
- E13 Stormwater Management PlanDocument24 pagesE13 Stormwater Management PlanMalefane Cortez TlatlaneNo ratings yet
- Annexure 4-10 Pre and Post Construction SITE Survey or Inspection Rev 01Document1 pageAnnexure 4-10 Pre and Post Construction SITE Survey or Inspection Rev 01Malefane Cortez TlatlaneNo ratings yet
- Notification of Construction WorkDocument2 pagesNotification of Construction WorkMalefane Cortez TlatlaneNo ratings yet
- Accident or Incident RegisterDocument2 pagesAccident or Incident RegisterMalefane Cortez TlatlaneNo ratings yet
- Monthly Emp Compliance Monitoring and Evaluation ChecklistDocument9 pagesMonthly Emp Compliance Monitoring and Evaluation ChecklistMalefane Cortez TlatlaneNo ratings yet
- MDRZA011 DoDocument21 pagesMDRZA011 DoMalefane Cortez TlatlaneNo ratings yet
- Storm Water Management & Rehabilitation PlanDocument50 pagesStorm Water Management & Rehabilitation PlanMalefane Cortez TlatlaneNo ratings yet
- Dozer Checklist: DATEDocument1 pageDozer Checklist: DATEMalefane Cortez TlatlaneNo ratings yet
- Method Statements Waste Management Service Specific SpecificationDocument14 pagesMethod Statements Waste Management Service Specific SpecificationMalefane Cortez TlatlaneNo ratings yet
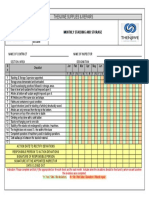
- Monthly Stacking & Storage - 0Document1 pageMonthly Stacking & Storage - 0Malefane Cortez TlatlaneNo ratings yet
- Excavator Daily Inspection ChecklistDocument1 pageExcavator Daily Inspection ChecklistMalefane Cortez TlatlaneNo ratings yet
- Front Loader Daily InspectionDocument1 pageFront Loader Daily InspectionMalefane Cortez TlatlaneNo ratings yet
- Coal Nswec Mtarthur BlastManagementPlanFINALApprovedDocument69 pagesCoal Nswec Mtarthur BlastManagementPlanFINALApprovedMalefane Cortez TlatlaneNo ratings yet
- Dump Truck ChecklistDocument1 pageDump Truck ChecklistMalefane Cortez TlatlaneNo ratings yet