Download as pdf or txt
You might also like
- Is Endodontic Re-Treatment Mandatory For Every Relatively Old Temporary Restoration?: A Narrative ReviewDocument7 pagesIs Endodontic Re-Treatment Mandatory For Every Relatively Old Temporary Restoration?: A Narrative ReviewARTNo ratings yet
- Complications in Surgical Removal of Impacted Mandibular Third Molars in Relation To Ap Design: Clinical and Statistical EvaluationsDocument10 pagesComplications in Surgical Removal of Impacted Mandibular Third Molars in Relation To Ap Design: Clinical and Statistical Evaluationswaleed MagidNo ratings yet
- Peri-Implant Health, Peri-Implant Mucositis, and Peri-Implantitis: Case Definitions and Diagnostic ConsiderationsDocument9 pagesPeri-Implant Health, Peri-Implant Mucositis, and Peri-Implantitis: Case Definitions and Diagnostic ConsiderationsFrancisca Cardenas OñateNo ratings yet
- Journal of Periodontology - 2022 - Monje - Significance of Barrier Membrane On The Reconstructive Therapy ofDocument13 pagesJournal of Periodontology - 2022 - Monje - Significance of Barrier Membrane On The Reconstructive Therapy of安西 泰規No ratings yet
- 35journal of Periodontology - 2018 - Renvert - Peri Implant Health Peri Implant Mucositis and Peri Implantitis CaseDocument9 pages35journal of Periodontology - 2018 - Renvert - Peri Implant Health Peri Implant Mucositis and Peri Implantitis CaseMax Flores RuizNo ratings yet
- Peri-Implantitis Summary and Consensus Statements of Group 3. The 6th EAO Consensus Conference 2021Document9 pagesPeri-Implantitis Summary and Consensus Statements of Group 3. The 6th EAO Consensus Conference 2021kaue francoNo ratings yet
- JCM 12 07189Document11 pagesJCM 12 07189lehueanh.umpNo ratings yet
- Coronally Advanced Flap With and Without VerticalDocument13 pagesCoronally Advanced Flap With and Without VerticalLEONARDO ALBERTO CRESPIN ZEPEDANo ratings yet
- Journal of Prosthodontics - 2021 - Manicone - Proximal Contact Loss in Implant Supported Restorations A Systematic ReviewDocument9 pagesJournal of Prosthodontics - 2021 - Manicone - Proximal Contact Loss in Implant Supported Restorations A Systematic ReviewDanaNo ratings yet
- Clinical Outcomes of EndodontiDocument13 pagesClinical Outcomes of Endodontiamqg97No ratings yet
- Jurnal 4Document12 pagesJurnal 4April TiramisuNo ratings yet
- Technical Aspects of Treatment in Relation To Treatment OutcomeDocument14 pagesTechnical Aspects of Treatment in Relation To Treatment OutcomekochikaghochiNo ratings yet
- Splinted Vs Nonsplinted ImplantsDocument11 pagesSplinted Vs Nonsplinted ImplantsMathias SchottNo ratings yet
- 4.radiolucent Inflammatory Jaw Lesions A TwentyyearDocument7 pages4.radiolucent Inflammatory Jaw Lesions A TwentyyearMihaela TuculinaNo ratings yet
- Case DefinitionsDocument9 pagesCase DefinitionsCarlos Armijos SNo ratings yet
- Clin Implant Dent Rel Res - 2024 - Serroni - History of Periodontitis As A Risk Factor For Implant Failure and Incidence ofDocument27 pagesClin Implant Dent Rel Res - 2024 - Serroni - History of Periodontitis As A Risk Factor For Implant Failure and Incidence ofarun perioNo ratings yet
- 1303 Prevalence and Etiologic Factors of Non Carious Cervical Lesions Among Prisons Population in DakarDocument6 pages1303 Prevalence and Etiologic Factors of Non Carious Cervical Lesions Among Prisons Population in DakarDHONY MIFTAHUL HUDANo ratings yet
- Renvert Et Al (2018) - Peri Implant Health, Peri Implant Mucositis, and Peri Implantitis - Case Definitions and Diagnostic Considerations - 1Document9 pagesRenvert Et Al (2018) - Peri Implant Health, Peri Implant Mucositis, and Peri Implantitis - Case Definitions and Diagnostic Considerations - 1FelipeOyarceSalazarNo ratings yet
- Insights Into The June 2020 Issue of The JOE - 2020Document2 pagesInsights Into The June 2020 Issue of The JOE - 2020MarielEsmeraldaNo ratings yet
- Autogenous Transalveolar Transplantation ofDocument9 pagesAutogenous Transalveolar Transplantation ofAndi Askandar AminNo ratings yet
- Javier Niño ItalianoDocument12 pagesJavier Niño ItalianoJavier NinoNo ratings yet
- Transalveolar Sinus Floor Lift Without Bone Grafting in Atrophic Maxilla: A Meta-AnalysisDocument9 pagesTransalveolar Sinus Floor Lift Without Bone Grafting in Atrophic Maxilla: A Meta-AnalysisEduardo VissicaroNo ratings yet
- Two Interceptive Approaches To Palatally Displaced Canines - A Prospective Longitudinal StudyDocument6 pagesTwo Interceptive Approaches To Palatally Displaced Canines - A Prospective Longitudinal StudyLuciana PraesNo ratings yet
- Clinical and Radiographic Evaluation of Pulpal and Periradicular Tissue, JR 2016Document5 pagesClinical and Radiographic Evaluation of Pulpal and Periradicular Tissue, JR 20163Racha supremacyNo ratings yet
- Coronectomy 2Document14 pagesCoronectomy 2Rovian RosaliaNo ratings yet
- Bibliografía 3Document27 pagesBibliografía 3monserratrmrzprzNo ratings yet
- Journal of Dentistry: Review ArticleDocument13 pagesJournal of Dentistry: Review ArticleNidia TorreaNo ratings yet
- Mombelli 2005Document10 pagesMombelli 2005luis sanchezNo ratings yet
- Ejoi - 12 - 4 - Daher Immediate Versusconventional Loading of Variable-Taperd Implant Supporting Three To Four Unit Fixed Partial DentureDocument18 pagesEjoi - 12 - 4 - Daher Immediate Versusconventional Loading of Variable-Taperd Implant Supporting Three To Four Unit Fixed Partial Denturedrmezzo68No ratings yet
- Root Resorption On Adjacent Teeth Associated With Included Permanent Canines A Study With Computerized Tomography September 2022 5286961863 7005868Document3 pagesRoot Resorption On Adjacent Teeth Associated With Included Permanent Canines A Study With Computerized Tomography September 2022 5286961863 7005868Nicolas ValenzuelaNo ratings yet
- 2016 Coronectomy of Impacted Mandibular Third Molars A Meta-Analysis and Systematic Review of The LiteratureDocument9 pages2016 Coronectomy of Impacted Mandibular Third Molars A Meta-Analysis and Systematic Review of The LiteraturekaarlaamendezNo ratings yet
- Japid 14 26Document6 pagesJapid 14 26rikaNo ratings yet
- JIAP October 2011 - The Influence of Restorations and Prosthetic Crowns Finishing Lines On Inflammatory Levels After Non-Surgical Periodontal TherapyDocument8 pagesJIAP October 2011 - The Influence of Restorations and Prosthetic Crowns Finishing Lines On Inflammatory Levels After Non-Surgical Periodontal TherapyMedstudNo ratings yet
- Impaksi Eng 7 PDFDocument2 pagesImpaksi Eng 7 PDFDevita Nuryco P . PNo ratings yet
- Berglundh Et Al-2018-Journal of Clinical PeriodontologyDocument6 pagesBerglundh Et Al-2018-Journal of Clinical PeriodontologyCristian CulcitchiNo ratings yet
- J 1600-051x 2012 01903 XDocument9 pagesJ 1600-051x 2012 01903 XDiyaa SakrNo ratings yet
- Medi 96 E5864Document6 pagesMedi 96 E5864mono1144No ratings yet
- French 2019Document7 pagesFrench 2019Netra TaleleNo ratings yet
- Periapical Lesions of The Jaws: A Review of 104 Cases in IbadanDocument5 pagesPeriapical Lesions of The Jaws: A Review of 104 Cases in IbadanShanaz ShaxawanNo ratings yet
- Alamanos 2016Document12 pagesAlamanos 2016dana40018256No ratings yet
- Ocr 12237Document11 pagesOcr 12237André FonsecaNo ratings yet
- Laporan Jurnal Reading Perio - Laila Rahma Milenia - 22010221220067Document35 pagesLaporan Jurnal Reading Perio - Laila Rahma Milenia - 22010221220067Laila R MNo ratings yet
- J Clinic Periodontology - 2018 - Fan - Occlusal Trauma and Excessive Occlusal Forces Narrative Review Case DefinitionsDocument8 pagesJ Clinic Periodontology - 2018 - Fan - Occlusal Trauma and Excessive Occlusal Forces Narrative Review Case DefinitionsAdriana Segura DomínguezNo ratings yet
- Long-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthDocument7 pagesLong-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthSahana RangarajanNo ratings yet
- Smear LayerDocument14 pagesSmear Layersandra del pilarNo ratings yet
- Nonsurgical Management of Complex Endodontic Cases With Several Periapical Lesions: A Case SeriesDocument10 pagesNonsurgical Management of Complex Endodontic Cases With Several Periapical Lesions: A Case SeriesAlyaNo ratings yet
- Tunkel Comparacion Tecnicas2013Document9 pagesTunkel Comparacion Tecnicas2013SergioNo ratings yet
- Comparison of Two Treatment Modalities Operculectomy Vs Thirdmolar Removal For Management of PericoronitisDocument4 pagesComparison of Two Treatment Modalities Operculectomy Vs Thirdmolar Removal For Management of PericoronitisghinaNo ratings yet
- Is Bleeding On Probing A Differential Diagnosis Between Periimplant Health and Disease?Document5 pagesIs Bleeding On Probing A Differential Diagnosis Between Periimplant Health and Disease?Tonya GoldenNo ratings yet
- DfsdfsDocument12 pagesDfsdfsSitiKhadijahNo ratings yet
- OOOO Ricucci 2000Document6 pagesOOOO Ricucci 2000karlaNo ratings yet
- Defectos de Furca y Regeneracion TisularDocument21 pagesDefectos de Furca y Regeneracion TisularSebastián BernalNo ratings yet
- Gingival Recession 10.1.1.677.5356Document4 pagesGingival Recession 10.1.1.677.5356solomonNo ratings yet
- Coronectomy Is An Effective Strategy For TreatingDocument2 pagesCoronectomy Is An Effective Strategy For TreatingAyesha Nasir KhanNo ratings yet
- Lasers: Effect of Low-Level Laser Therapy and Platelet-Rich Fibrin On The Treatment of Intra-Bony DefectsDocument8 pagesLasers: Effect of Low-Level Laser Therapy and Platelet-Rich Fibrin On The Treatment of Intra-Bony DefectsMegha PoojaryNo ratings yet
- Int Endodontic J - 2021 - Zahran - The Impact of An Enhanced Infection Control Protocol On Molar Root Canal TreatmentDocument13 pagesInt Endodontic J - 2021 - Zahran - The Impact of An Enhanced Infection Control Protocol On Molar Root Canal TreatmentMohd NazrinNo ratings yet
- Two Cases of An Atypical Presentation of Necrotizing StomatitisDocument5 pagesTwo Cases of An Atypical Presentation of Necrotizing StomatitisSamehada SamaNo ratings yet
- 2021 - Papilla Preservation Periodontal Surgery in Periodontal Reconstruction For Deep Combined Intra-Suprabony Defects. Retrospective Analysis of A Registry-Based CohortDocument7 pages2021 - Papilla Preservation Periodontal Surgery in Periodontal Reconstruction For Deep Combined Intra-Suprabony Defects. Retrospective Analysis of A Registry-Based CohortJontavius GilbertNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Minimally Invasive Approaches in Endodontic PracticeFrom EverandMinimally Invasive Approaches in Endodontic PracticeGianluca PlotinoNo ratings yet
- SPM Add Maths PaperDocument2 pagesSPM Add Maths PaperSEOW INN LEENo ratings yet
- KL 002.10 Eng Student Guide sp2 v1.0.1 PDFDocument414 pagesKL 002.10 Eng Student Guide sp2 v1.0.1 PDFalexusmatrixNo ratings yet
- Quadratic Equation Kajianp1Document2 pagesQuadratic Equation Kajianp1Siva BalanNo ratings yet
- PW Unit 8 PDFDocument3 pagesPW Unit 8 PDFac5sro1No ratings yet
- Reading Assessment in English For KS 3 4Document23 pagesReading Assessment in English For KS 3 4JENIVIVE D. PARCASIO100% (1)
- The EarthDocument12 pagesThe EarthKather ShaNo ratings yet
- Turbogenerator Stator Windings Support System. Experience-CigreDocument121 pagesTurbogenerator Stator Windings Support System. Experience-CigreJorge Vallejos100% (1)
- The Life and Works of ModiglianiDocument88 pagesThe Life and Works of ModiglianiKaanDemirer100% (1)
- 17 4377arkendughosh2 PDFDocument8 pages17 4377arkendughosh2 PDFRidwan BamideleNo ratings yet
- Data Gathering ActivitiesDocument3 pagesData Gathering ActivitiesKyla PapaNo ratings yet
- Heavyvinyl Issue1Document115 pagesHeavyvinyl Issue1Adam100% (2)
- Baydoun Willett (2000) Islamic Corporate Reports PDFDocument20 pagesBaydoun Willett (2000) Islamic Corporate Reports PDFAqilahAzmiNo ratings yet
- 105 - Quantitative Analysis For Management DecisionsDocument21 pages105 - Quantitative Analysis For Management DecisionsMycareer RamNo ratings yet
- Basic Concepts On Integrating Technology in InstructionDocument19 pagesBasic Concepts On Integrating Technology in InstructionAries PerezNo ratings yet
- IJSARTV6I738053Document3 pagesIJSARTV6I738053VISHAL BHOJWANINo ratings yet
- Guia de Estudio Aguilar Romero Claudia Angelica 109Document3 pagesGuia de Estudio Aguilar Romero Claudia Angelica 109claudia aguilarNo ratings yet
- 12 Step Manual V2.0Document68 pages12 Step Manual V2.0Daniel BatánNo ratings yet
- Formula SheetDocument10 pagesFormula SheetHuraiza AsifNo ratings yet
- West Facing Floor PlansDocument18 pagesWest Facing Floor Plansgurudev001No ratings yet
- Fast Food Nation Book ThesisDocument7 pagesFast Food Nation Book Thesistfwysnikd100% (2)
- Install LogDocument36 pagesInstall Logfrans parulianNo ratings yet
- Sales Rebates ProcessingDocument1 pageSales Rebates ProcessingNavjyot SinghviNo ratings yet
- Đề Tuyển Sinh 10 Chuyên Anh Thpt Chuyên Sư Phạm NĂM 2019: C. exhalation B. droughtDocument7 pagesĐề Tuyển Sinh 10 Chuyên Anh Thpt Chuyên Sư Phạm NĂM 2019: C. exhalation B. droughtKhôi Nguyên ĐặngNo ratings yet
- Datasheet (Signal Booster)Document4 pagesDatasheet (Signal Booster)Shrisha BhatNo ratings yet
- Atlan, Henri - The Living Cell As A Paradigm For Complex Natural SystemsDocument3 pagesAtlan, Henri - The Living Cell As A Paradigm For Complex Natural SystemsKein BécilNo ratings yet
- Imam Ali High School/Mr El Bahi/As-Lessons/Relative Clauses Relative ClausesDocument2 pagesImam Ali High School/Mr El Bahi/As-Lessons/Relative Clauses Relative ClausesEnglish for everyoneNo ratings yet
- Course Javascript Es6Document82 pagesCourse Javascript Es6AIT SALAH MassinissaNo ratings yet
- PhysicsOfMusic PDFDocument288 pagesPhysicsOfMusic PDFcahes100% (1)
- LM140/LM340A/LM340/LM7800C Series 3-Terminal Positive RegulatorsDocument15 pagesLM140/LM340A/LM340/LM7800C Series 3-Terminal Positive Regulatorsvmm mNo ratings yet
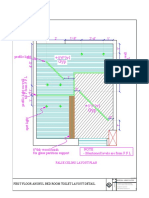
- Toilet False Ceiling PlanDocument1 pageToilet False Ceiling PlanPooja JabadeNo ratings yet