Download as pdf or txt
You might also like
- Insert - Elecsys T3.ms - 11731360122.v26.enDocument4 pagesInsert - Elecsys T3.ms - 11731360122.v26.enGuneyden Guneyden100% (3)
- Insert - Elecsys IgE II.04827031500.V12.enDocument4 pagesInsert - Elecsys IgE II.04827031500.V12.enRaj KumarNo ratings yet
- Nursing Laboratory & Diagnostic Tests Demystified, Second EditionFrom EverandNursing Laboratory & Diagnostic Tests Demystified, Second EditionNo ratings yet
- Myoglobin: A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Document3 pagesMyoglobin: A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Dóra BenczeNo ratings yet
- Tutorial 4 - Business AnalyticsDocument14 pagesTutorial 4 - Business AnalyticsRobin RichardsonNo ratings yet
- Cortisol II 2020-03 v6Document5 pagesCortisol II 2020-03 v6Parishan SaeedNo ratings yet
- Insert - Elecsys Cortisol II.07027150500.V6.EnDocument5 pagesInsert - Elecsys Cortisol II.07027150500.V6.EnVegha NedyaNo ratings yet
- Cortisol II 2017-05 v4Document5 pagesCortisol II 2017-05 v4Moshe FogelNo ratings yet
- LH.11732234500.V23.enDocument4 pagesLH.11732234500.V23.enAbdullah ZobayerNo ratings yet
- Insert - Cortisol II - Ms 06687733190.V4.EnDocument5 pagesInsert - Cortisol II - Ms 06687733190.V4.EnRastu KaryanaNo ratings yet
- Elecsyscyfra211 11820966122 en CanDocument5 pagesElecsyscyfra211 11820966122 en CanAgus SunardiNo ratings yet
- ElecsysCYFRA211 1Document5 pagesElecsysCYFRA211 1Tuấn Minh PhùngNo ratings yet
- Progesterone III: A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Document4 pagesProgesterone III: A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Jimboreanu György PaulaNo ratings yet
- Insert - Elecsys IL-6.05109442500.V9.enDocument4 pagesInsert - Elecsys IL-6.05109442500.V9.enraraNo ratings yet
- Insert - Elecsys CEA.07027079500.V5.EnDocument4 pagesInsert - Elecsys CEA.07027079500.V5.EnVegha NedyaNo ratings yet
- Insert - Elecsys CA 15-3 II.03045838500.V22.enDocument5 pagesInsert - Elecsys CA 15-3 II.03045838500.V22.enLILI DARMAPUTRINo ratings yet
- Insert - Elecsys Anti-HBs II - Ms - 05894816190.V2.EnDocument4 pagesInsert - Elecsys Anti-HBs II - Ms - 05894816190.V2.EnyantuNo ratings yet
- Testosteron II 2017-11 v9Document6 pagesTestosteron II 2017-11 v9Daoud IssaNo ratings yet
- Elecsys BRAHMS PCT: ProcalcitoninDocument5 pagesElecsys BRAHMS PCT: ProcalcitoninDóra BenczeNo ratings yet
- Insert - Elecsys CA 19-9.11776193501.v9.enDocument4 pagesInsert - Elecsys CA 19-9.11776193501.v9.enonedarigirlNo ratings yet
- Insert - Elecsys Estradiol III.07027249500.V8.EnDocument5 pagesInsert - Elecsys Estradiol III.07027249500.V8.EnVegha NedyaNo ratings yet
- Insert - Elecsys CA 15-3 II.07027001500.V7.enDocument5 pagesInsert - Elecsys CA 15-3 II.07027001500.V7.enVegha NedyaNo ratings yet
- A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) ) : REF SystemDocument3 pagesA) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) ) : REF SystemhairiNo ratings yet
- Insert - Elecsys CYFRA 21-1.07299966500.v7.enDocument5 pagesInsert - Elecsys CYFRA 21-1.07299966500.v7.enVegha NedyaNo ratings yet
- Elecsys CA 15-3 II: A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Document5 pagesElecsys CA 15-3 II: A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Douglas MirandaNo ratings yet
- A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Document4 pagesA) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )hairiNo ratings yet
- AslotDocument4 pagesAslotDrAlaa ZidanNo ratings yet
- Elecsys BRAHMS PCT: ProcalcitoninDocument5 pagesElecsys BRAHMS PCT: ProcalcitoninMilagrosLcNo ratings yet
- Anti-Tg 2018-07 v6Document5 pagesAnti-Tg 2018-07 v6Ismael CulquiNo ratings yet
- Digoxin: 11820796 190 Cobas e 411 Cobas e 601 Cobas e 602 English Intended UseDocument5 pagesDigoxin: 11820796 190 Cobas e 411 Cobas e 601 Cobas e 602 English Intended UsehairiNo ratings yet
- E CA19-9ms en 20Document3 pagesE CA19-9ms en 20Hassan GillNo ratings yet
- Ca 15-3 IiDocument4 pagesCa 15-3 IiMd. Moniruzzaman100% (1)
- FeritinaDocument4 pagesFeritinaJimboreanu György PaulaNo ratings yet
- TSH 2017-05 v23Document3 pagesTSH 2017-05 v23Yaser MNo ratings yet
- Anti-Tpo 2017-07 v5Document4 pagesAnti-Tpo 2017-07 v5Ismael CulquiNo ratings yet
- Insert - Anti-Tg CalSet - Ms 06368603190.V6.EnDocument2 pagesInsert - Anti-Tg CalSet - Ms 06368603190.V6.EnVegha NedyaNo ratings yet
- AAT2 enDocument3 pagesAAT2 enSyahdie FahledieNo ratings yet
- Insert - Elecsys CA 19-9.11776193500.v26.enDocument4 pagesInsert - Elecsys CA 19-9.11776193500.v26.ennatawulan dianNo ratings yet
- Elecsys IL-6: Cobas e 411 Cobas e 601 Cobas e 602 Cobas e 801Document12 pagesElecsys IL-6: Cobas e 411 Cobas e 601 Cobas e 602 Cobas e 801Okky IrawanNo ratings yet
- AFP α1-fetoprotein: a) Tris (2,2'-bipyridyl) ruthenium (II) -complex (Ru (bpy) )Document4 pagesAFP α1-fetoprotein: a) Tris (2,2'-bipyridyl) ruthenium (II) -complex (Ru (bpy) )hairiNo ratings yet
- Insert - CA 15-3 II - Ms - 03045838122.v18.enDocument4 pagesInsert - CA 15-3 II - Ms - 03045838122.v18.enFateh AzwiNo ratings yet
- Insert - Elecsys Anti Tg.09005021500.V1.EnDocument4 pagesInsert - Elecsys Anti Tg.09005021500.V1.EnVegha NedyaNo ratings yet
- Insert - PreciControl Multimarker - Ms - 05341787160 - USA.V6.enDocument2 pagesInsert - PreciControl Multimarker - Ms - 05341787160 - USA.V6.enykinomoto5No ratings yet
- Insert - Elecsys Syphilis - Ms 07802960190.V3.EnDocument5 pagesInsert - Elecsys Syphilis - Ms 07802960190.V3.EnGuneyden GuneydenNo ratings yet
- IgE II.V9Document4 pagesIgE II.V9Abdullah ZobayerNo ratings yet
- Total PSADocument4 pagesTotal PSAYeni Valderrama CcahuanaNo ratings yet
- E Anti-TgDocument4 pagesE Anti-TgHassan GillNo ratings yet
- DIGITDocument4 pagesDIGITARIF AHAMMED PNo ratings yet
- Insert - Elecsys Total PSA - Ms - 04641655190.V13.EnDocument5 pagesInsert - Elecsys Total PSA - Ms - 04641655190.V13.Entawfiq MohammadNo ratings yet
- Elecsys T4: Cobas e 411 Cobas e 601 Cobas e 602 English System InformationDocument5 pagesElecsys T4: Cobas e 411 Cobas e 601 Cobas e 602 English System InformationIsmael CulquiNo ratings yet
- Toxo Igm 2018-12 v11Document5 pagesToxo Igm 2018-12 v11ابو حمزةNo ratings yet
- E Digitoxin en 10Document3 pagesE Digitoxin en 10Hassan GillNo ratings yet
- Hbsagii 08814856190 en CanDocument5 pagesHbsagii 08814856190 en Canfarrah025No ratings yet
- CEA 11973223001 - enDocument3 pagesCEA 11973223001 - enModestusNo ratings yet
- FerritinDocument3 pagesFerritinModestus100% (1)
- Insert - Elecsys Anti-SARS-CoV-2 S.09289267500.V1.enDocument7 pagesInsert - Elecsys Anti-SARS-CoV-2 S.09289267500.V1.enLilik IndrawatiNo ratings yet
- CA 19-9 11872141001 - enDocument3 pagesCA 19-9 11872141001 - enModestusNo ratings yet
- Elecsys Hbsag Ii: A) Tris (2,2'-Bipyridyl) Ruthenium (Ii) - Complex (Ru (Bpy) )Document5 pagesElecsys Hbsag Ii: A) Tris (2,2'-Bipyridyl) Ruthenium (Ii) - Complex (Ru (Bpy) )Brian SamanyaNo ratings yet
- Insert - LH.ms 11732234122.v19.enDocument4 pagesInsert - LH.ms 11732234122.v19.enyantuNo ratings yet
- ACCENT-200 ASO ADocument2 pagesACCENT-200 ASO Aemc.medicalserviceNo ratings yet
- LH.11732234500.V23.enDocument4 pagesLH.11732234500.V23.enAbdullah ZobayerNo ratings yet
- Elecsys HGH: A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Document5 pagesElecsys HGH: A) Tris (2,2'-Bipyridyl) Ruthenium (II) - Complex (Ru (Bpy) )Abdullah ZobayerNo ratings yet
- CA 125 II - Ms - 11776223190.v2.enDocument4 pagesCA 125 II - Ms - 11776223190.v2.enAbdullah ZobayerNo ratings yet
- CA 15-3 II.03045838500.V23.enDocument5 pagesCA 15-3 II.03045838500.V23.enAbdullah ZobayerNo ratings yet
- Anti-HAV.V12Document4 pagesAnti-HAV.V12Abdullah ZobayerNo ratings yet
- Chap 02Document42 pagesChap 02Mahmoud WahshNo ratings yet
- Algoritmo Floyd WarshallDocument3 pagesAlgoritmo Floyd WarshallmcgeraldNo ratings yet
- Chap 123 Final Paper N Aunt ADocument48 pagesChap 123 Final Paper N Aunt AjoannaotawayNo ratings yet
- Finite Difference Methods For HJB PDEsDocument12 pagesFinite Difference Methods For HJB PDEsbobmezzNo ratings yet
- 09 Displacement Method - Slope Deflection EquationsDocument29 pages09 Displacement Method - Slope Deflection EquationsZhwa 18No ratings yet
- Hatch & Portlight GuidesDocument12 pagesHatch & Portlight Guidesjeanpaul.var.valNo ratings yet
- 2014 Zhang Book Chapter Divergence GeometryDocument27 pages2014 Zhang Book Chapter Divergence GeometrysggtioNo ratings yet
- (Limin Zhang, Yu Wang, Gang Wang, Li Dianqing) GeoDocument598 pages(Limin Zhang, Yu Wang, Gang Wang, Li Dianqing) GeoMarg OrpeecNo ratings yet
- BS en 00059-2016Document14 pagesBS en 00059-2016anurag yadavNo ratings yet
- VMC - SOSE JEE MAINS - 4 (Question Paper)Document14 pagesVMC - SOSE JEE MAINS - 4 (Question Paper)Gunjan SinghNo ratings yet
- Analysis and Design of Down-Aisle Pallet Rack StructuresDocument11 pagesAnalysis and Design of Down-Aisle Pallet Rack StructuresAbdalla Sharf EldienNo ratings yet
- 50 W Base Plate DesignDocument36 pages50 W Base Plate DesignKiely LiveprojectsNo ratings yet
- BSS AR-204 DatasheetDocument1 pageBSS AR-204 DatasheetAndy AndyNo ratings yet
- Body BiasDocument7 pagesBody BiasSwaroop KumarNo ratings yet
- Reactive Power Problems and System: Submitted By:-Section: - Roll No: - SubjectDocument16 pagesReactive Power Problems and System: Submitted By:-Section: - Roll No: - SubjectShubham AgrawalNo ratings yet
- Paper Chromatography: A Review: Mukta Gupta, Bhupinder Kapoor, Reena GuptaDocument8 pagesPaper Chromatography: A Review: Mukta Gupta, Bhupinder Kapoor, Reena GuptaYonas AlexandryNo ratings yet
- RPT ManualDocument20 pagesRPT Manualamele25No ratings yet
- Transmission Electron MicrosDocument97 pagesTransmission Electron MicrosAnonymous 0tqzNTWyyNo ratings yet
- Panel Punch Points Report-06!08!2019Document165 pagesPanel Punch Points Report-06!08!2019Kamesh MarwadeNo ratings yet
- Extenuate DDos Attacks in CloudDocument4 pagesExtenuate DDos Attacks in CloudkiranNo ratings yet
- Determining Sediment Concentration in Water Samples: Standard Test Methods ForDocument6 pagesDetermining Sediment Concentration in Water Samples: Standard Test Methods ForFajar Adi Nugroho100% (1)
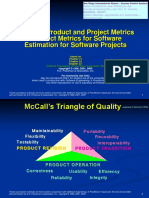
- Process, Product and Project Metrics Product Metrics For Software Estimation For Software ProjectsDocument46 pagesProcess, Product and Project Metrics Product Metrics For Software Estimation For Software ProjectsNassah AllaabNo ratings yet
- Wmsu Shs Students Perception of Grade 11Document46 pagesWmsu Shs Students Perception of Grade 11jaywarven100% (1)
- LEcture 14Document15 pagesLEcture 14asdsdNo ratings yet
- LCM and GCFDocument5 pagesLCM and GCFJULIA ALLANANo ratings yet
- Lecture 19 BDocument6 pagesLecture 19 BHongYu HuiNo ratings yet
- RospDocument55 pagesRospZoroNo ratings yet
- F646 CompleteSampleDocument36 pagesF646 CompleteSampleraj4523No ratings yet
- Asme Sec V A-2 RT PDFDocument44 pagesAsme Sec V A-2 RT PDFmsalinasaguilar71% (7)