Download as pdf or txt
You might also like
- Rekha D PDFDocument3 pagesRekha D PDFAbhishek ShrivastavNo ratings yet
- Report 6737931eDocument19 pagesReport 6737931eNeevinternational NeevNo ratings yet
- Report 400d0061Document18 pagesReport 400d0061Santosh BhandarkarNo ratings yet
- Po4009507960 540Document15 pagesPo4009507960 540PRADEEP KUMARNo ratings yet
- Report 3f90266bDocument18 pagesReport 3f90266bSK TacNo ratings yet
- 1-Senior Citizen Basic Package - PO3248534977-432Document16 pages1-Senior Citizen Basic Package - PO3248534977-432Krishna Nand RaiNo ratings yet
- Afridi Shaikh-23Document5 pagesAfridi Shaikh-23Altamash AnsariNo ratings yet
- 1-Good Health Premium Package - PO1065281239-651Document19 pages1-Good Health Premium Package - PO1065281239-651Renu ChoudharyNo ratings yet
- Report 220719 195623Document11 pagesReport 220719 195623Abdullah AlviNo ratings yet
- Report Geeti PaulDocument22 pagesReport Geeti PaulSAIKAT PAULNo ratings yet
- 1-Glucose - Postprandial YOGESHDocument19 pages1-Glucose - Postprandial YOGESHMeet PatelNo ratings yet
- Report 831a66a7 PDFDocument23 pagesReport 831a66a7 PDFViral PatelNo ratings yet
- Shaharyar Ansari: Report Status: FinalDocument3 pagesShaharyar Ansari: Report Status: FinalAutonomous Alfa100% (1)
- 1 Diabetes Screening PO4047576719 696Document4 pages1 Diabetes Screening PO4047576719 696rishiranjan04No ratings yet
- Lab ReportDocument2 pagesLab ReportSamir Kumar DashNo ratings yet
- Report B6cc7e5bDocument3 pagesReport B6cc7e5bArchana SinghNo ratings yet
- Report 33edcab8Document5 pagesReport 33edcab8sujithm435489No ratings yet
- Date 28/mar/2023 09:29AM Unit Bio Ref Interval: Laboratory Investigation ReportDocument10 pagesDate 28/mar/2023 09:29AM Unit Bio Ref Interval: Laboratory Investigation ReportbhailogofficiaNo ratings yet
- 1-Liver Function Test - PO3921596584-773 - 230517 - 125136Document4 pages1-Liver Function Test - PO3921596584-773 - 230517 - 125136Moksh GujjarNo ratings yet
- Gulrez Ali: Haematology Comprehensive Full Body Check Test Name Result Unit Bio Ref - Interval MethodDocument17 pagesGulrez Ali: Haematology Comprehensive Full Body Check Test Name Result Unit Bio Ref - Interval MethodGulrez AliNo ratings yet
- Tathagata Chatterjee: Report Status: FinalDocument2 pagesTathagata Chatterjee: Report Status: FinalTathagata ChatterjeeNo ratings yet
- Date 04/sep/2023 08:31AM 09/jul/23 08:10AM Unit Bio Ref IntervalDocument2 pagesDate 04/sep/2023 08:31AM 09/jul/23 08:10AM Unit Bio Ref IntervalAnimesh MondalNo ratings yet
- Report-812012540001431MR Rajesh TakDocument2 pagesReport-812012540001431MR Rajesh TakKrish JainNo ratings yet
- Date 15/feb/2024 12:05PM 31/jul/23 11:10AM Unit Bio Ref IntervalDocument4 pagesDate 15/feb/2024 12:05PM 31/jul/23 11:10AM Unit Bio Ref IntervalrajorajisunnyNo ratings yet
- Falaan ReportDocument4 pagesFalaan ReportAzeem ChauhanNo ratings yet
- Date 03/aug/2023 07:32AM Unit Bio Ref Interval: Laboratory Investigation ReportDocument12 pagesDate 03/aug/2023 07:32AM Unit Bio Ref Interval: Laboratory Investigation ReportRishabh GuptaNo ratings yet
- Date 01/dec/2021 04:33AM 30/nov/21 05:17PM Unit Bio Ref IntervalDocument2 pagesDate 01/dec/2021 04:33AM 30/nov/21 05:17PM Unit Bio Ref IntervalSaurabh PuriNo ratings yet
- Max2report PrintDocument6 pagesMax2report Printdevender0yadavNo ratings yet
- ReportDocument3 pagesReportPawan MadhesiyaNo ratings yet
- Complete Blood Count: Name DR Chetanbhai MojidaraDocument2 pagesComplete Blood Count: Name DR Chetanbhai Mojidarachetan mojidraNo ratings yet
- 1-Diabetes Screening - PO1580805721-424Document4 pages1-Diabetes Screening - PO1580805721-424Ekta Anshul JainNo ratings yet
- Date 30/nov/2021 02:37AM 29/nov/21 07:51PM Unit Bio Ref IntervalDocument2 pagesDate 30/nov/2021 02:37AM 29/nov/21 07:51PM Unit Bio Ref IntervalSaurabh PuriNo ratings yet
- 8000000936: Patient ID 80001350 Sid No Nehru Nagar Branch Mr. Vasanth NDocument3 pages8000000936: Patient ID 80001350 Sid No Nehru Nagar Branch Mr. Vasanth NSudha SaravananNo ratings yet
- Report PDFDocument6 pagesReport PDFAayushiNo ratings yet
- Haematology Haematology Haematology HaematologyDocument5 pagesHaematology Haematology Haematology HaematologysakshamNo ratings yet
- Haematology: DR - Abhilash Kumar JainDocument1 pageHaematology: DR - Abhilash Kumar Jainseds5anuragNo ratings yet
- Labreportnew - 2023-02-17T141822.094Document8 pagesLabreportnew - 2023-02-17T141822.094pavanimatteguntaNo ratings yet
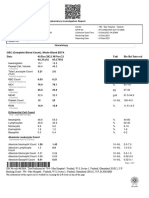
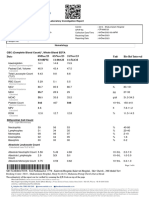
- Haematology Test Name Results Biological Reference Interval Units Specimen Test Method CBC - Complete Blood CountDocument8 pagesHaematology Test Name Results Biological Reference Interval Units Specimen Test Method CBC - Complete Blood CountArun DheekshahNo ratings yet
- S81 - Ram Ratan Lab-CcDocument1 pageS81 - Ram Ratan Lab-CcCHANDAN KUMARNo ratings yet
- Department of Biochemistry Campaign Diabetic Check (With PP)Document2 pagesDepartment of Biochemistry Campaign Diabetic Check (With PP)gsm2008No ratings yet
- Remotesensing 12 00857 v2Document1 pageRemotesensing 12 00857 v2Rajarshi BhattacharyaNo ratings yet
- Department of Clinical Biochemistry: Total Cholesterol, SerumDocument1 pageDepartment of Clinical Biochemistry: Total Cholesterol, SerumSabarinath RK PillaiNo ratings yet
- FRM Patient View All ReportDocument6 pagesFRM Patient View All ReportShailesh KumarNo ratings yet
- Shailendra Tamanekar 06102022 Report-1Document2 pagesShailendra Tamanekar 06102022 Report-1Shailendra TamanekarNo ratings yet
- Self Sangita Chauhan (46Y/F) 400/2C Saket Nagar Bhopal, Bhopal, 462024Document12 pagesSelf Sangita Chauhan (46Y/F) 400/2C Saket Nagar Bhopal, Bhopal, 462024Raj ChauhanNo ratings yet
- MadhavDocument1 pageMadhavmadhav maheshwariNo ratings yet
- 23rglmgb2punhj3tbk4mpfhzDocument1 page23rglmgb2punhj3tbk4mpfhzHarsh AryaNo ratings yet
- Department of Clinical Biochemistry: Lipid ProfileDocument3 pagesDepartment of Clinical Biochemistry: Lipid ProfilegeorgeNo ratings yet
- Apollo247 01 Jul 2021 Supriya ThakurDocument4 pagesApollo247 01 Jul 2021 Supriya ThakurthakuryaNo ratings yet
- Al41717200074538040 RLSDocument10 pagesAl41717200074538040 RLSanjali vermaNo ratings yet
- LabTest 29dec2023Document15 pagesLabTest 29dec2023Ayush KumarNo ratings yet
- LabTest 18jul2023Document5 pagesLabTest 18jul2023Kedarnath KundaNo ratings yet
- Arogyam1 3Document12 pagesArogyam1 3Sashikanta NayakNo ratings yet
- ReportDocument6 pagesReportvenkateshgoudvenkateshgouNo ratings yet
- Kgxrdtqpylps1aixlnec2p3y PDFDocument1 pageKgxrdtqpylps1aixlnec2p3y PDFNaveen PathakNo ratings yet
- KUNALYADAVreportDocument2 pagesKUNALYADAVreportSourabhNo ratings yet
- Thyrocare Processed atDocument3 pagesThyrocare Processed atKarim SirNo ratings yet
- RSLT An21100870 PDFDocument3 pagesRSLT An21100870 PDFMuhammed Ameen MoulaviNo ratings yet
- Aa709c29738113611478 RLSDocument3 pagesAa709c29738113611478 RLSLace HouseNo ratings yet
- Report F412b1a3Document18 pagesReport F412b1a3055Nitish BhatiaNo ratings yet
- 2023.04.04 TB Questionnaire - Fillable PDFDocument3 pages2023.04.04 TB Questionnaire - Fillable PDFLinxuan LiNo ratings yet
- Poisoning PPT Nursing FoundationDocument16 pagesPoisoning PPT Nursing FoundationMahimaNo ratings yet
- RBSE Class 8 Science Notes Chapter 8 Our Health, Diseases and Prevention - RBSE GuideDocument5 pagesRBSE Class 8 Science Notes Chapter 8 Our Health, Diseases and Prevention - RBSE GuideAlpine AcademiaNo ratings yet
- Drug StudyDocument2 pagesDrug StudyAnne Nicole ObispoNo ratings yet
- DR Pridania Vidya Ayuningtyas SpADocument7 pagesDR Pridania Vidya Ayuningtyas SpAumi barokahNo ratings yet
- 7primary & Secondary LesionsDocument6 pages7primary & Secondary LesionsOsamaNo ratings yet
- Amaros TrialDocument43 pagesAmaros TrialnitinNo ratings yet
- Migraine Cause and TreatmentDocument4 pagesMigraine Cause and TreatmentSorin PalcuNo ratings yet
- Pharm Exam 4 ReviewDocument2 pagesPharm Exam 4 ReviewHwi GNDCNo ratings yet
- Go Wyoming (Fall 2023)Document32 pagesGo Wyoming (Fall 2023)The Livingston County NewsNo ratings yet
- Acute Lymphoblastic Leukemia ThesisDocument5 pagesAcute Lymphoblastic Leukemia Thesisljctxlgld100% (2)
- Upper Airway ObstructionDocument12 pagesUpper Airway ObstructionAbhishek ChouhanNo ratings yet
- Letter To The Editor (Orignal)Document10 pagesLetter To The Editor (Orignal)Cynthia weirNo ratings yet
- Medical Student Career Paths BookDocument124 pagesMedical Student Career Paths BookMindi WindmillNo ratings yet
- Blood Tests ReportDocument7 pagesBlood Tests ReportLalith GoudNo ratings yet
- Chapter 3. Birth Asphyxia and ResuscitationDocument20 pagesChapter 3. Birth Asphyxia and ResuscitationNastehaNo ratings yet
- Chapter 16 - HeadacheDocument7 pagesChapter 16 - HeadacheSerious LeoNo ratings yet
- Brenda Alvarez Leccion 4Document8 pagesBrenda Alvarez Leccion 4Brenda AlvNo ratings yet
- Clinical Case Quizzes - American Association of Clinical EndocrinologyDocument20 pagesClinical Case Quizzes - American Association of Clinical EndocrinologyNesreden Jemal KedirNo ratings yet
- Case by Case Examination by Padeniya SirDocument4 pagesCase by Case Examination by Padeniya SirtharikaneelawathuraNo ratings yet
- Physiotherapy2019 ScientificProgramDocument4 pagesPhysiotherapy2019 ScientificProgramCristinaMolasNo ratings yet
- Effect of Vitamin C On Blood Glucose, Serum Lipids & Serum Insulin in Type 2 Diabetes PatientsDocument5 pagesEffect of Vitamin C On Blood Glucose, Serum Lipids & Serum Insulin in Type 2 Diabetes Patientssahama2508No ratings yet
- Untitled DocumentDocument4 pagesUntitled DocumentLouie Jay VillaganesNo ratings yet
- Barnett Patricia. - The Walker Cycle of Violence andDocument95 pagesBarnett Patricia. - The Walker Cycle of Violence andBetzi RuizNo ratings yet
- DrugStudy SalutilloDocument5 pagesDrugStudy SalutilloErwin SmithNo ratings yet
- PowerPoint Slides With Suggested CommentaryDocument66 pagesPowerPoint Slides With Suggested CommentaryLegal MomentumNo ratings yet
- Nursing Diagnosis 1Document5 pagesNursing Diagnosis 1Kim TangoNo ratings yet
- 2020 PrevMed 2 LE1 FeedbackDocument8 pages2020 PrevMed 2 LE1 Feedbackroxanne.viriNo ratings yet
- Problem List 1. Acute Pain 2. Nutrition Less Than Body Requirements 3. Impaired Physical Mobility 4. Impaired Skin Integrity 5. Disturbed Body ImageDocument12 pagesProblem List 1. Acute Pain 2. Nutrition Less Than Body Requirements 3. Impaired Physical Mobility 4. Impaired Skin Integrity 5. Disturbed Body Imagebernadette babaranNo ratings yet
- Maternal, Fetal, and Neonatal Outcomes in Pregnant Dengue Patients in MexicoDocument8 pagesMaternal, Fetal, and Neonatal Outcomes in Pregnant Dengue Patients in MexicoLola del carmen RojasNo ratings yet