
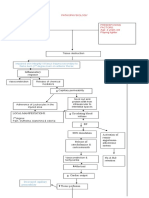
Manifestaciones Clínicas de Desórdenes de La Microcirculacion
Manifestaciones Clínicas de Desórdenes de La Microcirculacion
You might also like
- Buku Pegangan Kursus DSTC - FinalDocument119 pagesBuku Pegangan Kursus DSTC - FinalabdurrahmanNo ratings yet
- KS3 Blood Circulation TESTDocument4 pagesKS3 Blood Circulation TESTA.K Mon100% (1)
- Angelito L. Ramos Jr. RN Clinical InstructorDocument68 pagesAngelito L. Ramos Jr. RN Clinical Instructorraymondblade18100% (17)
- Diagnostics 11 01559 v2Document21 pagesDiagnostics 11 01559 v2Luis CortezNo ratings yet
- Lactato y Perfusion Kattan y GlennDocument5 pagesLactato y Perfusion Kattan y GlennAna Belén Artero CastañoNo ratings yet
- Rheology For CliniciansDocument8 pagesRheology For CliniciansRaluca LNo ratings yet
- 2021 CURR ORIBK CARDIOL Septic Cardiomiopathy From Basics To Management ChoicesDocument18 pages2021 CURR ORIBK CARDIOL Septic Cardiomiopathy From Basics To Management ChoicesConny MuñozNo ratings yet
- Shock Septico EvidenciaDocument8 pagesShock Septico EvidenciaFra1312No ratings yet
- Journal of Intensive Medicine: Florence Boissier, Nadia AissaouiDocument9 pagesJournal of Intensive Medicine: Florence Boissier, Nadia AissaouiMaudiel BrionesNo ratings yet
- Disseminated Intravascular Coagulopathy DICDocument24 pagesDisseminated Intravascular Coagulopathy DICMassimiliano MalerbaNo ratings yet
- Microcirculatory Alterations in Cardiac Surgery A ComprehensiveDocument10 pagesMicrocirculatory Alterations in Cardiac Surgery A ComprehensiveJuan Antonio SantosNo ratings yet
- Pathophysiology of Sepsis-Induced Myocardial Dysfunction: Review Open AccessDocument9 pagesPathophysiology of Sepsis-Induced Myocardial Dysfunction: Review Open AccessjessicaesmrldaNo ratings yet
- Microcirculacion en SepsisDocument4 pagesMicrocirculacion en Sepsis1.Bishop MasterNo ratings yet
- 10 1097@MCC 0000000000000356Document8 pages10 1097@MCC 0000000000000356Elena StepanNo ratings yet
- Sepsis-Induced Cardiomyopathy: A Comprehensive Review: Published Online: 6 May 2020Document12 pagesSepsis-Induced Cardiomyopathy: A Comprehensive Review: Published Online: 6 May 2020Alicia GarcíaNo ratings yet
- Oxygen Extraction and Perfusion Markers in Severe Sepsis and Septic Shock - Diagnostic, Therapeutic and Outcome ImplicationsDocument7 pagesOxygen Extraction and Perfusion Markers in Severe Sepsis and Septic Shock - Diagnostic, Therapeutic and Outcome Implicationshvf41327No ratings yet
- Noninvasive Hemodynamic Monitoring in The Intensive Care UnitDocument18 pagesNoninvasive Hemodynamic Monitoring in The Intensive Care UnitmegaNo ratings yet
- Vasoplegic Syndrome Following Cardiothoracic Surgery-Review of Pathophysiology and Update of Treatment Options - PMCDocument21 pagesVasoplegic Syndrome Following Cardiothoracic Surgery-Review of Pathophysiology and Update of Treatment Options - PMCluis orlando bustamante rojasNo ratings yet
- Management of Sepsis and Septic Shock in The Emergency DepartmentDocument13 pagesManagement of Sepsis and Septic Shock in The Emergency DepartmentandreaNo ratings yet
- Sepsis y Shock SepticoDocument41 pagesSepsis y Shock SepticoSilvia GarciaNo ratings yet
- DefinitionofdicDocument9 pagesDefinitionofdicDwika AudiyanandaNo ratings yet
- The Relationship Between Retinal Microvascular Abnormalities and Coronary Heart DiseaseDocument7 pagesThe Relationship Between Retinal Microvascular Abnormalities and Coronary Heart DiseaseMaria Camila RestrepoNo ratings yet
- Yjbm 92 4 629Document12 pagesYjbm 92 4 629Alfonso Ga MaNo ratings yet
- Choque Septico en CirrosisDocument19 pagesChoque Septico en CirrosisAzael HaggardNo ratings yet
- Macrocirculation and Microcirculation The Batman.39Document4 pagesMacrocirculation and Microcirculation The Batman.39Bro ManiacNo ratings yet
- 2022 Sepsis Related CardiomyopathyDocument3 pages2022 Sepsis Related Cardiomyopathystef lopezNo ratings yet
- BR J Haematol 2021 Adelborg Disseminated Intravascular CoagulationDocument16 pagesBR J Haematol 2021 Adelborg Disseminated Intravascular CoagulationSergio Alberto Sulub NavarreteNo ratings yet
- Sepsis-Induced AKI Revisited - Curr Op Crit Care 2014Document9 pagesSepsis-Induced AKI Revisited - Curr Op Crit Care 2014Vika RatuNo ratings yet
- Circulating Microvesicles in Convalescent Ischemic Stroke Patients: A Contributor To High-On-Treatment Residual Platelet Reactivity?Document7 pagesCirculating Microvesicles in Convalescent Ischemic Stroke Patients: A Contributor To High-On-Treatment Residual Platelet Reactivity?Nasdı BabayevaNo ratings yet
- The Vascular Biology of Atherosclerosis and Imaging TargetsDocument6 pagesThe Vascular Biology of Atherosclerosis and Imaging TargetsOrsid Sierra OchoaNo ratings yet
- Cerebral Venous Sinus ThrombosisDocument11 pagesCerebral Venous Sinus ThrombosisdjcafNo ratings yet
- Cardiac Involvement in Systemic SclerosisDocument7 pagesCardiac Involvement in Systemic SclerosisWisnu MataramNo ratings yet
- Management of Vasoplegic ShockDocument16 pagesManagement of Vasoplegic ShockxmksmwyspyNo ratings yet
- Micro IngenieriaDocument11 pagesMicro IngenieriaAlejandra Ramirez SanchezNo ratings yet
- Stroke Fix 1Document5 pagesStroke Fix 1Inset RiniNo ratings yet
- Intracranial AterosclerosisDocument6 pagesIntracranial AterosclerosisMarshell TendeanNo ratings yet
- HHS Public Access: Sepsis-Induced AKI Revisited: Pathophysiology, Prevention and Future TherapiesDocument13 pagesHHS Public Access: Sepsis-Induced AKI Revisited: Pathophysiology, Prevention and Future TherapiesromiNo ratings yet
- PIIS246802492301536XDocument13 pagesPIIS246802492301536XjosedegibesNo ratings yet
- Clinical Review: Myocardial Depression in Sepsis and Septic ShockDocument9 pagesClinical Review: Myocardial Depression in Sepsis and Septic ShockwasiNo ratings yet
- Sepsis Parte 1Document16 pagesSepsis Parte 1Maria AlejandraNo ratings yet
- Management of Sepsis-Induced Acute Kidney Injury: ReviewDocument12 pagesManagement of Sepsis-Induced Acute Kidney Injury: ReviewVika RatuNo ratings yet
- Clinical and Experimental Emergency MedicineDocument56 pagesClinical and Experimental Emergency MedicineAlfonso Ga MaNo ratings yet
- Https:emedicine Medscape Com:article:1227025-PrintDocument18 pagesHttps:emedicine Medscape Com:article:1227025-PrintSalsa BillaNo ratings yet
- CID Coagulación Intravascular TratamientoDocument16 pagesCID Coagulación Intravascular Tratamientoaraceli garciaNo ratings yet
- Icu Jendd2Document1 pageIcu Jendd2Jennifer AlamonNo ratings yet
- Circulation 2004 Zhu 2109 15Document8 pagesCirculation 2004 Zhu 2109 15gekayuuNo ratings yet
- Research Article: Retinal Structural and Microvascular Alterations in Different Acute Ischemic Stroke SubtypesDocument10 pagesResearch Article: Retinal Structural and Microvascular Alterations in Different Acute Ischemic Stroke SubtypesKarina NathaniaNo ratings yet
- Delta Neutrophil Index As An Early MDocument9 pagesDelta Neutrophil Index As An Early MFariz NurNo ratings yet
- Fluid Therapy and The Microcirculation in Health and Critical IllnessDocument11 pagesFluid Therapy and The Microcirculation in Health and Critical IllnessAdote DrmNo ratings yet
- Expert Statement For Management Hypovolemia in Sepsis PDFDocument8 pagesExpert Statement For Management Hypovolemia in Sepsis PDFRobi HeryantoNo ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptVictor Euclides Briones MoralesNo ratings yet
- Diastolic Dysfunction and Mortality in Severe Sepsis and Septic ShockDocument9 pagesDiastolic Dysfunction and Mortality in Severe Sepsis and Septic ShockShinohara YuusukeNo ratings yet
- Senam OtakDocument15 pagesSenam OtakDewi WulandariNo ratings yet
- Assessment of Volume Status and Fluid Responsiveness in The Emergency Department: A Systematic ApproachDocument8 pagesAssessment of Volume Status and Fluid Responsiveness in The Emergency Department: A Systematic ApproachandreaNo ratings yet
- 4ng-Komplikasi Jantung - CAP & COVIDDocument5 pages4ng-Komplikasi Jantung - CAP & COVIDsukiyantoNo ratings yet
- Sepsis and Septic Shock StrategiesDocument41 pagesSepsis and Septic Shock StrategiesBolivar IseaNo ratings yet
- HSA e Isquemia Tardia 2016Document12 pagesHSA e Isquemia Tardia 2016Ellys Macías PeraltaNo ratings yet
- Cells 11 04136 v2Document3 pagesCells 11 04136 v2ayunda rinataNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptMuhammad Dadan KurniawanNo ratings yet
- Sepsis UptodateDocument56 pagesSepsis Uptodatejosip_11No ratings yet
- Oxygen DeliveryDocument11 pagesOxygen DeliveryFatimah Syed OmarNo ratings yet
- Arterial Disorders: Definition, Clinical Manifestations, Mechanisms and Therapeutic ApproachesFrom EverandArterial Disorders: Definition, Clinical Manifestations, Mechanisms and Therapeutic ApproachesAdel BerbariNo ratings yet
- Normal Coronary Artery Dimensions in IndiansDocument6 pagesNormal Coronary Artery Dimensions in IndiansISHAN NIGAMNo ratings yet
- Ankle Brachial Index PDFDocument8 pagesAnkle Brachial Index PDFIncredibleNo ratings yet
- Effect of Progressive Muscle Relaxation Combined With Deep Breathing Technique Immediately After Aerobic Exercises On Essential HypertensionDocument2 pagesEffect of Progressive Muscle Relaxation Combined With Deep Breathing Technique Immediately After Aerobic Exercises On Essential HypertensionNetraNo ratings yet
- Circulatory System TerminologiesDocument4 pagesCirculatory System TerminologiesavduqueNo ratings yet
- Hypertensive Heart Disease: A Proposed Clinical ClassificationDocument2 pagesHypertensive Heart Disease: A Proposed Clinical ClassificationRonald Hamdani HamNo ratings yet
- 14 Cerebrovascular Accident Nursing Care PlansDocument5 pages14 Cerebrovascular Accident Nursing Care PlansHarvey T. Dato-onNo ratings yet
- Pathophysiology of CVD InfarctDocument2 pagesPathophysiology of CVD InfarctIris Caberte86% (7)
- Inflammatory Response: PathophysiologyDocument2 pagesInflammatory Response: PathophysiologySoniaMarieBalanayNo ratings yet
- Sim 2015Document16 pagesSim 2015Mary Grace A. BarridaNo ratings yet
- Saddle Pulmonary Embolism: A Rare Case of Proximal Pulmonary EmbolismDocument3 pagesSaddle Pulmonary Embolism: A Rare Case of Proximal Pulmonary EmbolismIJAR JOURNALNo ratings yet
- Icn Lec TransDocument43 pagesIcn Lec TransHannah DuyagNo ratings yet
- Circulatory and Respiratory Systems - Module 3Document47 pagesCirculatory and Respiratory Systems - Module 3CaityNo ratings yet
- SSC 8 Blood Pressure (High) CombinationDocument1 pageSSC 8 Blood Pressure (High) CombinationhimaNo ratings yet
- VASODILATORSDocument2 pagesVASODILATORSMichiko_Lois_Tao_203No ratings yet
- 5 Management of Cardiogenic ShockDocument14 pages5 Management of Cardiogenic Shockileav_2No ratings yet
- 12 Drugs Acting On The Cardiovascular SystemDocument5 pages12 Drugs Acting On The Cardiovascular SystemJAN CAMILLE LENONNo ratings yet
- Femoral Artery PDFDocument1 pageFemoral Artery PDFmittalvidushi24No ratings yet
- Stages of ShockDocument1 pageStages of ShockronaNo ratings yet
- Transcatheter Tricuspid Valve Interventions: Landscape, Challenges, and Future DirectionsDocument22 pagesTranscatheter Tricuspid Valve Interventions: Landscape, Challenges, and Future DirectionsgNo ratings yet
- Acute Ischemic Stroke TD - StudentDocument8 pagesAcute Ischemic Stroke TD - Studentapi-594366475No ratings yet
- Antiadrenergic Drugs 23.07.018 PDFDocument23 pagesAntiadrenergic Drugs 23.07.018 PDFHitesh karnNo ratings yet
- AHA Clinical Update Valvular Heart Disease PowerPoint 32321Document45 pagesAHA Clinical Update Valvular Heart Disease PowerPoint 32321Biswarup PurkayasthaNo ratings yet
- S Phy Gmo ManometerDocument4 pagesS Phy Gmo ManometerPaulo AlmeidaNo ratings yet
- Translational Research in AnatomyDocument8 pagesTranslational Research in Anatomyluthfi anggia sastiwiNo ratings yet
- Basic Concepts of Heart-Lung Interactions During Mechanical VentilationDocument14 pagesBasic Concepts of Heart-Lung Interactions During Mechanical VentilationanindiawNo ratings yet
- Anatomy Helpers Blood Supply To Abdominal OrgansDocument5 pagesAnatomy Helpers Blood Supply To Abdominal OrgansSam TagardaNo ratings yet
- Emergency Hypertension (Herbesser Injection)Document18 pagesEmergency Hypertension (Herbesser Injection)suho exoNo ratings yet
- StrokeDocument17 pagesStrokeSathias SundariNo ratings yet

























































































Download as pdf or txt
You might also like
- Buku Pegangan Kursus DSTC - FinalDocument119 pagesBuku Pegangan Kursus DSTC - FinalabdurrahmanNo ratings yet
- KS3 Blood Circulation TESTDocument4 pagesKS3 Blood Circulation TESTA.K Mon100% (1)
- Angelito L. Ramos Jr. RN Clinical InstructorDocument68 pagesAngelito L. Ramos Jr. RN Clinical Instructorraymondblade18100% (17)
- Diagnostics 11 01559 v2Document21 pagesDiagnostics 11 01559 v2Luis CortezNo ratings yet
- Lactato y Perfusion Kattan y GlennDocument5 pagesLactato y Perfusion Kattan y GlennAna Belén Artero CastañoNo ratings yet
- Rheology For CliniciansDocument8 pagesRheology For CliniciansRaluca LNo ratings yet
- 2021 CURR ORIBK CARDIOL Septic Cardiomiopathy From Basics To Management ChoicesDocument18 pages2021 CURR ORIBK CARDIOL Septic Cardiomiopathy From Basics To Management ChoicesConny MuñozNo ratings yet
- Shock Septico EvidenciaDocument8 pagesShock Septico EvidenciaFra1312No ratings yet
- Journal of Intensive Medicine: Florence Boissier, Nadia AissaouiDocument9 pagesJournal of Intensive Medicine: Florence Boissier, Nadia AissaouiMaudiel BrionesNo ratings yet
- Disseminated Intravascular Coagulopathy DICDocument24 pagesDisseminated Intravascular Coagulopathy DICMassimiliano MalerbaNo ratings yet
- Microcirculatory Alterations in Cardiac Surgery A ComprehensiveDocument10 pagesMicrocirculatory Alterations in Cardiac Surgery A ComprehensiveJuan Antonio SantosNo ratings yet
- Pathophysiology of Sepsis-Induced Myocardial Dysfunction: Review Open AccessDocument9 pagesPathophysiology of Sepsis-Induced Myocardial Dysfunction: Review Open AccessjessicaesmrldaNo ratings yet
- Microcirculacion en SepsisDocument4 pagesMicrocirculacion en Sepsis1.Bishop MasterNo ratings yet
- 10 1097@MCC 0000000000000356Document8 pages10 1097@MCC 0000000000000356Elena StepanNo ratings yet
- Sepsis-Induced Cardiomyopathy: A Comprehensive Review: Published Online: 6 May 2020Document12 pagesSepsis-Induced Cardiomyopathy: A Comprehensive Review: Published Online: 6 May 2020Alicia GarcíaNo ratings yet
- Oxygen Extraction and Perfusion Markers in Severe Sepsis and Septic Shock - Diagnostic, Therapeutic and Outcome ImplicationsDocument7 pagesOxygen Extraction and Perfusion Markers in Severe Sepsis and Septic Shock - Diagnostic, Therapeutic and Outcome Implicationshvf41327No ratings yet
- Noninvasive Hemodynamic Monitoring in The Intensive Care UnitDocument18 pagesNoninvasive Hemodynamic Monitoring in The Intensive Care UnitmegaNo ratings yet
- Vasoplegic Syndrome Following Cardiothoracic Surgery-Review of Pathophysiology and Update of Treatment Options - PMCDocument21 pagesVasoplegic Syndrome Following Cardiothoracic Surgery-Review of Pathophysiology and Update of Treatment Options - PMCluis orlando bustamante rojasNo ratings yet
- Management of Sepsis and Septic Shock in The Emergency DepartmentDocument13 pagesManagement of Sepsis and Septic Shock in The Emergency DepartmentandreaNo ratings yet
- Sepsis y Shock SepticoDocument41 pagesSepsis y Shock SepticoSilvia GarciaNo ratings yet
- DefinitionofdicDocument9 pagesDefinitionofdicDwika AudiyanandaNo ratings yet
- The Relationship Between Retinal Microvascular Abnormalities and Coronary Heart DiseaseDocument7 pagesThe Relationship Between Retinal Microvascular Abnormalities and Coronary Heart DiseaseMaria Camila RestrepoNo ratings yet
- Yjbm 92 4 629Document12 pagesYjbm 92 4 629Alfonso Ga MaNo ratings yet
- Choque Septico en CirrosisDocument19 pagesChoque Septico en CirrosisAzael HaggardNo ratings yet
- Macrocirculation and Microcirculation The Batman.39Document4 pagesMacrocirculation and Microcirculation The Batman.39Bro ManiacNo ratings yet
- 2022 Sepsis Related CardiomyopathyDocument3 pages2022 Sepsis Related Cardiomyopathystef lopezNo ratings yet
- BR J Haematol 2021 Adelborg Disseminated Intravascular CoagulationDocument16 pagesBR J Haematol 2021 Adelborg Disseminated Intravascular CoagulationSergio Alberto Sulub NavarreteNo ratings yet
- Sepsis-Induced AKI Revisited - Curr Op Crit Care 2014Document9 pagesSepsis-Induced AKI Revisited - Curr Op Crit Care 2014Vika RatuNo ratings yet
- Circulating Microvesicles in Convalescent Ischemic Stroke Patients: A Contributor To High-On-Treatment Residual Platelet Reactivity?Document7 pagesCirculating Microvesicles in Convalescent Ischemic Stroke Patients: A Contributor To High-On-Treatment Residual Platelet Reactivity?Nasdı BabayevaNo ratings yet
- The Vascular Biology of Atherosclerosis and Imaging TargetsDocument6 pagesThe Vascular Biology of Atherosclerosis and Imaging TargetsOrsid Sierra OchoaNo ratings yet
- Cerebral Venous Sinus ThrombosisDocument11 pagesCerebral Venous Sinus ThrombosisdjcafNo ratings yet
- Cardiac Involvement in Systemic SclerosisDocument7 pagesCardiac Involvement in Systemic SclerosisWisnu MataramNo ratings yet
- Management of Vasoplegic ShockDocument16 pagesManagement of Vasoplegic ShockxmksmwyspyNo ratings yet
- Micro IngenieriaDocument11 pagesMicro IngenieriaAlejandra Ramirez SanchezNo ratings yet
- Stroke Fix 1Document5 pagesStroke Fix 1Inset RiniNo ratings yet
- Intracranial AterosclerosisDocument6 pagesIntracranial AterosclerosisMarshell TendeanNo ratings yet
- HHS Public Access: Sepsis-Induced AKI Revisited: Pathophysiology, Prevention and Future TherapiesDocument13 pagesHHS Public Access: Sepsis-Induced AKI Revisited: Pathophysiology, Prevention and Future TherapiesromiNo ratings yet
- PIIS246802492301536XDocument13 pagesPIIS246802492301536XjosedegibesNo ratings yet
- Clinical Review: Myocardial Depression in Sepsis and Septic ShockDocument9 pagesClinical Review: Myocardial Depression in Sepsis and Septic ShockwasiNo ratings yet
- Sepsis Parte 1Document16 pagesSepsis Parte 1Maria AlejandraNo ratings yet
- Management of Sepsis-Induced Acute Kidney Injury: ReviewDocument12 pagesManagement of Sepsis-Induced Acute Kidney Injury: ReviewVika RatuNo ratings yet
- Clinical and Experimental Emergency MedicineDocument56 pagesClinical and Experimental Emergency MedicineAlfonso Ga MaNo ratings yet
- Https:emedicine Medscape Com:article:1227025-PrintDocument18 pagesHttps:emedicine Medscape Com:article:1227025-PrintSalsa BillaNo ratings yet
- CID Coagulación Intravascular TratamientoDocument16 pagesCID Coagulación Intravascular Tratamientoaraceli garciaNo ratings yet
- Icu Jendd2Document1 pageIcu Jendd2Jennifer AlamonNo ratings yet
- Circulation 2004 Zhu 2109 15Document8 pagesCirculation 2004 Zhu 2109 15gekayuuNo ratings yet
- Research Article: Retinal Structural and Microvascular Alterations in Different Acute Ischemic Stroke SubtypesDocument10 pagesResearch Article: Retinal Structural and Microvascular Alterations in Different Acute Ischemic Stroke SubtypesKarina NathaniaNo ratings yet
- Delta Neutrophil Index As An Early MDocument9 pagesDelta Neutrophil Index As An Early MFariz NurNo ratings yet
- Fluid Therapy and The Microcirculation in Health and Critical IllnessDocument11 pagesFluid Therapy and The Microcirculation in Health and Critical IllnessAdote DrmNo ratings yet
- Expert Statement For Management Hypovolemia in Sepsis PDFDocument8 pagesExpert Statement For Management Hypovolemia in Sepsis PDFRobi HeryantoNo ratings yet
- NIH Public Access: Author ManuscriptDocument17 pagesNIH Public Access: Author ManuscriptVictor Euclides Briones MoralesNo ratings yet
- Diastolic Dysfunction and Mortality in Severe Sepsis and Septic ShockDocument9 pagesDiastolic Dysfunction and Mortality in Severe Sepsis and Septic ShockShinohara YuusukeNo ratings yet
- Senam OtakDocument15 pagesSenam OtakDewi WulandariNo ratings yet
- Assessment of Volume Status and Fluid Responsiveness in The Emergency Department: A Systematic ApproachDocument8 pagesAssessment of Volume Status and Fluid Responsiveness in The Emergency Department: A Systematic ApproachandreaNo ratings yet
- 4ng-Komplikasi Jantung - CAP & COVIDDocument5 pages4ng-Komplikasi Jantung - CAP & COVIDsukiyantoNo ratings yet
- Sepsis and Septic Shock StrategiesDocument41 pagesSepsis and Septic Shock StrategiesBolivar IseaNo ratings yet
- HSA e Isquemia Tardia 2016Document12 pagesHSA e Isquemia Tardia 2016Ellys Macías PeraltaNo ratings yet
- Cells 11 04136 v2Document3 pagesCells 11 04136 v2ayunda rinataNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptMuhammad Dadan KurniawanNo ratings yet
- Sepsis UptodateDocument56 pagesSepsis Uptodatejosip_11No ratings yet
- Oxygen DeliveryDocument11 pagesOxygen DeliveryFatimah Syed OmarNo ratings yet
- Arterial Disorders: Definition, Clinical Manifestations, Mechanisms and Therapeutic ApproachesFrom EverandArterial Disorders: Definition, Clinical Manifestations, Mechanisms and Therapeutic ApproachesAdel BerbariNo ratings yet
- Normal Coronary Artery Dimensions in IndiansDocument6 pagesNormal Coronary Artery Dimensions in IndiansISHAN NIGAMNo ratings yet
- Ankle Brachial Index PDFDocument8 pagesAnkle Brachial Index PDFIncredibleNo ratings yet
- Effect of Progressive Muscle Relaxation Combined With Deep Breathing Technique Immediately After Aerobic Exercises On Essential HypertensionDocument2 pagesEffect of Progressive Muscle Relaxation Combined With Deep Breathing Technique Immediately After Aerobic Exercises On Essential HypertensionNetraNo ratings yet
- Circulatory System TerminologiesDocument4 pagesCirculatory System TerminologiesavduqueNo ratings yet
- Hypertensive Heart Disease: A Proposed Clinical ClassificationDocument2 pagesHypertensive Heart Disease: A Proposed Clinical ClassificationRonald Hamdani HamNo ratings yet
- 14 Cerebrovascular Accident Nursing Care PlansDocument5 pages14 Cerebrovascular Accident Nursing Care PlansHarvey T. Dato-onNo ratings yet
- Pathophysiology of CVD InfarctDocument2 pagesPathophysiology of CVD InfarctIris Caberte86% (7)
- Inflammatory Response: PathophysiologyDocument2 pagesInflammatory Response: PathophysiologySoniaMarieBalanayNo ratings yet
- Sim 2015Document16 pagesSim 2015Mary Grace A. BarridaNo ratings yet
- Saddle Pulmonary Embolism: A Rare Case of Proximal Pulmonary EmbolismDocument3 pagesSaddle Pulmonary Embolism: A Rare Case of Proximal Pulmonary EmbolismIJAR JOURNALNo ratings yet
- Icn Lec TransDocument43 pagesIcn Lec TransHannah DuyagNo ratings yet
- Circulatory and Respiratory Systems - Module 3Document47 pagesCirculatory and Respiratory Systems - Module 3CaityNo ratings yet
- SSC 8 Blood Pressure (High) CombinationDocument1 pageSSC 8 Blood Pressure (High) CombinationhimaNo ratings yet
- VASODILATORSDocument2 pagesVASODILATORSMichiko_Lois_Tao_203No ratings yet
- 5 Management of Cardiogenic ShockDocument14 pages5 Management of Cardiogenic Shockileav_2No ratings yet
- 12 Drugs Acting On The Cardiovascular SystemDocument5 pages12 Drugs Acting On The Cardiovascular SystemJAN CAMILLE LENONNo ratings yet
- Femoral Artery PDFDocument1 pageFemoral Artery PDFmittalvidushi24No ratings yet
- Stages of ShockDocument1 pageStages of ShockronaNo ratings yet
- Transcatheter Tricuspid Valve Interventions: Landscape, Challenges, and Future DirectionsDocument22 pagesTranscatheter Tricuspid Valve Interventions: Landscape, Challenges, and Future DirectionsgNo ratings yet
- Acute Ischemic Stroke TD - StudentDocument8 pagesAcute Ischemic Stroke TD - Studentapi-594366475No ratings yet
- Antiadrenergic Drugs 23.07.018 PDFDocument23 pagesAntiadrenergic Drugs 23.07.018 PDFHitesh karnNo ratings yet
- AHA Clinical Update Valvular Heart Disease PowerPoint 32321Document45 pagesAHA Clinical Update Valvular Heart Disease PowerPoint 32321Biswarup PurkayasthaNo ratings yet
- S Phy Gmo ManometerDocument4 pagesS Phy Gmo ManometerPaulo AlmeidaNo ratings yet
- Translational Research in AnatomyDocument8 pagesTranslational Research in Anatomyluthfi anggia sastiwiNo ratings yet
- Basic Concepts of Heart-Lung Interactions During Mechanical VentilationDocument14 pagesBasic Concepts of Heart-Lung Interactions During Mechanical VentilationanindiawNo ratings yet
- Anatomy Helpers Blood Supply To Abdominal OrgansDocument5 pagesAnatomy Helpers Blood Supply To Abdominal OrgansSam TagardaNo ratings yet
- Emergency Hypertension (Herbesser Injection)Document18 pagesEmergency Hypertension (Herbesser Injection)suho exoNo ratings yet
- StrokeDocument17 pagesStrokeSathias SundariNo ratings yet