Volume 8, Issue 8, August 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Macrophage Activation Syndrome Secondary
to Mixed Connective Tissue Disease: A Rare Case
in a Tertiary Care Hospital of Eastern India
Jyoti Prakash 1 , Rajdeep Porel1 , Neeraj Kumar2, Ratnadeep Biswas1, Vishnu S. Ojha 1
1
Department of General Medicine, All India Institute of Medical Sciences, Patna, Patna, IND
2
Department of Anaesthesiology, All India Institute of Medical Sciences, Patna, Patna, IND
Corresponding author: Jyoti Prakash
Abstract:- Macrophage activation syndrome (MAS) is disease, systemic lupus erythematosus and Kawasaki disease
considered a rare, potentially fatal type of secondary [2]. In this report, we present a rare case of MAS occurring
hemophagocytic lymphohistiocytosis (HLH) that occurs in the context of mixed connective tissue disorder (MCTD),
especially in cases of rheumatic diseases. 18-year- old which has rarely been associated previously.
female presented with a history of rheumatoid arthritis
who presented with fever, headache, vomiting, altered II. CASE PRESENTATION
sensorium, and abnormal limb movements. She also had
joint pains, alopecia, and oral ulcers. An 18-year-old female presented with complaints of
fever for two months, headache and vomiting for six days,
Examination revealed neurological signs, elevated altered sensorium for two days, and abnormal tightening of
inflammatory markers, and abnormal liver function. limbs for one day. The fever was low-grade (101-102°F) and
Cerebrospinal fluid analysis showed increased protein associated with chills but no rigors. She had a holocranial
levels. Urine analysis showed proteinuria. Anti- nuclear headache and experienced three to four episodes of vomiting
antibody profile indicated possible systemic lupus per day for the last six days. She had altered sensorium for
erythematosus (SLE) and rheumatoid arthritis. She two days with a reduced response to verbal commands and
developed aspiration pneumonitis during her hospital reduced speech output. For one day, she had episodes of
stay with a culture positive for Acinetobacter baumannii. abnormal body movements with tightening of all four limbs,
A diagnosis of macrophage activation syndrome (MAS) jerky movements, tongue biting, and frothy secretions from
secondary to mixed connective tissue disorder (MCTD) the mouth.
was made based on clinical and laboratory parameters.
She was started on intravenous colistin and Since the past two to three years, she has complained of
methylprednisolone, but unfortunately, she eventually joint pains involving multiple small joints (bilateral
succumbed to the overwhelming infection. metacarpophalangeal joints, proximal interphalangeal joints,
and wrist joints) and large joints (bilateral knee and ankle
Thus, in cases of MCTD, MAS can manifest as a life- joints). The pain was worse in the mornings and resulted in
threatening condition. Therefore, it is crucial to maintain restricted joint movement due to the severity, gradually
a high level of clinical suspicion for MAS in resolving as the day progressed. The pain was severe enough
rheumatological diseases to enable early initiation of to hamper activities of daily living. Additionally, she has
treatment with steroids or other immunomodulatory experienced on and off alopecia and recurrent oral ulcers for
agents. the past two years. There was no history of any rashes. She
was diagnosed as a case of rheumatoid arthritis at another
Categories: Internal Medicine, Infectious Disease, facility, with rheumatoid factor levels of 90 and 78 units per
Rheumatology. milliliter on consecutive testing. Her medication history
included regular intake of pain killers (non-steroidal anti-
Keywords:- Immune dysregulation syndrome, systemic lupus inflammatory drugs) for the last two to three years.
erythematosus, hemophagocytic lymphohistiocytosis, mixed
connective tissue disease, macrophage activation syndrome. On examination, the patient was drowsy with a
Glasgow Coma Scale score of E2V2M5. Her vitals showed a
I. INTRODUCTION raised temperature (100.5°F) and blood pressure of 100/60
millimeters of mercury. Pallor was present.
Macrophage activation syndrome (MAS) is considered
a rare, potentially fatal type of secondary hemophagocytic Examination of the central nervous system revealed
lymphohistiocytosis (HLH) that occurs especially in cases of neck stiffness, a positive Kernig's sign, bilateral mid- dilated
rheumatic diseases [1]. The distinguishing feature of this pupils responsive to light, increased tone of the bilateral
condition involves an abnormal increase in the activation and upper limbs and the left lower limb, exaggerated deep tendon
proliferation of T cells and macrophages, resulting in reflexes, and an extensor plantar reflex on the right side,
elevated cytokine levels and the occurrence of along with an equivocal plantar reflex on the left. Higher
hemophagocytosis. It has been associated most commonly mental functions, the rest of the motor functions, and the
with systemic juvenile idiopathic arthritis (SJIA), Still’s sensory system could not be assessed. Examination of the
IJISRT23AUG1138 www.ijisrt.com 1084
Volume 8, Issue 8, August 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
abdomen revealed hepatomegaly (felt 3 cm below the costal (mg/dL), fibrinogen levels of 112 mg/dL, and rheumatoid
margin) and a just palpable spleen. On musculoskeletal factor levels of 88 units per milliliter. The anti-cyclic
system examination, no joint deformity or signs of citrullinated peptide levels were within normal range. The
inflammation could be noticed. No joint tenderness could be liver function test revealed aspartate aminotransferase (AST)
elicited. The rest of the systemic examination was levels of 776 units per liter (U/L), alanine aminotransferase
unremarkable. levels (ALT) of 111 U/L, and alkaline phosphatase (ALP)
levels of 405 U/L. The cerebrospinal fluid analysis showed
The differentials considered were subacute acellular cytology, elevated protein levels of 140 mg/dL,
meningoencephalitis, connective tissue disorder (systemic normal glucose levels of 60 mg/dL, normal adenosine
lupus erythematosus [SLE] with neurolupus, and polyarthritis deaminase (ADA) levels of 4 international units per liter
(rheumatoid arthritis). (IU/L), negative staining for specific microorganisms, sterile
culture, negative results for Japanese encephalitis and
Her blood investigations showed a hemoglobin level of Epstein-Barr virus, and equivocal results for herpes simplex
10.1 grams per deciliter, white blood cell count of 4000 cells virus. Additional tests revealed normal chest x-ray and
per deciliter, platelet count of 102,000 cells per deciliter, C- electrocardiography findings, along with bilateral mild
reactive protein levels of 16 milligrams per liter, an pleural effusion observed in the abdominal ultrasound. The
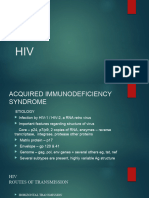
erythrocyte sedimentation rate of 79 millimeters per hour, magnetic resonance imaging (MRI) of the brain was normal
serum ferritin levels of 1650 micrograms per liter (μg/L), (Figure 1).
serum triglyceride levels of 833 milligrams per deciliter
Fig. 1: Magnetic resonance imaging (MRI) of the brain showingnormal study
The patient's urine showed 2+ proteinuria. Both blood possible underlying conditions. Complement levels showed
and urine cultures were sterile. The 24-hour urinary reduced C3 and lower side of normal C4.
proteinuria was 632 mg/day, but urinary creatinine was three
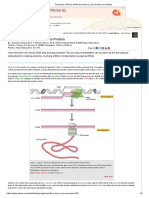
times less than normal, suggesting inadequate sampling. The During the patient's hospital stay, notable events
anti-nuclear antibody (ANA) screening was negative but the included drowsiness and delayed arousal on day two,
ANA profile revealed elevated U1 RNP (3+) and Anti Ro-60 followed by a generalized tonic-clonic seizure and aspiration
(3+), suggesting ANA-negative systemic lupus pneumonitis which evolved into acute respiratory distress
erythematosus (SLE) and rheumatoid arthritis (RA) as syndrome (Figure 2).
Fig. 2: Chest radiograph with the arrow pointing to consolidation in the lungs
IJISRT23AUG1138 www.ijisrt.com 1085
Volume 8, Issue 8, August 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
The patient was intubated and shifted to the medical sensitivity analysis of the endotracheal tube aspirate showed
intensive care unit. On day three, a diagnosis of MAS growth of Acinetobacter baumannii sensitive to colistin only.
secondary due to MCTD was made. The culture and The trend of blood investigations is given in Table 1.
Table 1: Trend of blood investigations over the course of hospital stay
Parameter (unit) Reference Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 8
range
Hemoglobin (grams per deciliter) 12-16 10.1 9.5 10 8.1 8.2 7.8 8.3 9
White blood cells (cells per cubic 4,000- 4,000 10,600 9,500 4,580 8,780 6,200 6,800 20,000
millimeter) 10,000
Platelet count (cells per cubic 150,000- 102,000 144,000 135,000 150,000 149,000 95,000 120,000 202,000
millimeter) 450,000
Alanine transaminase (units per liter) 10-28 135 111 121 - - - 55.3 -
Aspartate transaminase (units per liter) <31 656 776 531 - - - 203.5 -
Urea (milligrams per deciliter) 13-43 83 74 99 103.1 129.5 126.4 119 129.1
Creatinine (milligrams per deciliter) 0.7-1.3 1.25 1.25 1.33 1.36 1.41 1.15 1.34 1.60
C-reactive protein (milligrams per liter) <5 16 - 40 40.6 37.9 - 196.2 193.3
The patient was started on intravenous colistin and Still’s disease [5]. Recently other rheumatological conditions
pulse dose of methyl prednisolone. However, the patient's are also being implicated increasingly such as childhood-
condition deteriorated, leading to cardiac arrest and eventual onset SLE (with incidence of nearly 10% of the patients
death on day eight. developing MAS) [6], and Kawasaki disease (in 1-2% of the
patients) [7]. It has also been reported in the background of
III. DISCUSSION dermatomyositis, antiphospholipid syndrome, polyarticular
juvenile idiopathic arthritis, and very few cases of MCTD [8].
Macrophage activation syndrome is marked by an
exaggerated inflammatory response involving uncontrolled The HLH-2004 criteria developed by the International
activation and proliferation of T lymphocytes and Histiocyte Society, are used for diagnosing cases of HLH [9].
macrophages, resulting in excessive secretion of Due to the presence of persistent fever, cytopenias, elevated
proinflammatory cytokines [3]. It closely shares its levels of triglyceride and ferritin, and decreased levels of
pathophysiology with HLH, and many of its clinical features, fibrinogen, the criteria were fulfilled in our case. However,
including fever, organomegaly, cytopenias, elevated the HLH-2004 criteria are often not suitable for diagnosing
triglycerides, liver dysfunction, and elevated acute-phase MAS with underlying rheumatic diseases like SJIA due to the
reactants, are thought to be caused by the cytokine storm [4]. overlap of features, such as elevated ferritin levels and
Indeed, there is a belief that MAS is essentially synonymous splenomegaly, in active SJIA. This overlap makes it hard to
with HLH. However, the term MAS is typically used distinguish MAS from a flare-up of SJIA [10], and thus, the
specifically when it is associated with rheumatic diseases. Ravelli criteria is commonly employed for diagnosing MAS
[11], and it requires fulfilling two or more laboratory criteria
MAS has been commonly associated with systemic or any two or more clinical and/or laboratory criteria (Table
juvenile idiopathic arthritis (around 10% of patients with 2).
SJIA progress to develop evident MAS) and adult-onset
Table 2: Ravelli criteria for the diagnosis of Macrophage Activation Syndrome
Laboratory Reduced platelet count (≤262,000 cells per microliter)
criteria Elevated aspartate aminotransferase (>59 units per liter)
Reduced white blood count (≤4,000 cells per microliter)
Hypofibrinogenemia (≤2.5 grams per liter)
Clinical Central nervous system dysfunction (irritability, disorientation, lethargy, headache, seizures, coma)
criteria Hemorrhages (purpura, easy bruising, mucosal bleeding)
Hepatomegaly (≥3 centimeters below the costal margin)
The diagnosis is established when two or more laboratory criteria, or a combination of two or more clinical and/or
laboratory criteria, are fulfilled.
In this case, the presence of decreased platelet count, Our patient also fulfilled the criteria developed by
elevated AST levels, decreased white blood cell count, Parodi et al. [12] for the preliminary diagnosis of MAS in
central nervous system dysfunction, and hepatomegaly, rheumatological conditions, particularly juvenile systemic
coupled with the ANA-profile, led to the diagnosis of MAS lupus erythematosus (SLE). These criteria, outlined in Table
secondary to MCTD, according to the Ravelli criteria. 3, can be utilized for assessment.
IJISRT23AUG1138 www.ijisrt.com 1086
Volume 8, Issue 8, August 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Table 3: The Parodi criteria for diagnosis of macrophage activation syndrome
Clinical criteria Fever (>38°C)
Hepatomegaly (≥3 centimeters below the costal arch)
Splenomegaly (≥3 centimeters below the costal arch)
Hemorrhagic manifestations (purpura, easy bruising, or mucosal bleeding)
Central nervous system dysfunction (irritability, disorientation, lethargy, headache, seizures,
or coma)
Laboratory criteria Cytopenia affecting two or more cell lineages (white blood cell count ≤4,000 cells per
microliter, hemoglobin ≤9 grams per deciliter, or platelet count ≤150,000 cells per microliter)
Elevated aspartate transaminase (>40 units per liter)
Elevated lactate dehydrogenase (>567 units per liter)
Hypofibrinogenemia (≤150 milligrams per deciliter)
Hypertriglyceridemia (>178 milligrams per deciliter)
Hyperferritinemia (>500 micrograms per liter)
Histopathological Evidence of hemophagocytosis in the bone marrow aspirate
criterion
The diagnosis of macrophage activation syndrome: at least 1 clinical criterion and at least 2 laboratory criteria. Bone
marrow aspiration for evidence of macrophage hemophagocytosis may be required only in doubtful cases.
Early detection and prompt therapeutic intervention are REFERENCES
of utmost importance in managing MAS, a potentially fatal
condition with significant mortality rates. Timely recognition [1.] Sawhney S, Woo P, Murray KJ: Macrophage
of MAS symptoms and immediate initiation of appropriate activation syndrome: a potentially fatal complication
treatments are essential to achieve a swift and effective of rheumatic disorders. Arch Dis Child. 2001, 85:421-
response [10]. Steroids are often the first line of treatment for 6. 10.1136/adc.85.5.421
cases of MAS. Cyclosporine A and tumor necrosis factor [2.] Ravelli A, Davì S, Minoia F, Martini A, Cron RQ:
alpha inhibitors have also proven quite effective in many Macrophage activation syndrome. Hematol Oncol
cases [13,14]. Despite the administration of steroid therapy, Clin North Am. 2015, 29:927-41.
our patient's condition proved fatal due to the combination of 10.1016/j.hoc.2015.06.010
immune dysregulation leading to overwhelming sepsis and [3.] Ravelli A, Minoia F, Davì S, et al.: 2016 Classification
the resulting damage caused by hypercytokinemia. criteria for macrophage activation syndrome
complicating systemic juvenile idiopathic arthritis: a
IV. CONCLUSIONS european league against rheumatism/american college
of rheumatology/paediatric rheumatology
In cases of mixed connective tissue disease (MCTD), international trials organisation collaborative
MAS can manifest as a life-threatening condition. Therefore, initiative. Arthritis Rheumatol. 2016, 68:566-76.
it is crucial to maintain a high level of clinical suspicion for 10.1002/art.39332.
MAS in rheumatological diseases to enable early initiation of [4.] Henderson LA, Cron RQ: Macrophage activation
treatment with steroids or other immunomodulatory agents. syndrome and secondary hemophagocytic
Given the immune dysregulation associated with MAS, the lymphohistiocytosis in childhood inflammatory
risk of overwhelming infections is increased, necessitating disorders: diagnosis and management. Paediatr Drugs.
aggressive antimicrobial therapy. 2020, 22:29-44. 10.1007/s40272-019-00367-1
[5.] Minoia F, Davì S, Horne A, et al.: Clinical features,
ADDITIONAL INFORMATION treatment, and outcome of macrophage activation
DISCLOSURES syndrome complicating systemic juvenile idiopathic
arthritis: a multinational, multicenter study of 362
Human subjects: All authors have confirmed that this
patients. Arthritis Rheumatol. 2014, 66:3160-9.
study did not involve human participants or tissue.
10.1002/art.38802
Conflicts of interest: In compliance with the ICMJE [6.] Borgia RE, Gerstein M, Levy DM, Silverman ED,
uniform disclosure form, all authors declare the Hiraki LT: Features, treatment, and outcomes of
following: macrophage activation syndrome in childhood-onset
systemic lupus erythematosus. Arthritis Rheumatol.
Payment/services info: All authors have declared that no 2018, 70:616-24. 10.1002/art.40417.
financial support was received from any organization for
the submitted work. Financial relationships: All authors
have declared that they have no financial relationships at [7.] Latino GA, Manlhiot C, Yeung RSM, Chahal N,
present or within the previous three years with any McCrindle BW: Macrophage activation syndrome in
organizations that might have an interest in the submitted the acute phase of kawasaki disease. J Pediatr Hematol
work. Other relationships: All authors have declared that Oncol. 2010, 32:527-31.
there are no other relationships or activities that could [8.] 10.1097/MPH.0b013e3181dccbf4
appear to have influenced the submitted work.
IJISRT23AUG1138 www.ijisrt.com 1087
Volume 8, Issue 8, August 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[9.] Sen ES, Clarke SLN, Ramanan AV: Macrophage
activation syndrome. Indian J Pediatr. 2016, 83:248-
53. 10.1007/s12098-015-1877-1
[10.] Henter J-I, Horne A, Aricó M, et al.: HLH-2004:
diagnostic and therapeutic guidelines for
hemophagocytic lymphohistiocytosis. Pediatr Blood
Cancer. 2007, 48:124-31. 10.1002/pbc.21039
[11.] Schulert GS, Grom AA: Pathogenesis of macrophage
activation syndrome and potential for cytokine-
directed therapies. Annu Rev Med. 2015, 66:145-59.
10.1146/annurev-med-061813-012806
[12.] Ravelli A, Magni-Manzoni S, Pistorio A, et al.:
Preliminary diagnostic guidelines for macrophage
activation syndrome complicating systemic juvenile
idiopathic arthritis. J Pediatr. 2005, 146:598-604.
[13.] Parodi A, Davì S, Pringe AB, et al.: Macrophage
activation syndrome in juvenile systemic lupus
erythematosus: a multinational multicenter study of
thirty-eight patients. Arthritis Rheumat. 2009,
60:3388-99. 10.1002/art.24883
[14.] Mouy R, Stephan JL, Pillet P, Haddad E, Hubert P,
Prieur AM: Efficacy of cyclosporine A in the
treatment of macrophage activation syndrome in
juvenile arthritis: report of five cases. J Pediatr. 1996,
129:750-4.
[15.] Kelly A, Ramanan AV: A case of macrophage
activation syndrome successfully treated with
anakinra . Nat Clin Pract Rheumatol. 2008, 4:615-20.
10.1038/ncprheum0919
IJISRT23AUG1138 www.ijisrt.com 1088
You might also like
- Case ReportDocument5 pagesCase ReportsyahputriNo ratings yet
- Tuberculous Transverse Myelitis: Case Report and Review of The LiteratureDocument7 pagesTuberculous Transverse Myelitis: Case Report and Review of The LiteraturenoraNo ratings yet
- Case Report: Lepra Reaction With Lucio Phenomenon Mimicking Cutaneous VasculitisDocument5 pagesCase Report: Lepra Reaction With Lucio Phenomenon Mimicking Cutaneous VasculitisadibahtiarNo ratings yet
- Secondary Hemophagocytic Lymphohistiocytosis: A Rare Case ReportDocument5 pagesSecondary Hemophagocytic Lymphohistiocytosis: A Rare Case ReportivanNo ratings yet
- Medicine: Systemic Lupus Erythematosus With Guillian - Barre SyndromeDocument5 pagesMedicine: Systemic Lupus Erythematosus With Guillian - Barre SyndromeShri RamNo ratings yet
- Jurding 2Document4 pagesJurding 2fileochaNo ratings yet
- CHSJ 45 03 12 2019Document8 pagesCHSJ 45 03 12 2019mihail.boldeanuNo ratings yet
- Lupus 2024Document12 pagesLupus 2024MarcoNo ratings yet
- Guillain Barr Syndrome Occurring Synchronously With Systemic Lupus Erythematosus As Initial Manifestation Treated Successfully With Low DoseDocument5 pagesGuillain Barr Syndrome Occurring Synchronously With Systemic Lupus Erythematosus As Initial Manifestation Treated Successfully With Low DoseTessa CruzNo ratings yet
- Pancytopenia Secondary To Methotrexate Therapy in Rheumatoid ArthritisDocument5 pagesPancytopenia Secondary To Methotrexate Therapy in Rheumatoid ArthritisShaysta KhanNo ratings yet
- Recurrent Mycobacterium Tuberculosis Infection in Systemic Lupus Erythematosus Patient Case Report and ReviewDocument8 pagesRecurrent Mycobacterium Tuberculosis Infection in Systemic Lupus Erythematosus Patient Case Report and ReviewpaulallenfileNo ratings yet
- Q2 GPA Infectious Diseases IIDocument9 pagesQ2 GPA Infectious Diseases IIAdrian CaballesNo ratings yet
- Anetodermic Lupus Panniculitis and Antiphospholipid Antibodies: Report of Three CasesDocument4 pagesAnetodermic Lupus Panniculitis and Antiphospholipid Antibodies: Report of Three CasesDermatologie VenerologieNo ratings yet
- Abdominal Pain and Seizure in A 4-Year-Old Boy: PresentationDocument5 pagesAbdominal Pain and Seizure in A 4-Year-Old Boy: PresentationWiti Triple'sNo ratings yet
- 2017 32 3 264 267 EngDocument4 pages2017 32 3 264 267 Engemmanuellagrace06No ratings yet
- Respiratory and Pulmonary Medicine: ClinmedDocument3 pagesRespiratory and Pulmonary Medicine: ClinmedGrace Yuni Soesanti MhNo ratings yet
- Management of Septic ShockDocument33 pagesManagement of Septic ShockswatisinghnigeriaNo ratings yet
- 2104 Meningoencephalitis Due To Enteroviral Infection An Often Overlooked EtiologyDocument4 pages2104 Meningoencephalitis Due To Enteroviral Infection An Often Overlooked EtiologyRonald Ivan WijayaNo ratings yet
- Tsoi 1997Document7 pagesTsoi 1997Araceli Enríquez OvandoNo ratings yet
- Typhoid Encephalopathy As A Neuropsychiatric Manifestation of SalmonellosisDocument2 pagesTyphoid Encephalopathy As A Neuropsychiatric Manifestation of SalmonellosisFar CanakanNo ratings yet
- 1-s2.0-S1665268119318174-mainDocument3 pages1-s2.0-S1665268119318174-mainmarcelofabianamantepatologiaNo ratings yet
- Oxford University PressDocument9 pagesOxford University PresssarafraunaqNo ratings yet
- R Art 42778-10Document8 pagesR Art 42778-10Kevin Wladimir ChanchicochaNo ratings yet
- Artigo Base SimoneDocument5 pagesArtigo Base SimoneWolfgang ThyerreNo ratings yet
- G6Written Output - Blood Physio SGD 4th Aug 2023Document11 pagesG6Written Output - Blood Physio SGD 4th Aug 2023RUTUJA DILIP GADENo ratings yet
- 26 Mip CC 29 Teodor Andra C 808-811Document4 pages26 Mip CC 29 Teodor Andra C 808-811ana2693No ratings yet
- 0717 9227 RCHNP 57 03 0283Document12 pages0717 9227 RCHNP 57 03 0283Araceli PerezNo ratings yet
- Case Reports of RhupusDocument4 pagesCase Reports of RhupusSalwiyadiNo ratings yet
- An Unusual Presenting Symptom of Graves' Disease: Myalgia: Clinical Thyroidology / Original PaperDocument3 pagesAn Unusual Presenting Symptom of Graves' Disease: Myalgia: Clinical Thyroidology / Original PaperDian WalineloNo ratings yet
- April 2019 1554202000 8152018Document2 pagesApril 2019 1554202000 8152018KantiNareshNo ratings yet
- Marine-Lenhart Syndrome Case ReportDocument5 pagesMarine-Lenhart Syndrome Case ReportEliana InsaurraldeNo ratings yet
- Poster LESDocument6 pagesPoster LESAlejandra LuqueNo ratings yet
- Mediterranean Spotted Fever With Encephalitis: Case ReportDocument5 pagesMediterranean Spotted Fever With Encephalitis: Case Reportracut_khansatraNo ratings yet
- International Journal of Pharmaceutical Science Invention (IJPSI)Document3 pagesInternational Journal of Pharmaceutical Science Invention (IJPSI)inventionjournalsNo ratings yet
- Adult Still's Disease and Respiratory Failure in A 74 Year Old WomanDocument3 pagesAdult Still's Disease and Respiratory Failure in A 74 Year Old WomanEduardo Romero StéfaniNo ratings yet
- 72 - Progressive Multifocal Leukoencephalopathy in An Immunocompetent PatientDocument7 pages72 - Progressive Multifocal Leukoencephalopathy in An Immunocompetent PatientFaras ArinalNo ratings yet
- Evans Syndrome As The Initial Presentation of Systemic Lupus Erythromatosus in A Rural Kenyan Hospital: A Case ReportDocument4 pagesEvans Syndrome As The Initial Presentation of Systemic Lupus Erythromatosus in A Rural Kenyan Hospital: A Case ReportNovelty JournalsNo ratings yet
- Two Takayasu Arteritis Patients Successfully Treated With Infliximab: A Potential Disease-Modifying Agent?Document8 pagesTwo Takayasu Arteritis Patients Successfully Treated With Infliximab: A Potential Disease-Modifying Agent?tera95No ratings yet
- Acute Liver Failure in Dengue Shock SyndromeDocument3 pagesAcute Liver Failure in Dengue Shock SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Enfermedad MitocondrialDocument4 pagesEnfermedad Mitocondrialdoc_torresNo ratings yet
- Leptospirosis Presenting As Severe Cardiogenic Shock: A Case ReportDocument3 pagesLeptospirosis Presenting As Severe Cardiogenic Shock: A Case ReportFirdha GitaNo ratings yet
- A Curious Case of QuadriplegiaDocument4 pagesA Curious Case of QuadriplegiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- DownloadDocument3 pagesDownloadstudentstoma61No ratings yet
- A Case of Male Sle: An Unusual PresentationDocument4 pagesA Case of Male Sle: An Unusual PresentationIJAR JOURNALNo ratings yet
- Allopurinol-Induced Drug Reactions With Eosinophilia and Systemic Symptoms Syndrome With Interstitial NephritisDocument12 pagesAllopurinol-Induced Drug Reactions With Eosinophilia and Systemic Symptoms Syndrome With Interstitial NephritisJoc HerreraNo ratings yet
- Hashimoto'S Encephalopathy: Renata Telles Rudge de Aquino, Eduardo Genaro MutarelliDocument2 pagesHashimoto'S Encephalopathy: Renata Telles Rudge de Aquino, Eduardo Genaro Mutarellisergioqueiroz6452No ratings yet
- Juvenile Rheumatoid ArthritisDocument30 pagesJuvenile Rheumatoid ArthritisAnonymous dFSZ2k2IUNo ratings yet
- Cutaneous Lupus Erythematosus: SGD B3Document41 pagesCutaneous Lupus Erythematosus: SGD B3Che Haniff100% (2)
- Mixed Connective Tissue Disease That WasDocument10 pagesMixed Connective Tissue Disease That Wassaideh naghibiNo ratings yet
- Hunter Syndrome A Case ReportDocument4 pagesHunter Syndrome A Case ReportResearch ParkNo ratings yet
- Severe Dermatomyositis With Pronounced GeneralizedDocument4 pagesSevere Dermatomyositis With Pronounced Generalizedvasquezdario29No ratings yet
- Caso de EncefalitisDocument4 pagesCaso de EncefalitisJonathan CuevaNo ratings yet
- Involvement of MnSOD Ala16Val Polymorphism in Epilepsy A Relationship With Seizure TypeDocument6 pagesInvolvement of MnSOD Ala16Val Polymorphism in Epilepsy A Relationship With Seizure TypeDetector BotsNo ratings yet
- Germinoma With Involvement of Midline and Off-Midline Intracranial StructuresDocument6 pagesGerminoma With Involvement of Midline and Off-Midline Intracranial StructuresDiah LubisNo ratings yet
- Clinical and Pathological Findings of Necrotizing Meningoencephalitis in A Maltese Dog.Document6 pagesClinical and Pathological Findings of Necrotizing Meningoencephalitis in A Maltese Dog.ISABEL RODRIGUES ROSADONo ratings yet
- JurnalDocument9 pagesJurnalMelita Amalia AyubaNo ratings yet
- Case 14-2020: A 37-Year-Old Man With Joint Pain and Eye RednessDocument9 pagesCase 14-2020: A 37-Year-Old Man With Joint Pain and Eye RednessWho's Alewii?No ratings yet
- Barsoum 2004Document13 pagesBarsoum 2004Bruno MoraesNo ratings yet
- 1981-Case Report-9103-1-10-20201002Document6 pages1981-Case Report-9103-1-10-20201002irsyah dwi rNo ratings yet
- A Comprehensive Review on the Therapeutic Potential of PectinDocument6 pagesA Comprehensive Review on the Therapeutic Potential of PectinInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Quizlet's Usefulness for Vocabulary Learning: Perceptions of High-Level and Low-Level Chinese College EFL LearnersDocument5 pagesQuizlet's Usefulness for Vocabulary Learning: Perceptions of High-Level and Low-Level Chinese College EFL LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Rare Complication: Cardiac Arrest and Pulmonary Embolism in Polyarteritis NodosaDocument5 pagesA Rare Complication: Cardiac Arrest and Pulmonary Embolism in Polyarteritis NodosaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Forecasting PM10 Concentrations Using Artificial Neural Network in Imphal CityDocument10 pagesForecasting PM10 Concentrations Using Artificial Neural Network in Imphal CityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Integrated Border Security System on Human Trafficking in Bangladesh: The Mediating Effect of the Use of Advanced TechnologyDocument12 pagesThe Impact of Integrated Border Security System on Human Trafficking in Bangladesh: The Mediating Effect of the Use of Advanced TechnologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Application of Project Management using CPM (Critical Path Method) and Pert (Project Evaluation and Review Technique) in the Nava House Bekasi Cluster Housing Development ProjectDocument12 pagesApplication of Project Management using CPM (Critical Path Method) and Pert (Project Evaluation and Review Technique) in the Nava House Bekasi Cluster Housing Development ProjectInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Quality Control to Reduce Appearance Defects at PT. Musical InstrumentDocument11 pagesQuality Control to Reduce Appearance Defects at PT. Musical InstrumentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Application of the Economic Order Quantity (EOQ) Method on the Supply of Chemical Materials in the Laboratory of PT. Fajar Surya Wisesa TbkDocument15 pagesApplication of the Economic Order Quantity (EOQ) Method on the Supply of Chemical Materials in the Laboratory of PT. Fajar Surya Wisesa TbkInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of Carton Packaging Quality Control Using Statistical Quality Control Methods at PT XYZDocument10 pagesAnalysis of Carton Packaging Quality Control Using Statistical Quality Control Methods at PT XYZInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Visitor Perception Related to the Quality of Service in Todo Tourism VillageDocument10 pagesVisitor Perception Related to the Quality of Service in Todo Tourism VillageInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Entrepreneurial Adult Education as a Catalyst for Youth Employability in Disadvantaged AreasDocument9 pagesEntrepreneurial Adult Education as a Catalyst for Youth Employability in Disadvantaged AreasInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A New Model of Rating to Evaluate Start-ups in Emerging Indian MarketDocument7 pagesA New Model of Rating to Evaluate Start-ups in Emerging Indian MarketInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Enhancing Estimating the Charge Level in Electric Vehicles: Leveraging Force Fluctuation and Regenerative Braking DataDocument6 pagesEnhancing Estimating the Charge Level in Electric Vehicles: Leveraging Force Fluctuation and Regenerative Braking DataInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Proof of Concept Using BLE to Optimize Patients Turnaround Time (PTAT) in Health CareDocument14 pagesA Proof of Concept Using BLE to Optimize Patients Turnaround Time (PTAT) in Health CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Health Care - An Android Application Implementation and Analyzing user Experience Using PythonDocument7 pagesHealth Care - An Android Application Implementation and Analyzing user Experience Using PythonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Gravity Investigations Applied to the Geological Framework Study of the Mambasa Territory in Democratic Republic of CongoDocument9 pagesGravity Investigations Applied to the Geological Framework Study of the Mambasa Territory in Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrusion Detection System with Ensemble Machine Learning Approaches using VotingClassifierDocument4 pagesIntrusion Detection System with Ensemble Machine Learning Approaches using VotingClassifierInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Crop Monitoring System with Water Moisture Levels Using ControllerDocument8 pagesCrop Monitoring System with Water Moisture Levels Using ControllerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Naturopathic Approaches to Relieving Constipation: Effective Natural Treatments and TherapiesDocument9 pagesNaturopathic Approaches to Relieving Constipation: Effective Natural Treatments and TherapiesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Developing Digital Fluency in Early Education: Narratives of Elementary School TeachersDocument11 pagesDeveloping Digital Fluency in Early Education: Narratives of Elementary School TeachersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Synthetic and Natural Vitamin C Modulation of Leaded Paint-Induced Nephrotoxicity of Automobile Painters in Ile-Ife, Nigeria.Document21 pagesSynthetic and Natural Vitamin C Modulation of Leaded Paint-Induced Nephrotoxicity of Automobile Painters in Ile-Ife, Nigeria.International Journal of Innovative Science and Research TechnologyNo ratings yet
- Optimizing Bio-Implant Materials for Femur Bone Replacement:A Multi-Criteria Analysis and Finite Element StudyDocument5 pagesOptimizing Bio-Implant Materials for Femur Bone Replacement:A Multi-Criteria Analysis and Finite Element StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Study to Assess the Effectiveness of Bronchial Hygiene Therapy (BHT) on Clinical Parameters among Mechanically Ventilated Patients in Selected Hospitals at ErodeDocument7 pagesA Study to Assess the Effectiveness of Bronchial Hygiene Therapy (BHT) on Clinical Parameters among Mechanically Ventilated Patients in Selected Hospitals at ErodeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Year Wise Analysis and Prediction of Gold RatesDocument8 pagesYear Wise Analysis and Prediction of Gold RatesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Government's Role in DMO-based Urban Tourism in Kayutangan area of Malang cityDocument8 pagesThe Government's Role in DMO-based Urban Tourism in Kayutangan area of Malang cityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design and Implementation of Software-Defined ReceiverDocument8 pagesDesign and Implementation of Software-Defined ReceiverInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fahfi/Mochaina Illegal Gambling Activities and its Average Turnover within Limpopo ProvinceDocument8 pagesFahfi/Mochaina Illegal Gambling Activities and its Average Turnover within Limpopo ProvinceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Inclusive Leadership in the South African Police Service (SAPS)Document26 pagesInclusive Leadership in the South African Police Service (SAPS)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Effectiveness of Organizing Crossing Transport Services in the Maritime Area of Riau Islands ProvinceDocument10 pagesEffectiveness of Organizing Crossing Transport Services in the Maritime Area of Riau Islands ProvinceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Income Diversification of Rural Households in Bangladesh (2022-23)Document5 pagesIncome Diversification of Rural Households in Bangladesh (2022-23)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Bio 110 - Ch8 (Animal)Document65 pagesBio 110 - Ch8 (Animal)محسن الشاطريNo ratings yet
- HB-2641-002 R2 QIAstat-Dx Gastro-Pan CE 0920 ROWDocument84 pagesHB-2641-002 R2 QIAstat-Dx Gastro-Pan CE 0920 ROWAngélica Sarahí Chiroy SicánNo ratings yet
- Soapy - Value Proposition BrochureDocument5 pagesSoapy - Value Proposition Brochuresouarbh khemkaNo ratings yet
- Etextbook 978 0323319676 Andrews Diseases of The Skin Clinical DermatologyDocument61 pagesEtextbook 978 0323319676 Andrews Diseases of The Skin Clinical Dermatologyeric.chandler298100% (60)
- Human Cardiac Information Questions WorksheetDocument5 pagesHuman Cardiac Information Questions Worksheetgardereynoso14No ratings yet
- Social Studies Class V Worksheet Lesson 11Document2 pagesSocial Studies Class V Worksheet Lesson 11Rashi BakshNo ratings yet
- Carcinoembryonic AntigenDocument9 pagesCarcinoembryonic AntigenKatrina Ramos PastranaNo ratings yet
- LMC CursDocument31 pagesLMC CursEma ȚurcașNo ratings yet
- Worksheet in Bio 102: Microbiology and Parasitology - Week No. 3Document4 pagesWorksheet in Bio 102: Microbiology and Parasitology - Week No. 3DELOS SANTOS JESSIECAHNo ratings yet
- Enzymes PresDocument14 pagesEnzymes PresSaeed Ahmad Zeb100% (1)
- HIVDocument35 pagesHIVtejaswi71117No ratings yet
- Biology Part2 BIJUSDocument271 pagesBiology Part2 BIJUSDebasish BhattacharyyaNo ratings yet
- Bio Biological Molecules AlevelsDocument28 pagesBio Biological Molecules AlevelsMunazzagulNo ratings yet
- Cureus 0008 000000000515 PDFDocument12 pagesCureus 0008 000000000515 PDFDini WurnaningNo ratings yet
- Genetic Engineering Assignment Bacterial Artificial Chromosome (Bac) and Yeast Artificial Chromosome (Yac)Document5 pagesGenetic Engineering Assignment Bacterial Artificial Chromosome (Bac) and Yeast Artificial Chromosome (Yac)Hairil FiqriNo ratings yet
- ISBB Aaaaa PDFDocument55 pagesISBB Aaaaa PDFSelena de LimaNo ratings yet
- AST and Dosing Info Card - FINALDocument2 pagesAST and Dosing Info Card - FINALGAYATHIRINo ratings yet
- Ch. 18 Reading Guide Ed8Document10 pagesCh. 18 Reading Guide Ed8quinntai97No ratings yet
- Assignment 1 - ALMOITEDocument1 pageAssignment 1 - ALMOITERenz DominicNo ratings yet
- Frac List of Plant Pathogenic Organisms Resistant To Disease Control AgentsDocument75 pagesFrac List of Plant Pathogenic Organisms Resistant To Disease Control AgentsGeraldNo ratings yet
- Natural Compounds As Antimicrobial AgentsDocument324 pagesNatural Compounds As Antimicrobial AgentsSaad HassanNo ratings yet
- Translation Dna To Mrna To ProteinDocument5 pagesTranslation Dna To Mrna To ProteinAna MarianaNo ratings yet
- BioFire RP2 1 RP2 1plus Control Panel M441Document4 pagesBioFire RP2 1 RP2 1plus Control Panel M441Cecil James BuguisNo ratings yet
- Pomegranate: Natural Remedy For Treating Periodontal DiseaseDocument5 pagesPomegranate: Natural Remedy For Treating Periodontal DiseaseVenosha RajenNo ratings yet
- HepatitisDocument10 pagesHepatitisBheru LalNo ratings yet
- Bacterial Culture MediaDocument10 pagesBacterial Culture Medianosila_oz854No ratings yet
- Indira Gandhi Krishi Vishwavidyalaya College of Agriculture, Raipur Presentation On-Artificial Chromosome and Its UsesDocument16 pagesIndira Gandhi Krishi Vishwavidyalaya College of Agriculture, Raipur Presentation On-Artificial Chromosome and Its Usespallavi sharmaNo ratings yet
- Lisa Chem Biology Exam 2008Document21 pagesLisa Chem Biology Exam 2008Vy PhanNo ratings yet
- UntitledDocument557 pagesUntitledКатя КавалджиеваNo ratings yet
- COMPLETE BLOOD COUNT Lecture GuideDocument9 pagesCOMPLETE BLOOD COUNT Lecture GuideKaycee Gretz LorescaNo ratings yet