Download as pdf or txt
You might also like
- Pavement Design: Highway EngineeringDocument37 pagesPavement Design: Highway Engineeringjeromefamadico100% (2)
- Venture Bros: Innocence Cast AsideDocument73 pagesVenture Bros: Innocence Cast AsideZeb EcklesNo ratings yet
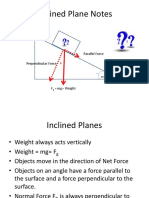
- Inclined Planes and Forces Notes PDFDocument19 pagesInclined Planes and Forces Notes PDFJohnLesterLaurelNo ratings yet
- Hepatitis B Virus (HBV) : A Review On Its Prevalence and Infection in Different Areas of IraqDocument8 pagesHepatitis B Virus (HBV) : A Review On Its Prevalence and Infection in Different Areas of IraqKanhiya MahourNo ratings yet
- Tentang World Hepatitis Day 2020Document8 pagesTentang World Hepatitis Day 2020YanMardianNo ratings yet
- Journal of Advanced Research: Nathalie Mentha, Sophie Clément, Francesco Negro, Dulce AlfaiateDocument13 pagesJournal of Advanced Research: Nathalie Mentha, Sophie Clément, Francesco Negro, Dulce AlfaiateYuin KhorNo ratings yet
- Hepatitis Delta Infection - Current and New Treatment OptionsDocument7 pagesHepatitis Delta Infection - Current and New Treatment OptionsDiana Carolina di Filippo VillaNo ratings yet
- Viral Hepatitis - Pragmatic Approach To Its Challenge in IndiaDocument3 pagesViral Hepatitis - Pragmatic Approach To Its Challenge in IndiabagusNo ratings yet
- Jiaa 668Document9 pagesJiaa 668prizankenny10No ratings yet
- Hepatite EDocument22 pagesHepatite EYmirNo ratings yet
- Jiaa668 PDFDocument9 pagesJiaa668 PDFhelen acostaNo ratings yet
- Diagnosis of Viral Hepatitis: ReviewDocument13 pagesDiagnosis of Viral Hepatitis: ReviewReza Redha AnandaNo ratings yet
- Prevalence of Hepatitis B Virus Infection Serologic Markers Among Blood Donors at Federal Medical Center, Keffi, Nasarawa State, NigeriaDocument17 pagesPrevalence of Hepatitis B Virus Infection Serologic Markers Among Blood Donors at Federal Medical Center, Keffi, Nasarawa State, NigeriaIJMSRTNo ratings yet
- Immigration and Viral Hepatitis: Public HealthDocument8 pagesImmigration and Viral Hepatitis: Public HealthEdgar MejiaNo ratings yet
- True Prevalence of Twin HDV-HBV Infection in Pakistan: A Molecular ApproachDocument5 pagesTrue Prevalence of Twin HDV-HBV Infection in Pakistan: A Molecular Approachwaqarkhan96No ratings yet
- Hcca Rev Nri 2005Document15 pagesHcca Rev Nri 2005Patrick RamosNo ratings yet
- Vassilopoulos 2002Document13 pagesVassilopoulos 2002deliaNo ratings yet
- Hepatitis Profile Co-Infection and Syphilis: Narrative Review ArticleDocument9 pagesHepatitis Profile Co-Infection and Syphilis: Narrative Review ArticleiajpsNo ratings yet
- Chronic Viral Hepatitis BDocument24 pagesChronic Viral Hepatitis BАлина ЛентицкийNo ratings yet
- Nihms 839861Document40 pagesNihms 839861Faisal JamshedNo ratings yet
- Prevalence of Overt and Occult Hepatitis B Virus Infections Among 135Document8 pagesPrevalence of Overt and Occult Hepatitis B Virus Infections Among 135د. مسلم الدخيليNo ratings yet
- Immigration and Viral Hepatitis: Public HealthDocument8 pagesImmigration and Viral Hepatitis: Public HealthFenny Noor AidaNo ratings yet
- EASL 2017 Clinical Practice Guidelines On The Management of Hepatitis B Virus InfectionDocument23 pagesEASL 2017 Clinical Practice Guidelines On The Management of Hepatitis B Virus InfectionIván Castellares RojasNo ratings yet
- Hepatitis C Virus: Screening, Diagnosis, and Interpretation of Laboratory AssaysDocument8 pagesHepatitis C Virus: Screening, Diagnosis, and Interpretation of Laboratory AssaysCristafeNo ratings yet
- Hepatitis B VaccinesDocument9 pagesHepatitis B Vaccinesadmir4No ratings yet
- HHS Public Access: Hepatitis B Virus Molecular Biology and PathogenesisDocument48 pagesHHS Public Access: Hepatitis B Virus Molecular Biology and PathogenesisZmajNo ratings yet
- Hepatitis D - OGRDocument7 pagesHepatitis D - OGRGrecia JimenezNo ratings yet
- Hepatitis Band Hepatitis Cviralinfection AReviewDocument13 pagesHepatitis Band Hepatitis Cviralinfection AReviewAustin HoodNo ratings yet
- Background: Cirrhosis Hepatocellular Carcinoma (HCC)Document24 pagesBackground: Cirrhosis Hepatocellular Carcinoma (HCC)Ignatius Rheza SetiawanNo ratings yet
- D Sousa 2020 Molecular Mechanisms of Viral Hepatitis Induced Hepatocellular CarcinomaDocument26 pagesD Sousa 2020 Molecular Mechanisms of Viral Hepatitis Induced Hepatocellular CarcinomaLUIS �NGEL V�LEZ SARMIENTONo ratings yet
- Acute Viral HepatitisDocument66 pagesAcute Viral HepatitisIfabiyi OlaniyiNo ratings yet
- Immunology of Hepatitis B Virus and Hepatitis C Virus InfectionDocument15 pagesImmunology of Hepatitis B Virus and Hepatitis C Virus InfectionMark BowlerNo ratings yet
- Pathogenesis of Hepatitis B Virus Infection: ReviewDocument11 pagesPathogenesis of Hepatitis B Virus Infection: ReviewShafa ShaviraNo ratings yet
- INTRODUCTION Final 5 (2) Sub 3Document25 pagesINTRODUCTION Final 5 (2) Sub 3Dawit g/kidanNo ratings yet
- Immunology of Hepatitis B Virus and Hepatitis C Virus InfectionDocument16 pagesImmunology of Hepatitis B Virus and Hepatitis C Virus InfectionZineb RAISNo ratings yet
- Seminar: Daniel P Webster, Paul Klenerman, Geoff Rey M DusheikoDocument12 pagesSeminar: Daniel P Webster, Paul Klenerman, Geoff Rey M Dusheikovira khairunisaNo ratings yet
- J Ejogrb 2020 11 052Document10 pagesJ Ejogrb 2020 11 052taki takiwNo ratings yet
- Hepatitis E Virus Songtanin 2023Document22 pagesHepatitis E Virus Songtanin 2023rootscriptureNo ratings yet
- Guidelines HepatitisDocument9 pagesGuidelines HepatitisSatriaNo ratings yet
- Hepatitis B Virus: Virology, Molecular Biology, Life Cycle and Intrahepatic SpreadDocument9 pagesHepatitis B Virus: Virology, Molecular Biology, Life Cycle and Intrahepatic SpreadMarius StancuNo ratings yet
- Viruses 13 01561 v3Document16 pagesViruses 13 01561 v3alphafoldjesus710No ratings yet
- Prevalence and Risk Factors Associated With Chronic Hepatitis B Among Patients Attending Fort Portal Regional Referral Hospital in Kabarole District, Western UgandaDocument13 pagesPrevalence and Risk Factors Associated With Chronic Hepatitis B Among Patients Attending Fort Portal Regional Referral Hospital in Kabarole District, Western UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Hepatitis Viruses (Other Than Hepatitis B and C Viruses) As Causes of Hepatocellular CarcinomaDocument13 pagesHepatitis Viruses (Other Than Hepatitis B and C Viruses) As Causes of Hepatocellular CarcinomaIvan RumenganNo ratings yet
- Hepatology - 2007 - Hoofnagle - Management of Hepatitis B Summary of A Clinical Research WorkshopDocument20 pagesHepatology - 2007 - Hoofnagle - Management of Hepatitis B Summary of A Clinical Research WorkshopEngr Hafiz Qasim AliNo ratings yet
- Pathogenic Mechanisms in HBV-and HCV-associated Hepatocellular CarcinomaDocument13 pagesPathogenic Mechanisms in HBV-and HCV-associated Hepatocellular CarcinomaJosé MateusNo ratings yet
- Fimmu 13 1059133Document29 pagesFimmu 13 1059133YANISSETH RIOS NINONo ratings yet
- Hepatology - 2014 - Messina - Global Distribution and Prevalence of Hepatitis C Virus GenotypesDocument11 pagesHepatology - 2014 - Messina - Global Distribution and Prevalence of Hepatitis C Virus GenotypesDem tksNo ratings yet
- Hep BDocument5 pagesHep BPolichonNo ratings yet
- Hepatitis B Envelope AntigenDocument30 pagesHepatitis B Envelope AntigenBalogun Samuel AbiodunNo ratings yet
- HepatitisBandHepatitisCviralinfectionAReview PDFDocument13 pagesHepatitisBandHepatitisCviralinfectionAReview PDFIndra YaniNo ratings yet
- Research Paper On Hepatitis BDocument20 pagesResearch Paper On Hepatitis Bjamaica_maglinteNo ratings yet
- Immunology of Hepatitis B Virus and Hepatitis C Virus InfectionDocument15 pagesImmunology of Hepatitis B Virus and Hepatitis C Virus InfectionHernan Dario Lancheros SanchezNo ratings yet
- Ijmsv02p0050 PDFDocument8 pagesIjmsv02p0050 PDFfikaanugrahNo ratings yet
- Chronic Viral Hepatitis:: Always Be Current!Document14 pagesChronic Viral Hepatitis:: Always Be Current!silpayNo ratings yet
- Hepatitis B: Pathophysiology and TransmissionDocument6 pagesHepatitis B: Pathophysiology and TransmissionEndrianus Jaya PutraNo ratings yet
- HepatitisDocument11 pagesHepatitistorsedepointeNo ratings yet
- Hepatitis Delta Genotype 5 Is Associated With Favourable Disease Outcome and Better Response To Treatment Compared To Genotype 1Document3 pagesHepatitis Delta Genotype 5 Is Associated With Favourable Disease Outcome and Better Response To Treatment Compared To Genotype 1muammerosmankoksalNo ratings yet
- Hepatitis E Springer Nature 2020 1Document11 pagesHepatitis E Springer Nature 2020 1azael11071991No ratings yet
- Hepatitis D: The Parasite's ParasiteDocument5 pagesHepatitis D: The Parasite's ParasiteLuis Ferdinand Dacera-Gabronino Gamponia-NonanNo ratings yet
- Hbsag HbcagDocument2 pagesHbsag HbcagRysna AzizahNo ratings yet
- Seroprevalence and Diagnosis of HIV, HBV, HCV and Syphilis Infections Among Blood DonorsDocument17 pagesSeroprevalence and Diagnosis of HIV, HBV, HCV and Syphilis Infections Among Blood DonorsNirmaljot KaurNo ratings yet
- Abbas 2014Document6 pagesAbbas 2014Apotik ApotekNo ratings yet
- Hepatitis B Virus and Liver DiseaseFrom EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNo ratings yet
- Bonaccia - Pizza La Cuptor Cu Lemne - Delivery Pizza Constanta 2Document1 pageBonaccia - Pizza La Cuptor Cu Lemne - Delivery Pizza Constanta 2Marilena TarcaNo ratings yet
- Biib059 - 2019Document1 pageBiib059 - 2019Marilena TarcaNo ratings yet
- Belimumab - 2021Document2 pagesBelimumab - 2021Marilena TarcaNo ratings yet
- Elimination of Hepatitis by 2030 Present.2Document6 pagesElimination of Hepatitis by 2030 Present.2Marilena TarcaNo ratings yet
- Lupus Art. 18Document2 pagesLupus Art. 18Marilena TarcaNo ratings yet
- Lupus Art. 19Document16 pagesLupus Art. 19Marilena TarcaNo ratings yet
- Lupus Art. 22Document19 pagesLupus Art. 22Marilena TarcaNo ratings yet
- Bibliografie Biochimie CrisDocument1 pageBibliografie Biochimie CrisMarilena TarcaNo ratings yet
- Lupus Art. 20Document13 pagesLupus Art. 20Marilena TarcaNo ratings yet
- Buletine de Analize: Dr. Nicoleta LefterDocument37 pagesBuletine de Analize: Dr. Nicoleta LefterMarilena TarcaNo ratings yet
- AINS CaseDocument11 pagesAINS CaseMarilena TarcaNo ratings yet
- Incidenta-25 09-08 10 2020Document2 pagesIncidenta-25 09-08 10 2020Marilena TarcaNo ratings yet
- Maths PDFDocument148 pagesMaths PDFAnkit BamboriyaNo ratings yet
- (The Solar System) Sherman Hollar-Astronomy - Understanding The Universe - Rosen Education Service (2011)Document98 pages(The Solar System) Sherman Hollar-Astronomy - Understanding The Universe - Rosen Education Service (2011)Camila Cavalcante100% (2)
- Face Sketch Synthesis Via Sparse Representation-Based Greedy SearchDocument6 pagesFace Sketch Synthesis Via Sparse Representation-Based Greedy SearchshaliniNo ratings yet
- Basic Electrical Circuits DR Nagendra Krishnapura Department of Electrical Engineering Indian Institute of Technology Madras Lecture - 01Document2 pagesBasic Electrical Circuits DR Nagendra Krishnapura Department of Electrical Engineering Indian Institute of Technology Madras Lecture - 01Ranjeet Singh BishtNo ratings yet
- Unfe 65 Intersex Factsheet ENGLISHDocument2 pagesUnfe 65 Intersex Factsheet ENGLISHRinio SimeonidouNo ratings yet
- Mayo Medical School: College of MedicineDocument28 pagesMayo Medical School: College of MedicineDragomir IsabellaNo ratings yet
- EbpDocument44 pagesEbpapi-356127291No ratings yet
- Course Code: 5653-01 Programme: M.L.I.S: Assignment No. 1Document14 pagesCourse Code: 5653-01 Programme: M.L.I.S: Assignment No. 1Qazi zubairNo ratings yet
- Test Bank For Learning Principles and Applications 8th Edition Stephen B KleinDocument21 pagesTest Bank For Learning Principles and Applications 8th Edition Stephen B KleinTonyRamosriqzf100% (36)
- A Critical Analysis of The Writings of Amos RapoportDocument11 pagesA Critical Analysis of The Writings of Amos RapoportmaxwalkerdreamNo ratings yet
- Arnold R. Shore, John M. (Michael) Carfora - The Art of Funding and Implementing Ideas - A Guide To Proposal Development and Project Management-SAGE Publications, Inc (2010) PDFDocument113 pagesArnold R. Shore, John M. (Michael) Carfora - The Art of Funding and Implementing Ideas - A Guide To Proposal Development and Project Management-SAGE Publications, Inc (2010) PDFRichard Oduor OdukuNo ratings yet
- Galatians GreekDocument5 pagesGalatians GreekTeresaVrazelKiehlNo ratings yet
- AN Assignment On Nursing Audit SUBJECT: Nursing ManagementDocument6 pagesAN Assignment On Nursing Audit SUBJECT: Nursing ManagementMansi Dabola100% (1)
- PPR MA Education SplittedDocument45 pagesPPR MA Education SplittedArif MohammadNo ratings yet
- Flight1 441 Conquest TutorialDocument10 pagesFlight1 441 Conquest TutorialJosé A. Montiel QuirósNo ratings yet
- Relevance Lost - MEDocument11 pagesRelevance Lost - MESiti FatimahNo ratings yet
- PendereckiDocument23 pagesPendereckiRuud WeltenNo ratings yet
- Info - Iec60079 29 2 (Ed2.0) en PDFDocument14 pagesInfo - Iec60079 29 2 (Ed2.0) en PDFtaibi aliNo ratings yet
- HindustaniMelodic SQPDocument4 pagesHindustaniMelodic SQPAkshit ChauhanNo ratings yet
- Kamal Sadiq CH 7Document11 pagesKamal Sadiq CH 7Gianna MinochaNo ratings yet
- Advanced 1 Midterm Written BDocument6 pagesAdvanced 1 Midterm Written BCarolina Aguido FerreiraNo ratings yet
- The ABCs of DR Desmond Ford S Theology W H JohnsDocument16 pagesThe ABCs of DR Desmond Ford S Theology W H JohnsBogdan PlaticaNo ratings yet
- Coop Learning ActivitiesDocument198 pagesCoop Learning ActivitiesJanine Mosca GonzalesNo ratings yet
- Finer - 2015 - Russian ModernismDocument18 pagesFiner - 2015 - Russian ModernismJosué Durán HNo ratings yet
- PA 644 - M2 LecturesDocument412 pagesPA 644 - M2 LectureskatNo ratings yet
- Extended Essay IB DiplomaDocument20 pagesExtended Essay IB Diplomasol GonzalezNo ratings yet
- Sami Pihlström - Putnam's Conception of Ontology (2006)Document13 pagesSami Pihlström - Putnam's Conception of Ontology (2006)lazarNo ratings yet