Download as pdf or txt
You might also like
- NCP. Decreased Cardiac OutputDocument5 pagesNCP. Decreased Cardiac OutputJillian AmponinNo ratings yet
- What Is HomeoprophylaxisDocument6 pagesWhat Is HomeoprophylaxiswrestlerloverNo ratings yet
- ESCAPE Study - JAMA 2005Document9 pagesESCAPE Study - JAMA 2005MICHAEL AMARILLO CORREANo ratings yet
- WATERFALL trial editorial - Fluid Resuscitation in Acute Pancreatitis - Going over the WATERFALL - 36103418Document2 pagesWATERFALL trial editorial - Fluid Resuscitation in Acute Pancreatitis - Going over the WATERFALL - 36103418hyperian521No ratings yet
- Febuxostat Therapy For Patients With Stage 3 CKD and Asymptomatic Hyperuricemia: A Randomized TrialDocument13 pagesFebuxostat Therapy For Patients With Stage 3 CKD and Asymptomatic Hyperuricemia: A Randomized TrialAndreas AdiwinataNo ratings yet
- Stop-Acei Trial Journal ClubDocument3 pagesStop-Acei Trial Journal Clubapi-648891519No ratings yet
- RCT ArticleDocument8 pagesRCT ArticleelpisNo ratings yet
- Kidney News Article p20 7Document2 pagesKidney News Article p20 7ilgarciaNo ratings yet
- Jeffrey L Carson Restrictive or Liberal TransfusionDocument11 pagesJeffrey L Carson Restrictive or Liberal Transfusionmiguel aghelNo ratings yet
- Cardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesDocument12 pagesCardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesAntonella Angulo CruzadoNo ratings yet
- Patel Et Al 2021 Kidney Function and Outcomes in Patients Hospitalized With Heart FailureDocument14 pagesPatel Et Al 2021 Kidney Function and Outcomes in Patients Hospitalized With Heart Failurevlopes.ptNo ratings yet
- 2014 Halt AdpkdDocument12 pages2014 Halt AdpkdBogdan Marian SorohanNo ratings yet
- Statin in CKDDocument10 pagesStatin in CKDKartika RahmawatiNo ratings yet
- Carson 2011Document10 pagesCarson 2011karine.ghiggiNo ratings yet
- Empagliflozin in Heart Failure With A Preserved Ejection FractionDocument11 pagesEmpagliflozin in Heart Failure With A Preserved Ejection FractionVinh Quy VoNo ratings yet
- Empagliflozin in Heart Failure With A PreservedDocument11 pagesEmpagliflozin in Heart Failure With A PreservedmarlenjyNo ratings yet
- DM Nefro3Document10 pagesDM Nefro3Teddy Alexander MorinNo ratings yet
- 3908 FullDocument7 pages3908 FullJavier MedinaNo ratings yet
- Cardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesDocument12 pagesCardiovascular and Renal Outcomes With Efpeglenatide in Type 2 DiabetesMoeez AkramNo ratings yet
- Journal Pone 0189126Document13 pagesJournal Pone 0189126Mohamad Syaikhul IslamNo ratings yet
- Astronaut 2013Document11 pagesAstronaut 2013Guilherme CarelliNo ratings yet
- Evidence-Based Medical Treatment of Peripheral Arterial Disease: A Rapid ReviewDocument14 pagesEvidence-Based Medical Treatment of Peripheral Arterial Disease: A Rapid ReviewLeo OoNo ratings yet
- Nejmoa 2107038Document11 pagesNejmoa 2107038Luis Rafael Suárez U.No ratings yet
- Empagliflozin in Heart Failure With A Preserved Ejection FractionDocument11 pagesEmpagliflozin in Heart Failure With A Preserved Ejection Fractionsri wahyuniNo ratings yet
- Alirocumab and Cardiovascular Outcomes After Acute Coronary SyndromeDocument11 pagesAlirocumab and Cardiovascular Outcomes After Acute Coronary SyndromeJohanyta Cañaveral QFNo ratings yet
- Brar 2014Document10 pagesBrar 2014Ismael Rivera DiazNo ratings yet
- Lixisenatide in Patients With Type 2 Diabetes and Acute Coronary SyndromeDocument11 pagesLixisenatide in Patients With Type 2 Diabetes and Acute Coronary SyndromeAndi Soraya PurnamandaNo ratings yet
- AURORA: Is There A Role For Statin Therapy in Dialysis Patients?Document4 pagesAURORA: Is There A Role For Statin Therapy in Dialysis Patients?Ravan WidiNo ratings yet
- Anemia Treatment in Patients With Chronic Kidney Disease: EditorialsDocument3 pagesAnemia Treatment in Patients With Chronic Kidney Disease: EditorialsGalih AryyagunawanNo ratings yet
- Reducción de Uratos y ERC NEJM 2020Document2 pagesReducción de Uratos y ERC NEJM 2020Gabriel VargasNo ratings yet
- PEXIVAS The End of Plasmapheresis For ANCA-Associated Vasculitis - CJASN 2020Document3 pagesPEXIVAS The End of Plasmapheresis For ANCA-Associated Vasculitis - CJASN 2020drshhagarNo ratings yet
- Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization EffectivenessDocument9 pagesEvaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization EffectivenessMelisa AnaNo ratings yet
- Mechanisms, Clinical Implications, and Treatment of Intradialytic HypotensionDocument7 pagesMechanisms, Clinical Implications, and Treatment of Intradialytic Hypotensionhemer hadyn calderon alvitesNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofAlvin JulianNo ratings yet
- Pfeffer 2009Document14 pagesPfeffer 2009maimetungka5764No ratings yet
- Long-Term Follow-Up After Tight Control of Blood Pressure in Type 2 DiabetesDocument12 pagesLong-Term Follow-Up After Tight Control of Blood Pressure in Type 2 DiabetesnovywardanaNo ratings yet
- Hypertension Control in African-American Patients With Chronic Kidney DiseaseDocument3 pagesHypertension Control in African-American Patients With Chronic Kidney Diseaseandikaagus13No ratings yet
- Pi Is 0272638616302645Document9 pagesPi Is 0272638616302645Eko PrasNo ratings yet
- Cardiovascular and Renal Outcomes With Empagliflozin in Heart FailureDocument12 pagesCardiovascular and Renal Outcomes With Empagliflozin in Heart FailureSandra PargaNo ratings yet
- PCI or CABG, That Is The Question!: Jong Shin Woo, MD, and Weon Kim, MDDocument2 pagesPCI or CABG, That Is The Question!: Jong Shin Woo, MD, and Weon Kim, MDHeńřÿ ŁøĵæńNo ratings yet
- Pi Is 1933287417302908Document11 pagesPi Is 1933287417302908Anonymous yptjlwJNo ratings yet
- Estudio CheetaDocument11 pagesEstudio CheetacrisordNo ratings yet
- Revive IiDocument9 pagesRevive Iidalialamasbonita1093No ratings yet
- Intradialitic HypotensionDocument7 pagesIntradialitic HypotensionanitaNo ratings yet
- CME Article: Clinical Trials and ObservationsDocument9 pagesCME Article: Clinical Trials and ObservationsOrxan HumbetovNo ratings yet
- CourageDocument14 pagesCourageSuryaNo ratings yet
- Comparative Efficacy of Angiotensin Converting Enzymes Inhibitors and Angiotensin Receptor Blockers in Patients With Heart Failure in Tanzania A Prospective Cohort StudyDocument10 pagesComparative Efficacy of Angiotensin Converting Enzymes Inhibitors and Angiotensin Receptor Blockers in Patients With Heart Failure in Tanzania A Prospective Cohort StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal Tatalaksana 2Document7 pagesJurnal Tatalaksana 2winny kartikaNo ratings yet
- Empagliflozin Outcome Trial in Patients With Chronic Heart Failure and A Reduced Ejection Fraction - American College of CardiologyDocument5 pagesEmpagliflozin Outcome Trial in Patients With Chronic Heart Failure and A Reduced Ejection Fraction - American College of CardiologyJackeline PazNo ratings yet
- Etm 07 03 0604Document5 pagesEtm 07 03 0604Raissa Metasari TantoNo ratings yet
- 2011 - Denicola (Jurnal)Document9 pages2011 - Denicola (Jurnal)Riana HandayaniNo ratings yet
- Hyperkalemia and Renin-Angiotensin Aldosterone System Inhibitor Therapy in Chronic Kidney Disease: A General Practice-Based, Observational StudyDocument15 pagesHyperkalemia and Renin-Angiotensin Aldosterone System Inhibitor Therapy in Chronic Kidney Disease: A General Practice-Based, Observational StudyRobertoVeraNo ratings yet
- Flow Nejm AksDocument13 pagesFlow Nejm Akslakshminivas PingaliNo ratings yet
- 2832 FullDocument6 pages2832 FullAdwin AlamsyaputraNo ratings yet
- New England Journal Medicine: The ofDocument14 pagesNew England Journal Medicine: The ofIMNo ratings yet
- Dapagliflozin and Cardiovascular Outcomes in Type 2 DiabetesDocument12 pagesDapagliflozin and Cardiovascular Outcomes in Type 2 DiabetesAlina PopaNo ratings yet
- RCT EvinacumabDocument13 pagesRCT EvinacumabMamoNo ratings yet
- Revascularizar ICC No Mejora PronosticoDocument10 pagesRevascularizar ICC No Mejora Pronosticokaren mendoza rodriguezNo ratings yet
- Manejo IncidentalomasDocument3 pagesManejo IncidentalomasAlexandra FreireNo ratings yet
- Geetha D, Specks U, Stone JH, Et Al. Rituximab Versus CyclophosphamideDocument14 pagesGeetha D, Specks U, Stone JH, Et Al. Rituximab Versus CyclophosphamidePablo BarraganNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofAlina PirtacNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Cancer PDFDocument18 pagesCancer PDFAhmed goldenNo ratings yet
- 1628 6995 3 PBDocument32 pages1628 6995 3 PBPelayanan Tahanan Rutan KendariNo ratings yet
- Chapter 20 With Comments - Acinetobacter - StenotrophomonasDocument13 pagesChapter 20 With Comments - Acinetobacter - StenotrophomonasGordon JamesonNo ratings yet
- Thyroid SwellingDocument8 pagesThyroid SwellingDn Ezrinah Dn Esham50% (2)
- Hair, Face, Nose, Neck, Skin, and NailsDocument4 pagesHair, Face, Nose, Neck, Skin, and NailsZJ GarcianoNo ratings yet
- 0 - Case Presentation On Uti, CKDDocument20 pages0 - Case Presentation On Uti, CKDAbin PNo ratings yet
- Epidemiology of Oral CancerDocument12 pagesEpidemiology of Oral Cancerعدي عبدالالهNo ratings yet
- Special Education ClassificationsDocument3 pagesSpecial Education ClassificationsEdmar AgarpaoNo ratings yet
- DRUG CeftazidimeDocument1 pageDRUG Ceftazidimerholiboi0% (1)
- Basic Principles of Wound MGMT - Poengki DP-ilovepdf-compressedDocument38 pagesBasic Principles of Wound MGMT - Poengki DP-ilovepdf-compressednugrahaNo ratings yet
- PyelonephritisDocument24 pagesPyelonephritisfatihahannisahumairaNo ratings yet
- Pre-Icar-Self Assessment Test - 2021: by DR Hanuman Mvsc-Scholar-Vsr - GadvasuDocument121 pagesPre-Icar-Self Assessment Test - 2021: by DR Hanuman Mvsc-Scholar-Vsr - Gadvasusuresh nepaliNo ratings yet
- Nexus ConnectionsDocument2 pagesNexus ConnectionsBarry RoginskiNo ratings yet
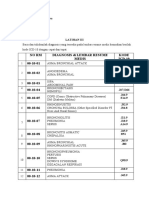
- L P APHDocument11 pagesL P APHmoni khatkarNo ratings yet
- Betarie Anum Almira - RMIK (A) - Praktik KSPK 8Document9 pagesBetarie Anum Almira - RMIK (A) - Praktik KSPK 8Betarie Anum AlmiraNo ratings yet
- Module1 Overview HivinfectionDocument20 pagesModule1 Overview HivinfectionCristine BarrozaNo ratings yet
- Hematology Terms and DefinitionsDocument9 pagesHematology Terms and DefinitionsLovely B. AlipatNo ratings yet
- Afectiuni GastriceDocument7 pagesAfectiuni GastriceAndreea ElenaNo ratings yet
- Acute Bioligic CrisisDocument141 pagesAcute Bioligic CrisisJanelle MatamorosaNo ratings yet
- Post Test NUR 219 17Document3 pagesPost Test NUR 219 17Naomi VirtudazoNo ratings yet
- Unit 4 - Mental Health and Coping - Dealing With Anxiety and DepressionDocument49 pagesUnit 4 - Mental Health and Coping - Dealing With Anxiety and DepressionAundrei ValdezNo ratings yet
- Telemetry Recognition WorkbookDocument29 pagesTelemetry Recognition WorkbookQueenNo ratings yet
- Pneumonia Is A Serious Infection of The Lungs in Which The AirDocument1 pagePneumonia Is A Serious Infection of The Lungs in Which The AirErdem EzerNo ratings yet
- Male InfertilityDocument1 pageMale Infertilitya jNo ratings yet
- Silent SyndromeDocument1 pageSilent SyndromeDFSAFSAFLFKSLNo ratings yet
- Aesculus Is Especially Indicated For People With Low Back Pain Who Also Have A TendencyDocument2 pagesAesculus Is Especially Indicated For People With Low Back Pain Who Also Have A Tendencyradmilo32No ratings yet
- Drug Study-Sodium BicarbonateDocument7 pagesDrug Study-Sodium BicarbonateTrisha Faye OrtegaNo ratings yet
- Listening Drills - Melissa GordonDocument5 pagesListening Drills - Melissa GordonAira CatubayNo ratings yet