Download as pdf or txt
You might also like
- Ebook Strategic Management Competitiveness and Globalization Concepts and Cases 14E PDF Full Chapter PDFDocument67 pagesEbook Strategic Management Competitiveness and Globalization Concepts and Cases 14E PDF Full Chapter PDFsamuel.chapman41697% (38)
- Cambridge Secondary Checkpoint - Science (1113) PastPapers 2009-2019Document375 pagesCambridge Secondary Checkpoint - Science (1113) PastPapers 2009-2019Harini Bharani100% (8)
- John Carroll University Magazine Spring 2012Document54 pagesJohn Carroll University Magazine Spring 2012johncarrolluniversityNo ratings yet
- Review Article: Chagas' Disease: Pregnancy and Congenital TransmissionDocument11 pagesReview Article: Chagas' Disease: Pregnancy and Congenital Transmissiondiaa skamNo ratings yet
- Enfermedad de Chagas PDFDocument10 pagesEnfermedad de Chagas PDFLuisFernando91No ratings yet
- Enfermedad de Chagas Una Visión General de Los Aspectos Clínicos y Epidemiológicos Pereira 2013Document10 pagesEnfermedad de Chagas Una Visión General de Los Aspectos Clínicos y Epidemiológicos Pereira 2013Adriana Santander OliveraNo ratings yet
- Chapter 7Document34 pagesChapter 7Regina MunaamadaniNo ratings yet
- Oral Transmission of Chagas DiseaseDocument8 pagesOral Transmission of Chagas DiseaseLuisa MontoyaNo ratings yet
- Hepatology - 2004 - Alter - Epidemiology of Hepatitis CDocument4 pagesHepatology - 2004 - Alter - Epidemiology of Hepatitis CEngr Hafiz Qasim AliNo ratings yet
- 1 s2.0 S0140673623017877 MainDocument16 pages1 s2.0 S0140673623017877 Mainybahos3misenaNo ratings yet
- tmpF7DD TMPDocument6 pagestmpF7DD TMPFrontiersNo ratings yet
- Molecular Dissection of Chagas Induced CardiomyopathyDocument31 pagesMolecular Dissection of Chagas Induced CardiomyopathyClaudia Calvet AlvarezNo ratings yet
- Nihms 1895762Document25 pagesNihms 1895762medicinainterna.hgdz2023No ratings yet
- Dengue (Lancet)Document16 pagesDengue (Lancet)Roberth Mero100% (1)
- Bellini Biologic and Genetics Aspects of Chagas Disease at Endemic AreasDocument12 pagesBellini Biologic and Genetics Aspects of Chagas Disease at Endemic AreasGabriela Sanches SerranoNo ratings yet
- Enfermedad de ChagasDocument11 pagesEnfermedad de Chagasandrea3895No ratings yet
- Chagas Disease: SeminarDocument13 pagesChagas Disease: SeminarRafaelNo ratings yet
- CLN 71 08 455Document9 pagesCLN 71 08 455Ranny Yovita MaharaniNo ratings yet
- Emerging Infectious Disease Agents and Their Potential Threat To Transfusion Safety.Document29 pagesEmerging Infectious Disease Agents and Their Potential Threat To Transfusion Safety.Pritha BhuwapaksophonNo ratings yet
- Clinical and Epidemiological Aspects of Chagas DiseaseDocument9 pagesClinical and Epidemiological Aspects of Chagas Diseasenatalia muñoz rodriguezNo ratings yet
- 2019 Chagas Review PDFDocument32 pages2019 Chagas Review PDFW Antonio Rivera MartínezNo ratings yet
- Fatal Acute Chagas Disease by TrypanosomaDocument5 pagesFatal Acute Chagas Disease by TrypanosomaGabriela YandunNo ratings yet
- Vassilopoulos 2002Document13 pagesVassilopoulos 2002deliaNo ratings yet
- Journal LeticiaDocument12 pagesJournal LeticiaDewi KUNo ratings yet
- Infecã Ã o e Doenã A CV JACCDocument10 pagesInfecã Ã o e Doenã A CV JACCgpxwdfbqfdNo ratings yet
- Tambo, Adetunde and Olalubi 2018 PDFDocument7 pagesTambo, Adetunde and Olalubi 2018 PDFOluwasegun AdetundeNo ratings yet
- Al-Tawfiq, Tambyah - 2014 - Healthcare Associated Infections (HAI) PerspectivesDocument6 pagesAl-Tawfiq, Tambyah - 2014 - Healthcare Associated Infections (HAI) PerspectiveshanNo ratings yet
- Chagasic CardiomyopathyDocument27 pagesChagasic Cardiomyopathykj185No ratings yet
- Hepa Changes in ManagementDocument9 pagesHepa Changes in Managemente.foresgilNo ratings yet
- 1 s2.0 S0196439923000491 MainDocument9 pages1 s2.0 S0196439923000491 Mainybahos3misenaNo ratings yet
- Is Dengue A Threat To The Blood Supply?: D. Teo, L. C. NG & S. LamDocument12 pagesIs Dengue A Threat To The Blood Supply?: D. Teo, L. C. NG & S. LamCristhian ReyesNo ratings yet
- Neglected Tropical Diseases in Sub-Saharan Africa: Review of Their Prevalence, Distribution, and Disease BurdenDocument10 pagesNeglected Tropical Diseases in Sub-Saharan Africa: Review of Their Prevalence, Distribution, and Disease BurdenGuhan KANo ratings yet
- 1 s2.0 S2667100X23000567 MainDocument18 pages1 s2.0 S2667100X23000567 MainEnrique CastelanNo ratings yet
- DHF Review Focused in Pulmonary InvolvementDocument7 pagesDHF Review Focused in Pulmonary InvolvementAmirah FaridahNo ratings yet
- Bio StatslecturesDocument60 pagesBio StatslectureszeliawillscumbergNo ratings yet
- The Engines of SARS-CoV-2 SpreadDocument3 pagesThe Engines of SARS-CoV-2 Spreadsc8v86fbnbNo ratings yet
- Chapter E132 - Coronavirus Disease (COVID-19)Document31 pagesChapter E132 - Coronavirus Disease (COVID-19)aleksme88No ratings yet
- Ageing 2: The Burden of Disease in Older People and Implications For Health Policy and PracticeDocument15 pagesAgeing 2: The Burden of Disease in Older People and Implications For Health Policy and PracticeEdeline LooNo ratings yet
- Dengue LancetDocument16 pagesDengue LancetJorge Ricardo Uchuya GómezNo ratings yet
- Prevention of Inection Related Tumor Bgr054Document9 pagesPrevention of Inection Related Tumor Bgr054heruNo ratings yet
- 1 - Mathematical Formulation of Hepatitis B Virus With Optimal Control Analysis PDFDocument16 pages1 - Mathematical Formulation of Hepatitis B Virus With Optimal Control Analysis PDFindah rania729No ratings yet
- Immigration and Viral Hepatitis: Public HealthDocument8 pagesImmigration and Viral Hepatitis: Public HealthEdgar MejiaNo ratings yet
- Cruz 021Document12 pagesCruz 021wasimNo ratings yet
- Trujillo-Ochoa2018 Hav in MexicoDocument9 pagesTrujillo-Ochoa2018 Hav in MexicoOliver Viera SeguraNo ratings yet
- Global Numbers of Infection and Disease Burden of Soil Transmitted Helminth Infections in 2010Document19 pagesGlobal Numbers of Infection and Disease Burden of Soil Transmitted Helminth Infections in 2010Yuanita ClaraNo ratings yet
- Seminar: Keertan Dheda, Clifton E Barry 3rd, Gary MaartensDocument16 pagesSeminar: Keertan Dheda, Clifton E Barry 3rd, Gary Maartensmedicina FelipeNo ratings yet
- Mcglynn 2020Document23 pagesMcglynn 2020Luluil MunirohNo ratings yet
- Nature 2020 03 05Document467 pagesNature 2020 03 05Desmond pengNo ratings yet
- Viral Hepatitis in Pregnancy PDFDocument15 pagesViral Hepatitis in Pregnancy PDFBerri RahmadhoniNo ratings yet
- Risk of Leukemia After DengueDocument7 pagesRisk of Leukemia After DengueJoão Marcos Germano SouzaNo ratings yet
- White Paper - Effective-Covid19-Control-through-carrier-tracking-and-non-pharmaceutical-interventions-v2.0-2Document45 pagesWhite Paper - Effective-Covid19-Control-through-carrier-tracking-and-non-pharmaceutical-interventions-v2.0-2Daniel SloanNo ratings yet
- mr1018 1 ch5Document21 pagesmr1018 1 ch5AkileshDhanushiyanNo ratings yet
- 05 - Hepatitis B Virus Infection - Lancet 2014Document11 pages05 - Hepatitis B Virus Infection - Lancet 2014Jmv VegaNo ratings yet
- Guzman 2010Document3 pagesGuzman 2010Renaldi ArdiyaNo ratings yet
- Immigration and Viral Hepatitis: Public HealthDocument8 pagesImmigration and Viral Hepatitis: Public HealthFenny Noor AidaNo ratings yet
- Diagnosis and Management of COVID-19 Disease: Public HealthDocument4 pagesDiagnosis and Management of COVID-19 Disease: Public HealthSam HaileyNo ratings yet
- Cutting Edge Issues in Rheumatic FeverDocument25 pagesCutting Edge Issues in Rheumatic FeverGeorgi GugicevNo ratings yet
- University of Santo Tomas: UST-SHS Practical Research 2Document3 pagesUniversity of Santo Tomas: UST-SHS Practical Research 2MayNo ratings yet
- Plos One 2021Document20 pagesPlos One 2021cdsaludNo ratings yet
- Why We Should Take Coronavirus SeriouslyDocument6 pagesWhy We Should Take Coronavirus Seriouslytara100% (2)
- Dengue Hemorrhagic Fever and Shock Syndromes : Suchitra Ranjit, MBBS, MD Niranjan Kissoon, MBBS, FAAP, FCCM, FACPEDocument11 pagesDengue Hemorrhagic Fever and Shock Syndromes : Suchitra Ranjit, MBBS, MD Niranjan Kissoon, MBBS, FAAP, FCCM, FACPEvalenzuelacastilloNo ratings yet
- @MBS - MedicalBooksStore - 2020 - Global-993hlm (Warna Hanya Cover) - 1Document58 pages@MBS - MedicalBooksStore - 2020 - Global-993hlm (Warna Hanya Cover) - 1Gunawan AriefNo ratings yet
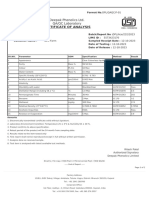
- Acetone - Deepak PhenolicsDocument1 pageAcetone - Deepak PhenolicsPraful YadavNo ratings yet
- Charles H. Hapgood Earths Shifting Crust 331 420Document90 pagesCharles H. Hapgood Earths Shifting Crust 331 420Cesar Ruiz100% (1)
- Cambridge IGCSE: Information and Communication Technology 0417/31Document8 pagesCambridge IGCSE: Information and Communication Technology 0417/31Erdoğan ŞahinNo ratings yet
- Gyroscopic PrinciplesDocument38 pagesGyroscopic PrinciplesAli Abu Shhiwa100% (1)
- Optimization of Methanol ProductionDocument14 pagesOptimization of Methanol ProductionMuhammad AliNo ratings yet
- IGF Code WorkbookDocument9 pagesIGF Code WorkbookGiby JohnNo ratings yet
- Crown WAV60 Operator Manual - CompressedDocument39 pagesCrown WAV60 Operator Manual - CompressedHector PeñaNo ratings yet
- HistoryDocument5 pagesHistoryrawan.sharari0911No ratings yet
- MGT410 Take Home Final 1 - Fall2010Document10 pagesMGT410 Take Home Final 1 - Fall2010Belinda Elois ToNo ratings yet
- Valkokari TIMReview August2015Document8 pagesValkokari TIMReview August2015Héctor BallesterosNo ratings yet
- Leading Workplace CommunicationDocument26 pagesLeading Workplace CommunicationEahbm KaduNo ratings yet
- MODULE 4 - Sliding Contact BearingDocument14 pagesMODULE 4 - Sliding Contact BearingBoris PalaoNo ratings yet
- Troy-Bilt 019191 PDFDocument34 pagesTroy-Bilt 019191 PDFSteven W. NinichuckNo ratings yet
- Technical Guidelines: Physical Properties of Refrigerants R-410ADocument2 pagesTechnical Guidelines: Physical Properties of Refrigerants R-410AYaxmine Edward StylesNo ratings yet
- Mini Proj RCT 222 PDFDocument34 pagesMini Proj RCT 222 PDF4073 kolakaluru mounishaNo ratings yet
- American Scientific Research Journal For Engineering, Technology, and Sciences (Asrjets), Vol 6, No 1 (2013), Issn (Print) 2313-44106Document2 pagesAmerican Scientific Research Journal For Engineering, Technology, and Sciences (Asrjets), Vol 6, No 1 (2013), Issn (Print) 2313-44106atilaelciNo ratings yet
- Limbo PowerpointDocument10 pagesLimbo Powerpointapi-693306390No ratings yet
- Feeling Comfortable With Logic Analyzers PDFDocument24 pagesFeeling Comfortable With Logic Analyzers PDFJ dosherNo ratings yet
- BRS ExerciseDocument7 pagesBRS ExerciseMuskan LohariwalNo ratings yet
- Sensor de TierraDocument3 pagesSensor de TierraAnonymous FXM2q3hM2No ratings yet
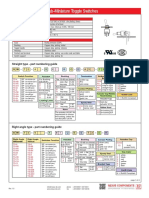
- SW-TS40T Series Sub-Miniature Toggle Switches: Straight Type - Part Numbering GuideDocument4 pagesSW-TS40T Series Sub-Miniature Toggle Switches: Straight Type - Part Numbering GuideVALTERNo ratings yet
- Advance Data StructuresDocument184 pagesAdvance Data StructureskamsiNo ratings yet
- Passage 2 For Grade 6Document3 pagesPassage 2 For Grade 6Irish Joy CachaperoNo ratings yet
- IELTS Essay 1 With AnswerDocument1 pageIELTS Essay 1 With AnsweraazizmajidNo ratings yet
- AI-Ghazali On Logical Necessity, Causality, and MiraclesDocument16 pagesAI-Ghazali On Logical Necessity, Causality, and Miraclespll01No ratings yet
- Grade 9 Social Studies Textbook CbseDocument3 pagesGrade 9 Social Studies Textbook CbseKurtNo ratings yet
- FCE Exam 3 ListeningDocument6 pagesFCE Exam 3 ListeningSaul MendozaNo ratings yet