Physician / Office Name DOCTOR / PHYSICIAN
Address Line 1
Address Line 2
City, State, ZIP
1(123) 456-7899
website@company.com
your@email.com
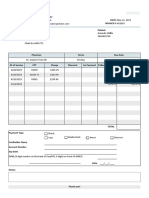
INVOICE
Bill To Invoice # Payment Terms Amount Due
Patient Name _e.g., 00000 _e.g., Net 14
$ 321.00
_Address Line 1
Invoice Date Due Date
_Address Line 2
01/01/2025 01/14/2025
_City, State, ZIP
Description Qty / Hrs Price / Rate Amount
_Post-surgery check-up 1 $ 250.00 $ 250.00
_Arm sling 1 $ 50.00 $ 50.00
$ 0.00
$ 0.00
$ 0.00
$ 0.00
Payment Method(s): _e.g., Check, credit card, or online Subtotal $ 300.00
Tax $ 21.00
Payment Link(s): _e.g., https://healthpaymentonline.com/ Misc.
Notes: Recovering is going well! We look forward to seeing u back in 6 weeks. Amount Due $ 321.00
yo
Brought to you by InTouch Health!
You might also like
- Dicks ReceiptDocument3 pagesDicks Receiptmiranda criggerNo ratings yet
- Eye Doctor Bill ExampleDocument1 pageEye Doctor Bill Examplemiranda criggerNo ratings yet
- Dave Banking Account StatementDocument2 pagesDave Banking Account Statementdaniel floydNo ratings yet
- Doctor ReceiptDocument1 pageDoctor Receiptmiranda criggerNo ratings yet
- Methadone Invoice Paid ExampleDocument1 pageMethadone Invoice Paid Examplemiranda criggerNo ratings yet
- Var o DocumentDocument2 pagesVar o DocumentNatalie RichardsonNo ratings yet
- March 2020 Varo Bank StatementDocument2 pagesMarch 2020 Varo Bank StatementCandy ValentineNo ratings yet
- Account Number Statement Period: ActivityDocument2 pagesAccount Number Statement Period: ActivityAshley KingNo ratings yet
- March 06 2017Document10 pagesMarch 06 2017Anonymous u7HLgyXDTNo ratings yet
- Confirmation Your Receipt: Payment Was Successful - Your Money Has Been SentDocument2 pagesConfirmation Your Receipt: Payment Was Successful - Your Money Has Been SentAhmed KassemNo ratings yet
- Handyman InvoiceDocument1 pageHandyman InvoiceAlimNo ratings yet
- Ambulance InvoiceDocument1 pageAmbulance InvoicetrandreelsNo ratings yet
- Quotation TemplateDocument1 pageQuotation TemplateIsmail ZakariaNo ratings yet
- Yoga InvoiceDocument1 pageYoga InvoiceedcaabayNo ratings yet
- Invoice Template PDF 3Document1 pageInvoice Template PDF 3Ashraf Al-SayedNo ratings yet
- Invoice: ID Description Qty Price TotalDocument1 pageInvoice: ID Description Qty Price TotalSanjeev ThadaniNo ratings yet
- Travel Invoice TemplateDocument1 pageTravel Invoice TemplateGaneshNo ratings yet
- Your Company Name: InvoiceDocument2 pagesYour Company Name: InvoicelarisaNo ratings yet
- Invoice Template Excel22Document4 pagesInvoice Template Excel22aliouecheNo ratings yet
- Shari A WallaceDocument2 pagesShari A WallaceMark WilliamsNo ratings yet
- Images Receipt Template Excel22Document4 pagesImages Receipt Template Excel22uduhpatrick2002No ratings yet
- Cell Phone Repair InvoiceDocument1 pageCell Phone Repair InvoiceAmérica DelgadoNo ratings yet
- Contoh Remittance AdviceDocument1 pageContoh Remittance AdviceFATAHILLAH SHOLAHUDDINSWARDANINo ratings yet
- ViewFile PDFDocument2 pagesViewFile PDFNikole MontezNo ratings yet
- BANKSTATEMENTDocument2 pagesBANKSTATEMENTmartinallen1759No ratings yet
- Purchase Order 25Document1 pagePurchase Order 25NoviandryNo ratings yet
- Camille Davidson StatementDocument2 pagesCamille Davidson StatementPeter MariluchNo ratings yet
- Invoice: Charge DetailsDocument2 pagesInvoice: Charge DetailsHaekal FikriNo ratings yet
- Screenshot 2023-10-01 at 4.01.53 PMDocument4 pagesScreenshot 2023-10-01 at 4.01.53 PMptmcmurrayNo ratings yet
- Doctor InvoiceDocument1 pageDoctor Invoicemiranda criggerNo ratings yet
- January 09, 2018Document6 pagesJanuary 09, 2018Monina JonesNo ratings yet
- Images HK Quotation Template WordDocument1 pageImages HK Quotation Template WordIzzied GamingNo ratings yet
- Invoice Template ExcelDocument4 pagesInvoice Template ExcelAmazeKraft IndiaNo ratings yet
- Camille DavidsonDocument2 pagesCamille DavidsonMark WilliamsNo ratings yet
- Medi 2Document4 pagesMedi 2Mere HamsafarNo ratings yet
- QBO-US Aug'23Document1 pageQBO-US Aug'23Ankit VermaNo ratings yet
- Summary of Account Activity Payment Information: Protecting What Matters MostDocument4 pagesSummary of Account Activity Payment Information: Protecting What Matters MostJames BergmanNo ratings yet
- Spending Account StatementDocument2 pagesSpending Account StatementDez SanchezNo ratings yet
- Brand Name3Document1 pageBrand Name3devilking12663No ratings yet
- Benefits SummaryDocument2 pagesBenefits SummaryGustavo StorNo ratings yet
- Images Invoice Template Excel3Document4 pagesImages Invoice Template Excel3perry363No ratings yet
- My Company Name: Price QuoteDocument1 pageMy Company Name: Price QuoteSatvendra SinghNo ratings yet
- Images Invoice Template Excel 3Document4 pagesImages Invoice Template Excel 3PRASHANTH HNo ratings yet
- Consolidate Journal ReportDocument6 pagesConsolidate Journal Reportalagha.zhNo ratings yet
- Bestbuy 1111Document8 pagesBestbuy 1111VictorNo ratings yet
- Waterfall WordDocument2 pagesWaterfall WordDaniel DelbonisNo ratings yet
- Medical in Voice Template 1Document7 pagesMedical in Voice Template 1joel sabastin dassNo ratings yet
- Cell Phone Repair InvoiceDocument1 pageCell Phone Repair InvoiceShailendra SolankiNo ratings yet
- April 2021.Document2 pagesApril 2021.Myt WovenNo ratings yet
- Invoice: Bill From ID Description Price Qty TotalDocument4 pagesInvoice: Bill From ID Description Price Qty TotalMary Anne BantogNo ratings yet
- Invoice: Issue Date Due DateDocument2 pagesInvoice: Issue Date Due DateCheikh Ahmed Tidiane GUEYENo ratings yet
- Bill 107466Document2 pagesBill 107466api-663655760No ratings yet
- Sbseg en Row 2023 Invoice TemplateDocument1 pageSbseg en Row 2023 Invoice TemplatevanessazhaotodoNo ratings yet
- Nevada ADA LawsuitDocument20 pagesNevada ADA LawsuitDave BiscobingNo ratings yet
- AdhAm 2 PDFDocument2 pagesAdhAm 2 PDFAhmed KassemNo ratings yet
- Jon Brown Evolve 0122Document2 pagesJon Brown Evolve 0122Mark DeweyNo ratings yet
- Explanation of Benefits (EOB) - This Is Not A Bill: Track Your Health Care CostsDocument5 pagesExplanation of Benefits (EOB) - This Is Not A Bill: Track Your Health Care CostsRUFFHOUSENo ratings yet
- February Bank StatementDocument1 pageFebruary Bank StatementQuiskeya LLCNo ratings yet
- Medical Template Invoice Word 1Document1 pageMedical Template Invoice Word 1Ezeaka SamuelNo ratings yet
- Invoice 23 FDocument1 pageInvoice 23 FSanjeev ThadaniNo ratings yet
- Secured Card: Trans Post Reference Number Description Credits ChargesDocument3 pagesSecured Card: Trans Post Reference Number Description Credits Chargesinversiones reussi c.a50% (2)
- Invoice 0000001Document1 pageInvoice 0000001Janin MendozaNo ratings yet
- Invoice Template Excel22Document6 pagesInvoice Template Excel22Sushil ThakurNo ratings yet
- Specialty Lens CodesDocument5 pagesSpecialty Lens Codesmiranda criggerNo ratings yet
- Dental Claim FormDocument2 pagesDental Claim Formmiranda criggerNo ratings yet
- Receipt Invoice TemplateDocument1 pageReceipt Invoice Templatemiranda criggerNo ratings yet
- Medical Super BillDocument6 pagesMedical Super Billmiranda criggerNo ratings yet
- Washington Rental Agreement Legal Blank Template PrintableDocument7 pagesWashington Rental Agreement Legal Blank Template Printablemiranda criggerNo ratings yet
- Washington Roommate Agreement Legal Template LeaseDocument6 pagesWashington Roommate Agreement Legal Template Leasemiranda criggerNo ratings yet
- 14 Day Notice Template LegalDocument1 page14 Day Notice Template Legalmiranda criggerNo ratings yet
- Blank Shipping Order Invoice TemplateDocument1 pageBlank Shipping Order Invoice Templatemiranda criggerNo ratings yet
- Pay Rent of Vacat 14 Day Notice LegalDocument1 pagePay Rent of Vacat 14 Day Notice Legalmiranda criggerNo ratings yet
- Legal Residential Month-To-Month Lease AgreementDocument9 pagesLegal Residential Month-To-Month Lease Agreementmiranda criggerNo ratings yet
- Washington STATE14 Day For Evicit Notice Legal TemplateDocument2 pagesWashington STATE14 Day For Evicit Notice Legal Templatemiranda criggerNo ratings yet
- Blank Medical BillDocument1 pageBlank Medical Billmiranda criggerNo ratings yet
- Dental Services RenderedDocument1 pageDental Services Renderedmiranda criggerNo ratings yet
- 14DAYDocument2 pages14DAYmiranda criggerNo ratings yet
- 14DAYDocument2 pages14DAYmiranda criggerNo ratings yet
- 14DAYDocument2 pages14DAYmiranda criggerNo ratings yet
- Real Medical Bill ScanDocument1 pageReal Medical Bill Scanmiranda criggerNo ratings yet
- 14 Comply or Vacat Nonpayment Notice TemplateDocument2 pages14 Comply or Vacat Nonpayment Notice Templatemiranda criggerNo ratings yet
- Methadone InvoiceDocument1 pageMethadone Invoicemiranda criggerNo ratings yet
- CPT Code Dos (Date of Service) Description of ServiceDocument2 pagesCPT Code Dos (Date of Service) Description of Servicemiranda criggerNo ratings yet
- Statement of AccountDocument1 pageStatement of Accountmiranda criggerNo ratings yet
- Methadone ClinicDocument2 pagesMethadone Clinicmiranda criggerNo ratings yet
- Web Payment InvoiceDocument2 pagesWeb Payment Invoicemiranda criggerNo ratings yet
- Co InvoiceDocument1 pageCo Invoicemiranda criggerNo ratings yet
- Heart Doctor Medical Bill ExampleDocument1 pageHeart Doctor Medical Bill Examplemiranda criggerNo ratings yet
- Methadone Clinic InvoiceDocument2 pagesMethadone Clinic Invoicemiranda criggerNo ratings yet