Professional Documents
Culture Documents
PN 2023 003817.full
PN 2023 003817.full
Uploaded by
Henrique OliveiraOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
PN 2023 003817.full
PN 2023 003817.full
Uploaded by
Henrique OliveiraCopyright:
Available Formats
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
Alcohol and the central nervous system
Maytal Wolfe,1,2 Arun Menon,1,3 Maria Oto,2 Natasha E Fullerton,1,2
John-Paul Leach 2
► Additional supplemental ABSTRACT and sociological harms. A recent survey
material is published online
Ethanol use is common to most cultures but of UK drug users found that 32 out of 93
only. To view, please visit
the journal online (http://dx. with varying doses and to varying extents. respondents had experienced more harm
doi.org/10.1136/pn-2023- While research has focused on the effects from alcohol compared with many other
003817). on the liver, alcohol exerts a range of actions substances due to its ready availability,
1
University of Glasgow,
on the function and structure of the nervous potential for addiction, its risk of death
Glasgow, UK system. In the central nervous system (CNS) it from acute and chronic effects, social
2
Queen Elizabeth University can provoke or exacerbate neurological and harms and the dangers of withdrawal.3
Hospital, Glasgow, UK psychiatric disease; its effects on the peripheral Excessive consumption often begins in
3
Gartnavel Royal Hospital,
Glasgow, UK nervous system are not included in this review. youth, but alcohol overuse is not the
Sustained alcohol intake can predispose to preserve of the young, with UK surveys
Correspondence to acute neurochemical changes which, with showing that 38% of men and 19% of
Professor John-Paul Leach,
Queen Elizabeth University
continued ingestion and incomplete treatment, women drink more than the recom-
Hospital, Glasgow, G51 4TF, UK; can lead to chronic structural changes in the mended limits of alcohol.4
j pleach246@me.c om CNS: these include generalised cortical and Predictions of future consumption are
cerebellar atrophy, amnesic syndromes such as not encouraging. The decade up to 2019
Accepted 14 May 2023
Korsakoff’s syndrome, and specific white matter saw a 19% rise in alcohol- related UK
disorders such as central pontine myelinolysis hospital admissions to over 350 000 per
Protected by copyright.
and Marchiafava–Bignami syndrome. Alcohol in year. People from the most deprived areas
pregnancy commonly and significantly affects (and especially men) were most likely
fetal health, though this receives less medical to be admitted to hospital with alcohol-
and political attention than other causes of fetal related problems.5 In the same time
harm. This review looks at the range of disorders frame, the rate of alcohol-related deaths
that can follow acute or chronic alcohol use, and had increased by 7%, with indications of
how these should be managed, and we provide increasing incidence in most but not all
a practical overview on how neurologists might countries.6–8
diagnose and manage alcohol addiction. Most research and campaigning has
focused on hepatic damage, but the central
nervous system (CNS) is particularly
INTRODUCTION susceptible to the chemical chaos wrought
Ethanol consumption is normalised in by excessive consumption both acutely
most cultures around the world.1 It is one and chronically. The pattern of neurolog-
of the substances of abuse that is toler- ical change is complicated by the multiple
ated, and in fact capitalised on by local medical, nutritional and sociological asso-
and regional governments, forming a ciations of alcohol excess, many of which
significant part of the economy of many can result from, or predispose to alcohol-
western democracies. The UK Institute related harm. While the medical harm
of Alcohol Studies reported in 2020 that reflects the rate and extent of alcohol
alcohol comprised around 2.5% of the intake, social factors increase this risk, as
UK’s gross domestic product, totalling do a range of as-yet unidentified genetic
around £46 billion, of which £11 billion factors. Comorbidities influence the CNS
© Author(s) (or their
accrued directly from alcohol taxation.2 response, including general medical status
employer(s)) 2023. No Unlike other drugs of abuse, the socio- and nutritional state, prior liver disease,
commercial re-use. See rights logical constructs and habits around head injury, underlying fetal alcohol spec-
and permissions. Published
by BMJ.
alcohol make its frequent use easy and trum disorder and underlying (and possibly
acceptable, and abstinence from alcohol secondary) psychiatric diagnoses such as
To cite: Wolfe M, Menon A, difficult to maintain. So, while the social depression, anxiety, schizophrenia and/or
Oto M, et al. Pract Neurol Epub
ahead of print: [please include effects of alcohol at moderate doses may concomitant antipsychotic and antianx-
Day Month Year]. doi:10.1136/ be regarded as acceptable, increased iety medications.9 Additional complexity
pn-2023-003817 intake contributes to significant medical comes from patients’ experiences of
Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817 1
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
‘self-managing’ their own mental health, particularly revision of the international classification of diseases
since this may be difficult to detect. Left unchecked it (ICD 11) came into effect in January 2022 and is grad-
ultimately serves only to hamper treatment and moni- ually being incorporated into clinical practice.14 These
toring of associated common psychiatric conditions or include updated definitions of alcohol use disorders.
neurological disorders, such as epilepsy and dementia. Hazardous alcohol use substantially increases the risk
of harm to an individual’s physical or mental health or
Problematic alcohol use in a social/holistic context
risk of behaviour that harms others. A ‘harmful pattern
Alcohol intake is more than a medical problem, and it is of use of alcohol’ is defined as repetitive use of alcohol
very important to see the broader difficulties in context. that has caused such harms, and which persists despite
Richard Billingham’s book ‘Ray’s a Laugh’ provides this. Alcohol dependence is defined by the presence of
valuable insight into the extent and wide-ranging phys- any two of three diagnostic criteria:
ical, mental and social consequences of alcohol depen- 1. Impaired control over alcohol use.
dence.10 The aim of addictions services is not solely 2. Priority of alcohol use over other activities.
abstinence (although this may suit the majority): care 3. Physiological features of dependence (eg, tolerance,
needs to be taken, since repeated alcohol withdrawal withdrawal, and repeated alcohol use to alleviate with-
has neurotoxic potential and has observable effects on drawal symptoms).
cognition.11 A pragmatic harm- reduction approach Clinicians in the UK should also be familiar with the
may be required, and clinicians need to be mindful of Driver and Vehicle Licensing Agency (DVLA)’s definitions
the complexity of patients with addictions and provide of alcohol misuse and alcohol dependence that apply to
person-centred and trauma-informed care. driving eligibility. These are not especially useful in clin-
In this article, we outline the nature and extent of ical practice but knowledge of them helps in advising
alcohol’s CNS effects and provide guidance on the patients and other health professionals about the condi-
diagnosis and monitoring of alcohol- related neuro- tions required for return of driving privileges.15
logical problems. However, we will not address the In terms of quantifying healthy limits of alcohol
significant peripheral neurological sequelae caused by use, although there is no absolute safe limit, the UK
alcohol, such as neuropathy and myopathy. government currently recommends a maximum of 14
Protected by copyright.
EFFECTS OF ALCOHOL ON NEUROTRANSMISSION units per week, spread over 3 or more days, along with
Clinical manifestations of acute alcohol ingestion several drink-free days per week.16 In the UK, one unit
were long held to relate to GABA receptor agonism is defined as 10 mL or 8 g of pure ethanol. This can be
and glutamate receptor antagonism (particularly calculated by multiplying the total volume of a drink
the NMDA subtype). Variations in susceptibility of in millilitre by the percentage alcohol by volume (the
GABA- A receptor subunits may explain why some percentage of volume of the drink that is pure ethanol).
brain regions with high prevalence of delta subunits England’s National Institute of Health and Care
are more affected at lower alcohol concentrations than Excellence (NICE) guidelines outline a strategy for
others.12 13 Acute adaptation in the CNS results in invo- initial screening for alcohol use disorders.17 Assess-
lution of GABA receptors in response to continued ment should include formal tools, such as AUDIT (a
effects of alcohol. The simultaneous upregulation of 10-question self-report questionnaire with questions
NMDA receptor activity and reduced GABA receptor on hazardous use of alcohol, dependence symptoms
function becomes problematic with abrupt cessation of and harmful use of alcohol).18 Due to its complexity,
alcohol, when the resultant imbalance in neurotrans- despite its presence in the NICE guidelines, AUDIT is
mitters leads to neurotoxicity and the rapid onset not as easy for clinicians to remember and administer;
of psychiatric difficulties and/or seizures described for this reason, the CAGE questionnaire has persisted
below. Genetic variations in receptor pharmacology in clinical settings19 (see table 1). However, CAGE is
may contribute to individual variations in response to not sensitive to heavy drinking and does not distin-
alcohol ingestion and withdrawal. Recognised factors guish between previous and current drinking.
affecting acute response to alcohol include tolerance
mediated by chronic effects on GABA and NMDA
receptor expression and rate of ingestion. Positron
emission tomography has helped to understand other
broader neurochemical effects on neurotransmitter Table 1 The CAGE questionnaire
function, which encompass opioid, dopaminergic and
C Have you ever felt you should Cut down on your drinking?
serotonergic systems that may underly some of the
A Have people Annoyed you by criticising your drinking?
other features around addictive behaviour.12
G Have you ever felt bad or Guilty about your drinking?
DIAGNOSIS AND QUANTIFICATION OF ALCOHOL E Have you ever had a drink first thing in the morning to steady
EXCESS your nerves or to get rid of a hangover (Eye opener)?
A focused alcohol intake history is an essential part * A total of two or more ‘Yes’ answers is considered clinically
of the neurological consultation. The WHO’s 11th significant for diagnosis of problem drinking (Bradley 1992)
2 Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
As a result, attempts have been made to validate it is increased in around 10% of patients who also take
an abbreviated version of AUDIT (named AUDIT-C), enzyme- inducing antiseizure medications. The full
which includes only three items (typical frequency and blood count may include a raised mean corpuscular
quantity of drinking and frequency of drinking six or volume (even with normal folate and vitamin B12),
more drinks on one occasion) and has been shown to and a reduced serum urea may also indicate impaired
be effective in screening for alcohol dependence or hepatic function.
heavy drinking warranting further assessment.20
Carbohydrate-deficient transferrin
LABORATORY TESTS OF EFFECTS OF ALCOHOL Transferrin is a transport protein for iron, and high
INTAKE alcohol intake will increase the proportion of the
Acute protein that has reduced sialic acid. This appears to
Blood alcohol concentration rise when alcohol intake exceeds four units per day.
The use of one-off measurement of serum alcohol fell Some studies have suggested that this carbohydrate-
out of favour when results were used inappropriately deficient transferrin (CDT) is a more sensitive and
in legal arenas. Measurement can however be essential specific marker of alcohol excess than GGT.21 CDT
(in assessing whether lowered conscious level may be is not routinely used in clinical practice but may be
secondary to intoxication) and may help in non-acute required by some organisations (eg, DVLA) to provide
situations, particularly where it is suspected that there optimal evidence of abstinence in someone with a prior
is ongoing use of alcohol. This should not be done diagnosis of alcohol misuse or alcohol dependence.
covertly.
General health and nutritional assessment
Chronic
Serum magnesium and phosphate can help in assessing
Liver function tests
both the degree of metabolic upset caused by alcohol
As well as measuring serum alcohol, liver function tests
and the need for replacement of these elements. Clini-
can help in assessing the long-term effects of alcohol,
cians should consider the risk of refeeding syndrome
although these may be normal in the later stages of
when admitting alcohol-dependent patients to hospital.
liver disease. Serum gamma glutamyl transferase
Protected by copyright.
(GGT) is the most sensitive of these routine tests, but
CLINICAL EFFECTS ON THE CNS—ACUTE
Intoxication
The acute CNS effects of alcohol are familiar across the
globe and include emotional instability impaired judge-
ment, inappropriate behaviour and cerebellar signs
(slurred speech, incoordination, ataxia, nystagmus).13
With higher doses, there may be memory impairment
and stupor at very high doses. Respiratory depres-
sion is a risk at serum alcohol concentrations above
300 mg/dL; death from alcohol intoxication can result
at concentrations above 500 mg/dL. Acute effects are
dose related, but the individual response is heavily
affected by individual tolerance and prior exposure.
In a patient presenting with a reduced level of
consciousness and smelling of alcohol, it may be
hazardous to assume that alcohol is the cause. It
is important to consider a differential diagnosis,
including subdural haematoma (with the possibility of
a higher risk of trauma combined with risk of possible
dysfunctional coagulation and cerebral atrophy),
metabolic abnormality (especially hypoglycaemia) and
a structural brain lesion.22 Evidence of trauma or focal
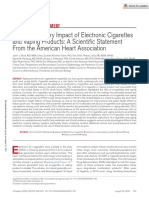
Figure 1 Unenhanced CT brain in a middle-aged man with neurological signs should prompt imaging to exclude
alcoholic liver disease presenting to the emergency department another cause (figure 1).
after a fall when intoxicated. The scan shows alcohol-related
trauma. There are bilateral convexity subdural collections Blackouts
(arrows) of various density in keeping with acute on chronic
The term ‘blackouts’ refers to episodic amnesia expe-
subdural collections. There is further an extradural collection
overlying the right parietal lobe (asterix) with acute blood of
rienced after acute intoxication and usually indicates
various densities, suggesting ongoing bleed, likely secondary to that serum alcohol concentrations have been signifi-
coagulopathy. A small subcutaneous haematoma can be seen cantly high. Although historically, blackouts have indi-
from a recent fall overlying the right frontal bone (arrowhead). cated ‘alcoholism’, it is now clear that they happen in
Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817 3
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
people with and without alcohol dependence. They small creatures. Auditory and tactile hallucinations
probably result from memory being disrupted before can also occur. Generalised seizures can emerge.26
motor control is lost with increasing intoxication.23 Perhaps 2%–5% of patients in hospital suffer from
Interestingly, alcohol’s effects on memory may be delirium tremens, with a mortality rate of 1%–15%.27
complex and there are reports of people who can Although symptoms commonly last between 1 and
recall while drunk where they have secreted alcohol or 7 days, they can persist for several weeks. Prolongation
money, which they could not remember when sober. is more common in those with a history of using illicit
CA1 pyramidal cells in the hippocampus are prob- substances (eg, benzodiazepines), comorbid dementia
ably affected by alcohol in a dose-dependent fashion, or head injury. As with withdrawal, the mainstay of
leading to disruption of transfer of long-term encoding treatment is benzodiazepines (often at very high
of short-term memory. There are two documented doses), but low doses of antipsychotics can be added to
forms of blackout: en-bloc blackouts in which there is help manage agitation associated with hallucinations.
inability to remember events during a discrete period
of time, and fragmentary blackouts in which there Seizures
is incomplete disruption of recall. The most signifi- While some sources suggest that seizures can be
cant risk factor for blackout is the rate of increase in precipitated by high amounts of alcohol, this would be
blood alcohol concentration. Adolescents and young an unusual result of excessive GABAergic stimulation
people may be particularly susceptible to blackouts, in adult humans. Sustained alcohol intake can reduce
not only due to their impulsive drinking patterns but the time spent in REM sleep, and the coingestion of
also due to the susceptibility of the developing hippo- other compounds may play more of a part than the
campus.24 Studies measuring blood alcohol concen- alcohol itself. Low serum concentrations of phosphate
trations compared with placebo show that younger and magnesium may suggest a higher risk of electro-
subjects perform poorly on tests of semantic and non- lyte disturbance with refeeding, which in theory may
verbal memory when intoxicated compared with older be proconvulsant, although this is probably rare in
subjects. Women are also at increased risk of blackouts alcohol detoxification.28 29 Subacute encephalopathy
and slower recovery from cognitive impairment. with seizures in alcoholics (SESA) was first described
Protected by copyright.
Susceptibility to en-bloc blackouts is also increased in the 1980s, this syndrome includes patients with
with ingestion of other substances, including cannabis prolonged confusion who have conditions along the
and benzodiazepines. ictal-
interictal spectrum, including non- convulsive
status.30 While SESA is not a necessary term, it acts
Acute withdrawal state as a prompt for investigating with EEG or using EEG
An acute withdrawal state typically occurs within monitoring in this situation.30
6–48 hours of a sudden reduced intake in someone Seizures directly provoked by alcohol withdrawal
with alcohol dependency.25 The neurological effects are usually self-limiting and are an indication for
result from the combination of chronically downregu- benzodiazepines, thiamine and glucose loading. Esca-
lated GABA receptors and upregulated NMDA recep- lation to use of antiseizure medications and, if neces-
tors in the absence of alcohol. The relative deficiency sary, admission to an intensive care unit (ICU) may
of GABAergic effects and excessive glutamatergic stim- still be required if immediate response is incomplete.
ulation lead to symptoms including confusion, rigidity, These ‘provoked seizures’ should not be regarded as
tremor, anxiety and excessive sweating. The treatment trivial. The 1-year mortality after admission to ICU
is with either fixed doses or as-required dosing with with seizure is around 35% in patients with a history
benzodiazepines when symptoms occur. NICE guide- of alcohol dependence or drug use.31 Continued
lines recommend giving symptom-triggered benzodi- obtundation post-ictally may justify EEG to exclude
azepines using a structured tool such as the revised non-convulsive status epilepticus. Where seizures are
clinical institute withdrawal assessment alcohol scale exclusively clearly related to alcohol withdrawal, each
for withdrawal in hospital settings.17 Patients with one having attendant preceding withdrawal symptoms,
recent high alcohol intake and previous history of then the focus should ideally be on preventing future
severe withdrawal require a regular regimen.22 occurrence of severe withdrawal to reduce risk of
long-term neurotoxicity. Where there is an unclear or
Delirium tremens at best tenuous relationship to withdrawal, antiseizure
Where withdrawal is more severe, particularly on a medication will come into play for some. Where there
background of more severe dependence, the clinical is such doubt, we feel it is safer to begin antiseizure
situation can progress to delirium tremens on the medication, a view justified by the risks of harm from
third to fifth day after withdrawing. This state is char- continued or prolonged seizures. There is no clear
acterised by the acute onset of hallucinations, agita- evidence of benefit of any particular antiseizure medi-
tion, autonomic hyperactivity, hand tremulousness cation in patients with provoked seizures, but given
and nausea. Visual hallucinations are most common, the risk of incomplete adherence in patients prone to
classically in the form of Lilliputian hallucinations of excess alcohol intake, a reasonable strategy is slowly to
4 Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
titrate a well-tolerated, non-enzyme-inducing antisei- duration of psychotic symptoms was 4 days, and
zure medication, with a moderate (eg, lamotrigine) or most reported hallucinations only when decreasing
long (eg, zonisamide) half-life. Levetiracetam should their alcohol intake or abstaining from alcohol.32
be avoided where there is an underlying acute or The authors point out that twothirds of patients
chronic mood disturbance. Monitoring serum concen- had previous episodes of alcohol-r elated psychosis,
trations of long-term antiseizure medication may help highlighting risk of recurrence. There is no clear
to ensure adherence; ready access to laboratory facil- consensus on the nature of alcohol- i nduced
ities may influence the choice of antiseizure medica- psychotic disorder; some highlight similarities
tion if this is an important part of planned clinical with delirium tremens, for example, a tendency
management. towards physical symptoms and slight clouding of
consciousness, and others favour a conceptualisa-
Hallucinosis—alcohol-induced psychotic disorder tion closer to a schizophrenia-like illness indicated
Hallucinations in the context of alcohol use by auditory hallucinations in clear consciousness
were described as a separate entity from delirium and chronic course of the condition. 34 Alcohol-
tremens by Marcel in 1847. Bleuler coined the induced psychotic disorder has no accepted stan-
term alcoholic hallucinosis in 1916, the modern dard treatment, but improvement usually requires
term being alcohol-i nduced psychotic disorder. 14 32 abstinence from alcohol and use of antipsychotic
Lifetime prevalence of alcohol-induced psychotic drugs to treat psychotic symptoms. Some have
disorder ranges from 0.4% in Germany to 12.4% in suggested that initial treatment with benzodiaze-
Nepal. By the ICD11 definition of alcohol-i nduced pines helps in only some cases. 35
psychotic disorder, prominent psychotic symp-
toms occur during or shortly after intoxication or CLINICAL EFFECTS ON THE CNS—CHRONIC
withdrawal from alcohol, and symptoms should be Alcohol-related brain damage
more than those usually found in alcohol intoxica- Alcohol-r elated brain damage is the unofficial, but
tion or withdrawal. The symptoms should improve widely-u sed term encompassing a wide spectrum
and usually resolve with a significant period of of pathology and cognitive impairment related to
Protected by copyright.
abstinence from alcohol.33 The literature highlights alcohol, including Wernicke-Korsakoff syndrome,
characteristic features, including typical auditory and conditions resulting from direct toxic effects of
hallucinations of an acute onset, hallucinations alcohol and also effects of head injury and stroke
of derogatory voices and persecutory delusions. related to alcohol.36 37 The lack of accepted defini-
These usually occur in clear consciousness and in tion can sometimes create difficulties. DSM-V clas-
the absence of the thought-d isorder typically seen sifies alcohol-r elated cognitive disorders as mild
in other forms of psychosis, but around 10% may and severe alcohol-r elated neurocognitive disorder,
have features of delirium in the acute stage of the amnestic and non- a mnestic38 (see online supple-
disorder. Alcohol-i nduced psychotic disorder tends mental case 1). This diagnosis is supported by
to occur later in life and has a better prognosis than other signs of long-term systemic effects of alcohol,
other psychoses. Among 61 inpatients, the mean for example, cirrhosis, ataxia or peripheral sensory
Figure 2 Patient with alcohol-related brain damage (ARBD) after prolonged alcohol abuse presenting with cognitive issues.
An unenhanced helical CT scan (A) shows disproportionate frontal lobe atrophy (arrows), a frequent finding after heavy alcohol
consumption. Tc-99m HMPAO perfusion SPECT imaging (B) shows frontal cortical reduction in brain perfusion (arrows), which can be
seen secondary to chronic alcohol abuse or acute intoxication.
Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817 5
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
Figure 3 Appearances of Wernicke encephalopathy on MR brain scans from an elderly (A–C) and a middle-aged man (D–F)
presenting with prolonged alcohol abuse, confusion and cognitive impairment, ataxia and falls and nystagmus and oculomotor
Protected by copyright.
signs. MR scan of brain showing symmetrical, high signal on T2-weighted and T2 FLAIR imaging, as well as on diffusion-weighted
imaging affecting periaqueductal grey matter, medial thalamus, mamillary body and hypothalamus (arrows). Post-contrast imaging
(C) shows corresponding enhancement (arrows). Brain atrophy for age is noted in the younger patient.
neuropathy, cardiac effects as well as evidence of cognitive assessment is currently the most well-
cerebellar atrophy on neuroimaging. According to validated method of screening and distinguishing
Oslin’s diagnostic criteria, the clinical diagnosis alcohol-
r elated brain damage from other causes
should be made at least 60 days after the last expo- of cognitive impairment, although more detailed
sure to alcohol.39 neuropsychological assessment is required in making
the diagnosis and characterising difficulties.41
Pathophysiology
In alcohol-related brain damage, the frontal lobes Treatment and prevention
appear particularly vulnerable to glutamate excito- Improvement or recovery in function can continue
toxicity, oxidative stress and disruption of neurogen- following a substantial period of abstinence from
esis.40 Cycles of bingeing and withdrawal probably alcohol over a period of weeks to months.42 43
predispose to upregulation of NMDA receptors and Repeated episodes of withdrawal probably contribute
effects on cholinergic transmission in the basal fore- to alcohol-related brain damage, hence it is best to
brain. Almost 80% of alcohol- dependent people avoid severe withdrawal syndrome and emergency
have brain changes at postmortem, leading to frontal detoxes, and rather to plan detoxification.11 Planned
lobe volume loss and atrophy. Functional imaging, inpatient detoxification under addiction services is
including 99mTc-HMPAO SPECT assessing cerebral very different to emergency detoxification in an acute
perfusion and blood flow, can show decreased frontal medical setting, which focuses on preventing acute
perfusion in alcohol abuse and alcohol-related brain morbidity and mortality. Additional time, planning
damage (figure 2) and expertise is needed to promote long-term absti-
nence with appropriate emphasis on general rehabili-
Clinical features tation and long-term care.
As suggested by the pathology, frontal cognitive
deficits are common. Compared with Alzheimer’s, Wernicke/Korsakoff’s
patients with alcohol-
r elated brain damage have Wernicke’s syndrome classically represents the acute
better semantic and verbal memory and poorer effects of CNS nutritional deficiency whereas Korsa-
performance in visuospatial tasks. 36 The montreal koff ’s represents the chronic effects. However,
6 Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
Figure 4 (A–C) MR scan of brain in a patient in their late 40s, admitted with alcohol-related problems, showing cerebellar, in
particular superior vermian and mamillary body atrophy (arrows).
in clinical practice, a mixed picture is much more gravidarum and malignancy. People with alcohol
common. Chronic alcohol use leads to poor nutrition dependence are at particular risk of Wernicke’s due
and vitamin B1 deficiency causing symmetrical lesions to poor nutrition, decreased capacity for hepatic
Protected by copyright.
in thalamus, hypothalamus, mammillary bodies and nutrient storage and decreased vitamin absorption.
periaqueductal grey matter. Thiamine is a cofactor for A diagnosis of Wernicke’s is based on Caine’s clas-
several enzymes in the Krebs cycle and involvement in sification requiring two of four features of dietary
transketolase and glucose metabolism leads to build-up deficiency, eye signs (ranging from subtle nystagmus
of toxic metabolites. The neuropathology is varied but to complete ophthalmoplegia), cerebellar dysfunc-
is usually associated with some degree of brain volume tion and altered mental state.46 Altered mental
loss.44 Wernicke’s pathology includes symmetrical state is the most common feature and severity
lesions around the third ventricle, aqueduct and fourth can vary from disorientation to coma. Nutritional
ventricle, with mamillary body involvement in up to replacement is vital and should be immediate if the
80% of cases. Some studies identify particular effects diagnosis is suspected. There is no international
on white matter volume, although this is not a uniform consensus on optimal dosing with thiamine, but
finding. Prefrontal white matter, and the genu of the in the UK, there is a widely accepted standard of
corpus callosum appear to be particularly suscep- replacement doses 500 mg intravenous thiamine
tible in Wernicke-Korsakoff syndrome, the degree of three times per day for 2 or 3 days followed by
white matter loss probably correlating with the degree 250 mg intravenously three times per day for the
of alcohol consumption. Figure 3 shows the typical next 2 or 3 days, followed by oral thiamine.47–49
imaging findings. Continuing disorientation would justify continuing
treatment with parenteral thiamine. Anaphylaxis
Wernicke’s syndrome due to thiamine preparations is very rare. 22 Since
Wernicke’s syndrome refers to the classic triad of signs of Wernicke’s can be non-s pecific, it is a good
oculomotor signs (classically ophthalmoplegia), practice to treat prophylactically if alcohol depen-
cerebellar signs and altered mental state (See dence is suspected or detoxification is planned,
online supplemental case 2). However, the classic using once daily parenteral thiamine for 5 days.
Wernicke’s triad occurs in only 10% of cases. Carl
Wernicke first described this syndrome in 1881 in Korsakoff’s
a case series.45 Of note, one of his cases was not Korsakoff syndrome describes the syndrome of
alcohol related but was a young woman with nutri- persistent residual cognitive impairment, often where
tional deficiency due to pyloric stenosis. This high- Wernicke’s has been incompletely treated. There
lights the role of thiamine deficiency in the clinical is ongoing debate as to whether these are part of a
manifestations and that Wernicke’s is not unique to continuum of features that can be grouped with other
alcohol misuse but is a risk associated with malab- types of alcohol- related brain damage or whether
sorption from any cause, including hyperemesis Korsakoff ’s is a pure syndrome related exclusively
Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817 7
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
prominent in assessment of gait and the lower limbs.
The clinical features of a cerebellar ataxia may be exac-
erbated by a coincident peripheral neuropathy.
Marchiafava–Bignami disease
This is a rare and poorly understood clinical constella-
tion first described in the early 20th century. The most
common features include personality change, enceph-
alopathy, and gaze disorders, occasionally alongside
seizures.56 A corpus callosal syndrome may become
apparent with visual and tactile anomia, hemi-alexia,
unilateral left-sided apraxia and absence of interhemi-
Figure 5 (A,B) MR scan of brain (sagittal and coronal)
showing corpus callosal changes of Marchiafava-Bignami
spheric transference of unilateral somatosensory stim-
disease. Images courtesy of Radiopedia. ulation of both hands.57 Other features of the damage
wrought by alcohol can include longstanding cognitive
decline, gait problems and incontinence. Focal neuro-
to thiamine deficiency. The most important contrib- logical deficits such as hemiparesis, aphasia and apraxia
utory factor is delay in thiamine replacement. In its are less helpful in differentiating from other causes of
clinical features, Korsakoff syndrome has been defined corpus callosal lesions. Imaging findings are usually
by a disproportionate impairment of declarative centred on the corpus callosum, with changes ranging
memory (especially episodic and semantic) in an alert from oedema to cystic lesions. MR brain imaging
patient. In addition, most of the memory loss tends (figure 5) shows progressive demyelination and ulti-
to be anterograde, with disproportionate loss of more mately necrosis of corpus callosum, affecting the body
recent memories, known as Ribot’s law.50 This is well- of corpus callosum, followed by genu and ultimately
illustrated in the case of Jimmy in Oliver Sacks’ book, splenium, leading to classical imaging appearances of
‘The Man Who Mistook his Wife for a Hat’.51 Other callosal degeneration with cystic cavities. Occasionally
Protected by copyright.
features consistent with Korsakoff ’s include apathy, similar lesions may also develop in the corticospinal
executive dysfunction, lack of insight and confabula- tracts, cerebellar peduncles and the hemispheric white
tion. There is no widely accepted treatment available matter. Treatment involves avoiding alcohol and nutri-
for Korsakoff ’s syndrome. tional replacement with thiamine alongside B12 and
folate. Some have suggested that prognosis is better in
Dementia due to use of alcohol those with unimpaired level of consciousness.58
ICD-11 has this as a specific category of effect.14
There is an interesting ‘J-shaped’ relationship between Osmotic demyelination
patterns of alcohol use and dementias. This is thought Patients with chronic excessive alcohol consump-
to be due to protective effects of low levels of alcohol tion are more prone to significant hyponatraemia via
consumption, resulting from associated reduction in various mechanisms including hypovolaemia, drinking
platelet aggregation, inflammatory markers and lipids. excessive salt-
poor solutes (eg, beer), cerebral salt
Meta-analysis suggests that this protects only against wasting syndrome and reset osmostat syndrome.59
Alzheimer’s dementia but not vascular dementia.40 A Rapid correction of this can cause acute onset of demy-
cohort study of people admitted to hospital over 5 elination in some white matter tracts, most evident in
years in France found that alcohol use disorders were the pons. A recent review of clinical and neurolog-
strongly associated with all risk factors for dementia ical features listed signs including most commonly
onset, particularly with early-onset dementia.52 encephalopathy and dysphonia (50%), less so with
extrapyramidal symptoms and seizures. Neuroimaging
Cerebral and cerebellar atrophy results (figure 6) showed central pontine myelino-
Light-to-moderate drinking in an elderly cohort may lysis in 11/18, in seven accompanied by extrapontine
lower the risk of cerebral atrophy especially if the myelinolysis. Five patients (27.8%) had extrapontine
alcohol is taken as wine rather than beer or spirits, myelinolysis only. The prognosis appeared better in
but this has been countered in studies of younger those presenting with encephalopathy rather than
cohorts.53 54 Both nutritional deficiency and trauma focal neurological signs.60 Osmotic demyelination may
can exacerbate the generalised atrophic effects of occur largely asymptomatically and be detected inci-
alcohol (figure 4). Mamillary body atrophy correlates dentally during later imaging.61
with the cognitive issues described above. In addition
to cortical atrophy, there may be particular mecha- Fetal alcohol spectrum disorder
nisms for the effects of alcohol on the cerebellum.55 The frequency and severity of this condition merits
They lead to neuropathological effects more promi- further consideration. Given the range of neurochem-
nent in the cerebellar vermis, and clinical effects more ical effects exerted by alcohol, it is not surprising that
8 Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
Figure 6 CT and MRI images show central pontine myelinolysis (CPM) as part of an osmotic demyelination syndrome (ODS) in a
middle-aged patient with a history of alcohol excess and an admission with severe hyponatraemia rapidly corrected on admission.
The initial CT scan (A) shows centrally low density changes at the level of the pons (asterix). In addition, well seen on the sagittal CT
images, there is cerebellar atrophy (arrowhead) reflecting alcohol-related cerebellar degeneration. Further, there is some mamillary
body atrophy (arrows), related to thiamine deficiency in alcoholic liver disease, and cognitive dysfunction. The axial T2 TSE MRI
sequence (B,C) shows high signal centrally in the pons (asterixes) involving transverse pontine fibres, with sparing of the peripheral
and corticospinal tracts, leading to a three-pronged spear appearance, described as a ‘trident sign’ found in CPM.
prenatal exposure to alcohol affects the developing (table 2), comprising short palpebral fissures, smooth
Protected by copyright.
brain. Fetal alcohol spectrum disorder describes a spec- philtrum and thin upper lip.65
trum of physical and neurological abnormalities related Standardised scales have been developed for
to prenatal alcohol exposure.62 This disorder probably assessing physical signs. Studies suggest FASD
has a greater population impact than other syndromes of behavioural phenotypes score highly for hyperkinetic
prenatal harm; prenatal alcohol exposure globally affects
behaviours as well as anxiety and emotional problems.
an estimated 7.7 per 1000 live births, with estimated UK
prevalence of fetal alcohol spectrum disorder of around There is significant recognised overlap with attention-
32.4 per 1000 live births. This is likely to be an under- deficit hyperactivity disorder and autistic spectrum
estimate, and there have been calls for coordinated and disorders, and studies indicate that in those with good
standardised assessment and management of patients language skills, difficulties with understanding and
affected by this condition.63 The pathophysiology of social skills may remain well hidden. Given this vari-
prenatal damage is unclear, but MR imaging studies ability and its high prevalence, it is highly likely that
have shown the effect of alcohol in the corpus callosal FASD diagnosis may only become apparent in adult-
anatomy.64 Whether this is a primary or secondary effect hood. Such patients may already be known to the
is unknown. judicial system or mental health services. By the time
Clinical features of fetal alcohol spectrum disorder
the diagnosis is made, the only measures required are
Around 10% of patients with fetal alcohol spectrum to treat the emergent symptoms. The recent guide-
disorder have characteristic or ‘sentinel’ facial features lines describe a need for standardised and coordinated
multidisciplinary patient- centred assessment and
management.63
Table 2 Fetal alcohol spectrum disorder (FASD) diagnostic criteria
FASD with sentinel features FASD without sentinel features At risk
All three sentinel facial features (short palpebral No sentinel facial features Prenatal alcohol exposure confirmed
features, smooth philtrum, thin upper lip)
Prenatal exposure to alcohol confirmed or unknown Prenatal alcohol exposure confirmed Diagnostic criteria for FASD not met
Severe impairment in three or more Severe impairment in three or more Some indication of neurodevelopmental
neurodevelopmental areas neurodevelopmental areas disorder but does not meet criteria for
significant impairment
Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817 9
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
Protected by copyright.
Figure 7 Woman with alcohol excess and known liver disease. MR scan of brain (A–D) shows features suggestive of hepatic
or hyperammonaemic encephalopathy (arrows). High T1-weighted signal globus pallidus in keeping with mineral deposition
(arrowheads). Symmetrical high FLAIR signal involving basal ganglia, affecting caudate and to a lesser degree lentiform nuclei,
further thalamus, posterior limbs of the internal capsule, and also cingulate gyrus, insula and splenium, in addition to centrum
semiovale and corona radiata. Subtle peri-aqueductal and mamillary body high T2-weighted signal also noted in addition to some
mamillary body atrophy and marked frontal lobe atrophy (asterixes).
INDIRECT EFFECTS OF ALCOHOL ON THE CNS— there is persisting disorientation or encephalopathy,
ACUTE it may be justified to screen for other substances that
Trauma might be perpetuating any psychiatric or neurological
The impaired motor skills and disinhibition of acute features, as this could help with prognostication and
intoxication lead not only to more risky behaviours perhaps with treatment.
but also the reduced ability to enact protective reflexes.
Alcohol excess in itself probably increases the chances
of direct traumatic brain and neurological injury, INDIRECT EFFECTS OF ALCOHOL ON THE CNS—
and any sign of trauma or focal neurological deficit CHRONIC
should prompt further neurological monitoring and/ Hepatic encephalopathy
or investigation. The liver’s role in dealing with products of protein
breakdown clears the body of many tertiary and
Exposure to other substances quaternary amines. Where this is impaired, this
Patients prone to alcohol excess commonly ingest leaves the normal CNS function compromised by
other substances. In 2020, the Office for National false neurotransmitters, manifests as hepatic enceph-
Statistics noted that the proportion of adults reporting alopathy.68 An acute- on-
chronic overuse of alcohol
drug use increased substantially with higher alcohol can provoke this, but other sudden metabolic stress
use; nearly 15% of people drinking on more than (systemic infection, gastrointestinal bleed causing an
3 days per week reported use of any drug, over 10% acute ‘protein load’ or localised peritoneal infection)
reported cannabis use and over 5% reported cocaine should not be overlooked. Clinicians should suspect
use.66 As with alcohol use, this may not be volunteered the diagnosis in someone with a prior history of hepatic
and may be deliberately concealed. Such substances disease, developing a subacute delirium or reduced
might contribute to the clinical presentation and might conscious level. Blood testing will show deranged liver
reduce or attenuate the clinical recovery.67 Where function tests and raised serum ammonia. Imaging is
10 Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
Figure 8 MR spectroscopy shows a Glx complex (blue circle) including glutamine and glutamate peaks between 2.2 and 2.5 ppm
in lesional voxels and ‘normal’ white matter—a finding in hepatic encephalopathy secondary to brain hyperammonaemia. MR
Protected by copyright.
spectroscopy overall would be compatible with hepatic encephalopathy.
usually normal, and EEG shows generalised slowing. Chronic trauma
Despite long- held belief about the specificity of Chronic alcohol use is often noted to be associated
triphasic waves, the EEG findings are usually non- with cortical atrophy and it has been suggested that
specific and not always easily differentiated from EEG alcohol potentiates and exacerbates the atrophic
in encephalopathy of other causes. However, EEG can effects of brain injury.70 The exact mechanism of this
help in excluding non- convulsive status epilepticus, is unknown, but studies have shown that in an older
and it may help with long-term prognosis of hepatic population, the consumption of alcohol at higher levels
failure.69 MR brain imaging findings are shown in in both men and women is associated with subjective
figure 7 along with an example of MR spectroscopic and objective measures of atrophy particularly in the
changes (figure 8). frontal and temporal lobes.71 Poor nutrition is also
associated with temporal atrophy.
Box 1 Practical considerations when assessing a TREATMENT OF ALCOHOL-RELATED CNS DISEASE
patient with alcohol addiction expressing low mood The diagnosis of alcohol-related CNS disease is often
a challenging part of the management process. Treat-
► Alcohol intoxication may lead to suicidality through
ment of specific complications has been referred
disinhibition, impulsiveness and an exacerbation of
to above, but the long-term need is for prevention
depressive thoughts, most of which will resolve with
of further harm using a combination of education,
sobriety.
a good therapeutic relationship and holistic care.
► Suicide risk is significantly increased in people with
Current NICE guidelines on alcohol use disorders
alcohol dependence; it is important to enquire about
advocate an empathic and non-judgemental approach
suicidal ideation and plans.
that preserves the patient’s dignity and involves
► Depression is the most common psychiatric mental
carers.17 Initial evaluation should include assessment
illness in people with alcohol use disorder.
of alcohol-related harms to physical, mental and social
► Depressive symptoms associated with heavy
well-being and consideration of onward referral to
consumption of alcohol often resolve with abstinence.
specialist addiction services. As previously discussed,
► Addressing the alcohol addiction is an essential
structured clinical tools should be used for screening
first intervention when commencing treatment for
and for assessment of the nature and severity of
depression.
alcohol-related problems.
Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817 11
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
chosen, which does not rely as heavily on liver metabo-
Box 2 Practical considerations when reviewing
lism, such as lorazepam).
a patient with a history of alcohol use disorder
5. Manage long-term psychiatric comorbidities and neuro-
presenting with agitation and psychotic- like
logical problems, such as epilepsy
symptoms
6. Plan follow-up with addiction services and promote self-
management strategies to increase the chances of long-
► Although ‘common things are common’, do not
term abstinence or prevention of excessive consumption.
automatically assume that the presentation relates to
7. Attend to the social context and to the carer’s needs.
alcohol.
Collateral history from carers can be extremely valuable
► A collateral history from a relevant other is crucial.
and should be sought.
► Is there ongoing intoxication?
► Is it due to withdrawal?
There are many practical considerations for clini-
► Have they ingested other substances? (this is
cians managing patients presenting with disturbances
common). of cognition, mood and behaviour in the context of
► Have they sustained a head injury which is
problematic alcohol use (see boxes 1–3). It is essential
contributing to the confusion? to have an holistic approach to history-taking, exam-
► Consider previous history of mental illness including
ination and risk assessment.
psychosis. However, the long-term case management of people
► Consider capacity to consent to treatment.
with alcohol use disorders relies on understanding
the relationship between alcohol and the individual,
as people use alcohol for various purposes, including
The principles of management of alcohol-related managing mental distress and psychological trauma.
CNS disease should address the direct and indirect It is important to develop a therapeutic alliance to
toxicity of alcohol. encourage engagement with appropriate services,
1. Avoid—or at least minimise—further exposure to alco- particularly as those with alcohol use disorders are hesi-
hol and its attendant lifestyle risks. tant to engage in supports due to stigma and discrim-
2. Replace nutrients: prophylactic thiamine should be of- ination. Alcohol brief interventions are an important
Protected by copyright.
fered to those at risk of Wernicke’s due to malnutrition, tool to encourage and promote behavioural changes
alcohol dependence or risk of withdrawal. For those with in alcohol consumption, with significant outcomes.72
Wernicke’s, parenteral thiamine should continue for at
least 5 days, although as described above, in some situa-
tions, patients require treatment for much longer. Case 1 – Alcohol-related brain damage and traumatic
3. Treat acute paroxysmal symptoms, such as seizures. brain injury
4. Manage and prevent withdrawal using benzodiazepines
A 55- year-old man was admitted to hospital after a
(usually chlordiazepoxide or diazepam unless there is liv-
witnessed seizure and was later referred to liaison psychi-
er impairment, in which case an alternative should be
atry due to 4 weeks of protracted delirium. He had a
history of alcohol dependence with previous inpatient
Box 3 Prolonged confusion in someone with alcohol alcohol detoxification when abroad and a right subdural
dependence in the general hospital—practical haematoma 3 months before. He initially required low-
considerations dose antipsychotic medication for agitation.
After the delirium had resolved, he still had cognitive
► Consider other common comorbid pathologies that deficits. During this time, he drank alcohol when not on
might prolong delirium, for example, cerebrovascular the ward, and staff reported a regression of skills in activi-
disease, previous brain injury. ties of daily living, declining mood, and expressing suicidal
► It is very unusual to see a clear-cut case of Korsakoff’s ideation. He underwent inpatient functional occupational
or Wernicke’s: mixed presentations are much more therapy. Cognitive assessment identified persistent diffi-
likely and tend to take longer to resolve. culties with executive dysfunction and safety awareness
► Find out about/establish premorbid cognitive baseline and he was transferred to the neurorehabilitation unit
(often the person’s cognitive function was already under detention. One week later, he was participating well
impaired). in activities on the unit but still had very poor insight and
► Review the medication regimen; for example, felt he was suitable for rapid discharge.
benzodiazepines withdrawn too quickly or medication Conclusion
contributing to confusion (eg, opioids). This case demonstrates the complexity of treating
► Be aware that recovery with reasonable cognitive comorbid alcohol- related brain damage and traumatic
function can still occur after weeks of confusion/ brain injury, which requires a multidisciplinary approach,
delirium. thoughtful and holistic assessment, and in this case, use of
► Consider the need for incapacity or mental health act incapacity and mental health legislation to allow inpatient
legislation. assessment and rehabilitation.
12 Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
Case 2 – Wernicke’s encephalopathy Further reading
A 62-year-old man with a history of alcohol dependence ► WHO (2018) Alcohol. Available at: https://www.who.
and alcoholic cirrhosis was admitted to hospital from int/news-room/fact-sheets/detail/alcohol (Accessed: 11
his own home. He had phoned emergency services in a February 2022).
panicked state to say that he was locked in a house he ► Billingham, R., Collins, M. and Germain, J. (1996) ‘Ray’s
didn’t know. a laugh’. (Out of print but viewable at https://www.
His family knew that he had been drinking around two youtube.com/watch?v=3_T_AKPfVdI)
bottles of vodka per day for at least 2 years. His walking was ► SIGN (2019) SIGN 156: Children and young people
very poor, and he had several falls at home, and eventually exposed prenatally to alcohol. Available at: https://
had been restricted to sleeping downstairs and unable to www.sign.ac.uk/our-guidelines/children-and-young-
leave the house. He had stopped drinking suddenly without people-exposed-prenatally-to-alcohol/ (Accessed: 10
explanation around 6 weeks before admission. Two weeks December 2021).
before admission, he had developed problems with daily ► Nutt, D. et al. (2021) ‘Alcohol and the Brain’, Nutrients
functioning, for example, confusing the microwave for the 2021, Vol. 13, Page 3938, 13(11), p. 3938. doi:
cooker, and could not work out how to use the TV remote 10.3390/NU13113938
control. He also started having problems with his memory,
commenting to family that his children looked too old, and
at times believing that he still lived with his parents. Key points
On initial presentation, he was irritable, easily distracted,
and disorientated. His speech was tangential, with confab- ► Alcohol misuse appears to be increasing, with
ulation. He was treated with Pabrinex and low doses of increasing rates of its neurological sequelae.
haloperidol for agitation. Initial bloods were unremarkable. ► Identifying specific alcohol-related neurological
CT scan of brain showed bilateral periventricular hypoat- syndromes can help to target treatments and
tenuation and low attenuation foci in the basal ganglia. prevention.
After a few weeks, his disorientation and agitation ► The clinical assessment of alcohol use and its
Protected by copyright.
improved, but with some persisting cognitive problems. complications is an important clinical skill.
A kitchen assessment reported problems with sequencing ► Imaging is important in assessing the degree of
tasks, poor safety awareness, and requirement for frequent complications of acute and chronic alcohol use.
prompting. An Addenbrookes Cognitive Examination iden- ► Treatment can reverse the acute and chronic effects of
tified poor memory and fluency. The patient was keen to alcohol ingestion.
engage with a programme of rehabilitation for alcohol- ► A multidisciplinary and holistic approach can help
related brain injury and to remain abstinent from alcohol, in managing alcohol-related harms to the central
and after several months, was transferred to an supported nervous system.
accommodation rehabiliation facility.
may be exacerbated or triggered by alcohol’s direct
Simply encouraging individuals to reduce and stop and indirect effects. An holistic approach to an indi-
drinking in isolation may expose underlying difficul- vidual’s relationship with alcohol is most likely to
ties and lead to relapse, without further support in produce meaningful outcomes.
place.
With appropriate support, individuals may engage in Twitter Arun Menon @drarunmenon and John-Paul Leach @
specialist addiction services, where other interventions jpleach246
may be available, including regular case management, Collaborators Not applicable.
access to alcohol protective medications including Contributors J-PL and MW wrote first draft. MW provided
acamprosate, disulfiram and naltrexone, mental health composite case histories MO and AM helped edit subsequent
drafts NEF sourced imaging and provided expert commentary.
supports, occupational therapy, dietetics, physio-
therapy, access to recovery communities and support Funding The authors have not declared a specific grant for this
research from any funding agency in the public, commercial or
groups and residential rehabilitation. not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not applicable.
CONCLUSION
Ethics approval Not applicable.
The increasing incidence of harm related to alcohol
Provenance and peer review Commissioned. Externally peer
across society should prompt us to remain vigilant reviewed by Joanna Lovett, Southampton, UK and Martin
to its possibility in a range of patients. The potential Sadler, Plymouth, UK.
for reversibility of CNS effects makes this especially Data availability statement No data are available.
worthwhile. Modifying alcohol intake may help the Supplemental material This content has been supplied by the
management of other neuropsychiatric conditions that author(s). It has not been vetted by BMJ Publishing Group
Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817 13
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
Limited (BMJ) and may not have been peer-reviewed. Any 17 NICE. Overview | alcohol-use disorders: diagnosis, assessment
opinions or recommendations discussed are solely those of and management of harmful drinking (high-risk drinking) and
the author(s) and are not endorsed by BMJ. BMJ disclaims alcohol dependence | guidance. Available: https://www.nice.
all liability and responsibility arising from any reliance placed
on the content. Where the content includes any translated org.uk/guidance/cg115 [Accessed 03 Jun 2022].
material, BMJ does not warrant the accuracy and reliability of 18 AUDIT: the alcohol use disorders identification test: guidelines
the translations (including but not limited to local regulations, for use in primary health care. Available: https://www.who.
clinical guidelines, terminology, drug names and drug dosages), int/publications/i/item/audit-the-alcohol-use-disorders-
and is not responsible for any error and/or omissions arising identification-test-guidelines-for-use-in-primary-health-care
from translation and adaptation or otherwise.
[Accessed 03 Jun 2022].
ORCID iD 19 Bradley KA, Bush KR, McDonell MB, et al. Screening for
John-Paul Leach http://orcid.org/0000-0003-2086-9937 problem drinking: comparison of CAGE and AUDIT. J Gen
Intern Med 1998;13:379–88.
20 Bush K, Kivlahan DR, McDonell MB, et al. The AUDIT
REFERENCES alcohol consumption questions (AUDIT-C): an effective
1 WHO. Alcohol; 2018. Available: https://www.who.int/news- brief screening test for problem drinking. Arch Intern Med
room/fact-sheets/detail/alcohol [Accessed 11 Feb 2022]. 1998;13:379–89.
2 IAS. Splitting the bill: alcohol’s impact on the economy an 21 Madhubala V, Subhashree AR, Shanthi B. Serum carbohydrate
Institute of alcohol studies report; 2017. Available: www.ias. deficient transferrin as A sensitive marker in diagnosing
org.uk@InstAlcStud [Accessed 11 Feb 2022]. alcohol abuse: a case – control study. J Clin Diagn Res
3 Carhart-Harris RL, Nutt DJ. Experienced drug users assess the 2013;7:197–200.
relative harms and benefits of drugs: a web-based survey. 22 Welch KA. Neurological complications of alcohol and misuse
J Psychoactive Drugs 2013;45:322–8. of drugs. Pract Neurol 2011;11:206–19.
4 NHS Digital. Statistics on alcohol, England. 2020. Available: 23 Rose ME, Grant JE. Alcohol-induced blackout phenomenology,
https://digital.nhs.uk/data-and-information/publications/ biological basis, and gender differences. J Addict Med
statistical/statistics-on-alcohol/2020 [Accessed 11 Feb 2022]. 2010;4:61–73.
5 Green MA, Strong M, Conway L, et al. Trends in alcohol- 24 Hermens DF, Lagopoulos J. Binge drinking and the young
related admissions to hospital by age, sex and socioeconomic brain: a mini review of the Neurobiological underpinnings of
deprivation in England, 2002/03 to 2013/14. BMC Public alcohol-induced blackout. Front Psychol 2018;9:12.
Protected by copyright.
Health 2017;17:412. 25 Hillbom M, Pieninkeroinen I, Leone M, et al. Seizures in
6 Alcohol Education Trust. Facts & figures - alcohol education alcohol-dependent patients. CNS Drugs 2003;17:1013–30.
trust. 2022. Available: https://alcoholeducationtrust.org/ 26 Grover S, Ghosh A. Delirium tremens: assessment and
teacher-area/facts-figures/ [Accessed 11 Feb 2022]. management. J Clin Exp Hepatol 2018;8:460–70.
7 Public Health England. Alcohol consumption and harm during 27 Kafle P, Mandal AK, Shrestha B, et al. Twenty-eight-day-
the COVID-19 pandemic - GOV.UK. 2021. Available: https:// long delirium tremens. J Investig Med High Impact Case Rep
www.gov.uk/government/publications/alcohol-consumption- 2019;7:2324709619847228.
and-harm-during-the-covid-19-pandemic [Accessed 11 Feb 28 Reber E, Friedli N, Vasiloglou MF, et al. Management
2022]. of refeeding syndrome in medical inpatients. J Clin Med
8 Holmes J, Angus C. Alcohol deaths rise sharply in England and 2019;8:2202.
Wales. BMJ 2021;372:607. 29 Manning S, Gilmour M, Weatherall M, et al. Refeeding
9 Petrakis IL, Gonzalez G, Rosenheck R, et al. Comorbidity of syndrome is uncommon in alcoholics admitted to a hospital
alcoholism and psychiatric disorders: an overview. Alcohol Res detoxification unit. Intern Med J 2014;44:512–4.
Heal 2002;26:81. 30 Fernández-Torre JL, Kaplan PW. Subacute encephalopathy
10 Billingham R, Collins M, Germain J. Ray’s a laugh. (out of with seizures in alcoholics (SESA syndrome) revisited. Seizure
print but Viewable). 1996. Available: https://www.youtube. 2014;23:393–6.
com/watch?v=3_T_AKPfVdI 31 Abbasi H, Leach JP. Refractory status epilepticus in adults
11 Loeber S, Duka T, Welzel Márquez H, et al. Effects of repeated admitted to ITU in Glasgow 1995-2013 a longitudinal audit
withdrawal from alcohol on recovery of cognitive impairment highlighting the need for action for provoked and unprovoked
under abstinence and rate of relapse. Alcohol Alcohol status epilepticus. Seizure 2019;65:138–43.
2010;45:541–7. 32 Jordaan GP, Emsley R. Alcohol-induced psychotic disorder: a
12 Vonghia L, Leggio L, Ferrulli A, et al. Acute alcohol review. Metab Brain Dis 2014;29:231–43.
intoxication. Eur J Intern Med 2008;19:561–7. 33 Perälä J, Kuoppasalmi K, Pirkola S, et al. Alcohol-induced
13 Nutt D, Hayes A, Fonville L, et al. Alcohol and the brain. psychotic disorder and delirium in the general population. Br J
Nutrients 2021;13:3938. Psychiatry 2010;197:200–6.
14 WHO. ICD-11 for mortality and morbidity statistics. 2021. 34 Glass IB. Alcoholic Hallucinosis: a psychiatric Enigma–1. The
Available: https://icd.who.int/browse11/l-m/en#/http://id.who. development of an idea. Br J Addict 1989;84:29–41.
int/icd/entity/769299330 [Accessed 17 Jan 2022]. 35 Narasimha VL, Patley R, Shukla L, et al. Phenomenology and
15 DVLA. Assessing fitness to drive: a guide for medical course of alcoholic Hallucinosis. J Dual Diagn 2019;15:172–6.
professionals - GOV.UK. 2021. Available: https://www.gov.uk/ 36 Rao R, Topiwala A. Alcohol use disorders and the brain.
government/publications/assessing-fitness-to-drive-a-guide-for- Addiction 2020;115:1580–9.
medical-professionals [Accessed 11 Feb 2022]. 37 Mental Welfare Commission. Alcohol-related brain damage -
16 NHS. The risks of drinking too much. Available: https://www. new guide | mental welfare commission for Scotland. 2019.
nhs.uk/live-well/alcohol-advice/the-risks-of-drinking-too-much/ Available: https://www.mwcscot.org.uk/news/alcohol-related-
[Accessed 03 Jun 2022]. brain-damage-new-guide [Accessed 03 Jan 2022].
14 Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817
Review
Pract Neurol: first published as 10.1136/pn-2023-003817 on 16 June 2023. Downloaded from http://pn.bmj.com/ on June 18, 2023 at UFMG - Universidade Federal de Minas Gerais.
38 Chao R-L, Manita J. DSM-IV-TR: diagnostic and statistical CT/MRI confirmed cases. J Neurol Neurosurg Psychiatry
Manual of mental disorders. Encycl Cross-Cultural Psychol 2014;85:168–73.
2013:445–7. 57 Politis DG, Tirigay RM, Gómez PG, et al. Description of
39 Oslin DW, Cary MS. Alcohol-related dementia: validation of Interhemispheric disconnection syndrome in a patient with
diagnostic criteria. Am J Geriatr Psychiatry 2003;11:441–7. Marchiafava-Bignami disease. WJNS 2013;03:190–7.
40 Ridley NJ, Draper B, Withall A. Alcohol-related dementia: an 58 Heinrich A, Runge U, Khaw AV. Clinicoradiologic subtypes of
update of the evidence. Alzheimers Res Ther 2013;5:3. Marchiafava-Bignami disease. J Neurol 2004;251:1050–9.
41 Heirene R, John B, Roderique-Davies G. Identification and 59 Abbott R, Silber E, Felber J, et al. Osmotic demyelination
evaluation of neuropsychological tools used in the assessment syndrome. BMJ 2005;331:829–30.
of alcohol-related cognitive impairment: a systematic review. 60 Lv X, Hong Q, Lin X, et al. Osmotic demyelination
Front Psychol 2018;9:2618. syndrome: clinical, neuroimaging characteristics,
42 Zahr NM, Kaufman KL, Harper CG. Clinical and pathological and outcomes in a series of 18 cases. Biomed Res Int
features of alcohol-related brain damage. Nat Rev Neurol 2021;2021:9944632.
2011;7:284–94. 61 Razvi SSM, Leach JP. Asymptomatic pontine Myelinolysis. Eur
43 Carlen PL, Wilkinson DA. Reversibility of alcohol‐related brain J Neurol 2006;13:1261–3.
damage: clinical and experimental observations. Acta Med 62 Guerri C, Bazinet A, Riley EP. Foetal alcohol spectrum
Scand 1987;221:19–26. disorders and alterations in brain and behaviour. Alcohol
44 Harper C. The neuropathology of alcohol-related brain Alcohol 2009;44:108–14.
damage. Alcohol Alcohol 2009;44:136–40. 63 SIGN. SIGN 156: children and young people exposed
45 Donnino MW, Vega J, Miller J, et al. Myths and prenatally to alcohol. 2019. Available: https://www.sign.ac.uk/
misconceptions of Wernicke’s encephalopathy: what our-guidelines/children-and-young-people-exposed-prenatally-
every emergency physician should know. Ann Emerg Med to-alcohol/ [Accessed 10 Dec 2021].
2007;50:715–21. 64 Chandran S, Sreeraj VS, Venkatasubramanian G,
46 Caine D, Halliday GM, Kril JJ, et al. Operational criteria et al. Corpus callosum Morphometry in children with
for the classification of chronic alcoholics: identification of prenatal alcohol exposure. Psychiatry Res Neuroimaging
Wernicke’s encephalopathy. J Neurol Neurosurg Psychiatry 2021;318:111405.
1997;62:51–60. 65 Schölin L, Mukherjee RAS, Aiton N, et al. Fetal alcohol
47 Nishimoto A, Usery J, Winton JC, et al. High-dose parenteral spectrum disorders: an overview of current evidence and
Protected by copyright.
thiamine in treatment of Wernicke's encephalopathy: case activities in the UK. Arch Dis Child 2021;106:636–40.
series and review of the literature. In Vivo 2017;31:121–4. 66 Office for National Statistics. Drug misuse in England and
48 NICE. BNF: British National Formulary. Br Natl Formul, Wales. 2020. Available: https://www.ons.gov.uk/peoplepopula
2022. tionandcommunity/crimeandjustice/articles/drugmisuseinengl
49 RCPsych. Alcohol and brain damage in adults with reference andandwales/yearendingmarch2020#overall-trends-in-drug-
to high-risk groups. 2014. Available: http://www.rcpsych.ac.uk/ misuse [Accessed 11 Feb 2022].
publications/collegereports.aspx [Accessed 03 Jan 2022]. 67 Leach JP, Mohanraj R, Borland W. Alcohol and drugs in
50 Arts NJM, Walvoort SJW, Kessels RPC. Korsakoff ’s syndrome: epilepsy: pathophysiology, presentation, possibilities, and
a critical review. Neuropsychiatr Dis Treat 2017;13:2875–90. prevention. Epilepsia 2012;53 Suppl 4:48–57.
51 Sacks O. The man who mistook his wife for a hat. 2011: 257. 68 Kandiah PA, Kumar G. Hepatic encephalopathy—the old and
52 Schwarzinger M, Pollock BG, Hasan OSM, et al. Contribution the new. Crit Care Clin 2016;32:311–29.
of alcohol use disorders to the burden of dementia in France 69 Koul R, Maiwall R, Ramalingam A, et al. Role of EEG in
2008–13: a nationwide retrospective cohort study. Lancet predicting outcome of hepatic encephalopathy patients.
Public Health 2018;3:e124–32. Neurodiagn J 2020;60:272–88.
53 Gu Y, Scarmeas N, Short EE, et al. Alcohol intake and 70 Anstey KJ, Jorm AF, Réglade-Meslin C, et al. Weekly alcohol
brain structure in a multiethnic elderly cohort. Clin Nutr consumption, brain atrophy, and white matter Hyperintensities
2014;33:662–7. in a community-based sample aged 60 to 64 years. Psychosom
54 Immonen S, Launes J, Järvinen I, et al. Moderate alcohol use is Med 2006;68:778–85.
associated with decreased brain volume in early middle age in 71 Verhaar BJH, de Leeuw FA, Doorduijn AS, et al. Nutritional
both sexes. Sci Rep 2020;10:1–8. status and structural brain changes in Alzheimer’s disease: the
55 Mitoma H, Manto M, Shaikh AG. Mechanisms of ethanol- NUDAD project. Alzheimers Dement (Amst) 2020;12:e12063.
induced cerebellar ataxia: underpinnings of neuronal death in 72 World Health Organization. Evidence for the effectiveness and
the cerebellum. Int J Environ Res Public Health 2021;18:8678. cost-effectiveness of interventions to reduce alcohol-related
56 Hillbom M, Saloheimo P, Fujioka S, et al. Diagnosis and harm. 2009. Available: https://apps.who.int/iris/handle/10665/
management of Marchiafava–Bignami disease: a review of 107269 [Accessed 06 Jul 2022].
Wolfe M, et al. Pract Neurol 2023;0:1–15. doi:10.1136/pn-2023-003817 15
You might also like
- Focused Exam - Depression - Completed - Shadow HealthDocument5 pagesFocused Exam - Depression - Completed - Shadow Healthjenyoilig100% (6)
- Honey and Cinnamon Cures PDFDocument5 pagesHoney and Cinnamon Cures PDFniranjan_meharNo ratings yet
- Alcohol and Drugs in Epilepsy: Pathophysiology, Presentation, Possibilities, and PreventionDocument10 pagesAlcohol and Drugs in Epilepsy: Pathophysiology, Presentation, Possibilities, and PreventionAna Maria Gómez GonzálezNo ratings yet
- STAD211ECE B2 AlcoholAbuseDocument14 pagesSTAD211ECE B2 AlcoholAbuseAlfredo MorenoNo ratings yet
- Newer Plant Based Drug Molecules With Theraputic Potential To Combat Alcohol DependencyDocument4 pagesNewer Plant Based Drug Molecules With Theraputic Potential To Combat Alcohol DependencyvickyNo ratings yet
- Correspondence: Alcohol Use and Misuse During The COVID-19 Pandemic: A Potential Public Health Crisis?Document1 pageCorrespondence: Alcohol Use and Misuse During The COVID-19 Pandemic: A Potential Public Health Crisis?David Adolfo Paez MolinaNo ratings yet
- Saah 2004 PDFDocument7 pagesSaah 2004 PDFIno MoxoNo ratings yet
- The Effect of Alcohol and Nicotine Abuse On Gene Expression in The BrainDocument15 pagesThe Effect of Alcohol and Nicotine Abuse On Gene Expression in The BrainJoão MaiaNo ratings yet
- The Neurobiology of AddictionDocument24 pagesThe Neurobiology of AddictionErnesto Jaramillo ValenzuelaNo ratings yet
- Effects of Drinking On Late-Life Brain and Cognition: Anya Topiwala, Klaus Peter EbmeierDocument5 pagesEffects of Drinking On Late-Life Brain and Cognition: Anya Topiwala, Klaus Peter Ebmeierfarah maulida martaNo ratings yet
- Alcohol y CerebroDocument19 pagesAlcohol y CerebromdsgdNo ratings yet
- Sistema GABA y Alcoholismo RevisionDocument19 pagesSistema GABA y Alcoholismo RevisionPsiquiatria Clinica ProyectarteNo ratings yet
- Pharmacogenetic Approaches To The Treatment of Alcohol AddictionDocument15 pagesPharmacogenetic Approaches To The Treatment of Alcohol AddictionVissente TapiaNo ratings yet
- Clinical Aspects of Alcohol and Drug AddictionDocument10 pagesClinical Aspects of Alcohol and Drug Addictional sharpNo ratings yet
- Nihms 960120Document22 pagesNihms 960120Fadli Nurul HanifNo ratings yet
- No Level of Alcohol Consumption Improves HealthDocument2 pagesNo Level of Alcohol Consumption Improves HealthMarcelo MenezesNo ratings yet
- Genetics Inheritability Factors and Addiction 2471 2663 1000143Document5 pagesGenetics Inheritability Factors and Addiction 2471 2663 1000143Anonymous QOx9XUzjNo ratings yet
- PIIS2468266720301237Document1 pagePIIS2468266720301237Milton Ricardo de Medeiros FernandesNo ratings yet
- Bja Substance Abuse in AnaesthesistDocument6 pagesBja Substance Abuse in AnaesthesistaleizaNo ratings yet
- Cardiac Complications of Common Drugs of AbuseDocument11 pagesCardiac Complications of Common Drugs of AbusemiguelalmenarezNo ratings yet
- The Impact of Alcoholic Beverages On Human HealthDocument3 pagesThe Impact of Alcoholic Beverages On Human HealthLaura NeiraNo ratings yet
- Drug Therapy: D T A DDocument9 pagesDrug Therapy: D T A DWahyu BachtiarNo ratings yet
- 36Document8 pages36Andra IrinaNo ratings yet
- Understanding Alcohol Use DisordersDocument17 pagesUnderstanding Alcohol Use DisordersNational Press FoundationNo ratings yet
- Alcohol Addiction, Gut Microbiota, and Alcoholism - ReviewDocument11 pagesAlcohol Addiction, Gut Microbiota, and Alcoholism - ReviewDeisy KesumawatiNo ratings yet
- Tubulointerstitial Injury and Drugs of AbuseDocument6 pagesTubulointerstitial Injury and Drugs of AbuseHadsfrv KajdgygNo ratings yet
- Stimulant and Designer Drug Use - AafpDocument8 pagesStimulant and Designer Drug Use - AafpRaihan HassanNo ratings yet
- Alcohol Related DisordersDocument27 pagesAlcohol Related DisordersIzzyinOzzieNo ratings yet
- AHA Statement-Cardiopulmonary Impact of E-Cigarettes and Vaping-2023Document26 pagesAHA Statement-Cardiopulmonary Impact of E-Cigarettes and Vaping-2023Walter ReyesNo ratings yet
- Drug Use in The Elderly: A Review of Problems and Special ConsiderationsDocument25 pagesDrug Use in The Elderly: A Review of Problems and Special ConsiderationsFariz AdamNo ratings yet
- Revista BiomédicaDocument13 pagesRevista BiomédicaJohana TovarNo ratings yet
- Identification and Management Acute Alcohol Intox - 2023Document8 pagesIdentification and Management Acute Alcohol Intox - 2023Choga ArlandoNo ratings yet
- Alcohol and Global Health 1: SeriesDocument11 pagesAlcohol and Global Health 1: SeriesMigs CarusoNo ratings yet
- Prescribing Medicines To Older People - How To Consider The Impact of Ageing On Human Organ and Body FunctionsDocument10 pagesPrescribing Medicines To Older People - How To Consider The Impact of Ageing On Human Organ and Body FunctionsEnzo VasquezNo ratings yet
- Nutt Study, Lancet, Harm of DrugsDocument7 pagesNutt Study, Lancet, Harm of DrugsNeil PetersonNo ratings yet
- Tratamiento de Alcohol InglesDocument11 pagesTratamiento de Alcohol InglesLit DianeNo ratings yet
- A Handbook of Mcqs in Toxicology: Muneeb U RehmanDocument53 pagesA Handbook of Mcqs in Toxicology: Muneeb U Rehmanquimicosorio100% (2)
- Alcohol Use: Annals of Internal MedicineDocument17 pagesAlcohol Use: Annals of Internal MedicinesolidchessNo ratings yet
- BMJ Open OphthalmologyDocument7 pagesBMJ Open OphthalmologySujiv AkkilaguntaNo ratings yet
- How Bad Are Illegal Drugs? - Lancet StudyDocument7 pagesHow Bad Are Illegal Drugs? - Lancet StudyJames Dwyer100% (1)
- Web 3 0 and MedicineDocument4 pagesWeb 3 0 and Medicinepradeep3112gowdaNo ratings yet
- Determinants of Mental Health and Abuse of Psychoactive Substances Associated With Tobacco Use. A Case-Control StudyDocument12 pagesDeterminants of Mental Health and Abuse of Psychoactive Substances Associated With Tobacco Use. A Case-Control Studymodesto66No ratings yet
- Farmacocinetica y Dinamia en Adultdos MayoresDocument5 pagesFarmacocinetica y Dinamia en Adultdos MayoresDIEGO FERNANDO URIBE JARAMILLONo ratings yet
- Faught Et Al-2015-British Journal of Clinical PharmacologyDocument9 pagesFaught Et Al-2015-British Journal of Clinical PharmacologyHendra Wana Nur'aminNo ratings yet
- Alcohol and CognitionDocument9 pagesAlcohol and CognitionKaren VelázquezNo ratings yet
- CEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDocument5 pagesCEACCP - Illegal Substances in Anaesthetic and Intensive Care PracticesDonkeyManNo ratings yet
- Nejmcp 2032393Document10 pagesNejmcp 2032393JEFFERSON MUÑOZNo ratings yet
- Genes and AddictionsDocument7 pagesGenes and AddictionsMihaela DumitrescuNo ratings yet
- Alcohol and The Nervous System: C Mcintosh, J ChickDocument6 pagesAlcohol and The Nervous System: C Mcintosh, J ChickSumroachNo ratings yet
- 2022 Tobacco AdictionDocument10 pages2022 Tobacco AdictionJuan jose Cacua DelgadoNo ratings yet
- Geria ToxicidadDocument9 pagesGeria ToxicidadGh RossiNo ratings yet
- The CircleDocument7 pagesThe Circleamaralmuamuene91No ratings yet
- Review of Thiamine Deficiency DisordersDocument10 pagesReview of Thiamine Deficiency DisordersAndre MattarNo ratings yet
- Addiction - 2021 - Herlinger - Opioid Use Disorder and The Brain A Clinical PerspectiveDocument11 pagesAddiction - 2021 - Herlinger - Opioid Use Disorder and The Brain A Clinical PerspectiveloloasbNo ratings yet
- Biological Substrates of Addiction 2014Document30 pagesBiological Substrates of Addiction 2014Jacky KarNo ratings yet
- Eposter Viewing2020Document307 pagesEposter Viewing2020loloasbNo ratings yet
- Who Benefits Most From The Cardioprotective Properties of Alcohol Consumption-Health Freaks or Couch Potatoes?Document4 pagesWho Benefits Most From The Cardioprotective Properties of Alcohol Consumption-Health Freaks or Couch Potatoes?Benard OyangNo ratings yet
- HHS Public Access: Neuropathology of Substance Use DisordersDocument29 pagesHHS Public Access: Neuropathology of Substance Use DisordersNathaly CantorNo ratings yet
- Continuum Abuso Sustancias 2023Document23 pagesContinuum Abuso Sustancias 2023siralkNo ratings yet
- Alcoholic/Non-Alcoholic Digestive DiseasesFrom EverandAlcoholic/Non-Alcoholic Digestive DiseasesHitoshi YoshijiNo ratings yet
- Imaging of Ischemic Heart Disease in Women: A Critical Review of the LiteratureFrom EverandImaging of Ischemic Heart Disease in Women: A Critical Review of the LiteratureNo ratings yet
- AtyícalparkinsonismDocument6 pagesAtyícalparkinsonismHenrique OliveiraNo ratings yet
- Movement Disorders - 2024 - Gan or - Genetics of Parkinson S Disease in Underrepresented Populations New Studies Pave TheDocument2 pagesMovement Disorders - 2024 - Gan or - Genetics of Parkinson S Disease in Underrepresented Populations New Studies Pave TheHenrique OliveiraNo ratings yet
- Clerico Et Al Treatment of Relapsing-Remitting Multiple Sclerosis After 24 Doses of NatalizumabDocument7 pagesClerico Et Al Treatment of Relapsing-Remitting Multiple Sclerosis After 24 Doses of NatalizumabHenrique OliveiraNo ratings yet
- Martínez-Lapiscina Et Al Natalizumab-Induced Autoimmune Hepatitis in A Patient With Multiple SclerosisDocument2 pagesMartínez-Lapiscina Et Al Natalizumab-Induced Autoimmune Hepatitis in A Patient With Multiple SclerosisHenrique OliveiraNo ratings yet
- Sustained Attention in Cranial Dystonia Patients Treated With BTDocument5 pagesSustained Attention in Cranial Dystonia Patients Treated With BTHenrique OliveiraNo ratings yet
- Cognitive Executive Function in Dystonia: Marjan Jahanshahi, John Rowe, and Rebecca FullerDocument12 pagesCognitive Executive Function in Dystonia: Marjan Jahanshahi, John Rowe, and Rebecca FullerHenrique OliveiraNo ratings yet
- Thecognitivefeaturesofidiopathicand DYT1 DystoniaDocument8 pagesThecognitivefeaturesofidiopathicand DYT1 DystoniaHenrique OliveiraNo ratings yet
- Jamaneurology Gray 2021 Oi 210082 1640103773.73219Document10 pagesJamaneurology Gray 2021 Oi 210082 1640103773.73219Henrique OliveiraNo ratings yet
- Patients With Primary Cervical Dystonia Have Evidence of Discrete Deficits in PraxisDocument24 pagesPatients With Primary Cervical Dystonia Have Evidence of Discrete Deficits in PraxisHenrique OliveiraNo ratings yet
- Parkinsonism and Related DisordersDocument4 pagesParkinsonism and Related DisordersHenrique OliveiraNo ratings yet
- Relationship of Cognitive Function To Motor Symptoms and Mood Disorders in Patients With Isolated DystoniaDocument7 pagesRelationship of Cognitive Function To Motor Symptoms and Mood Disorders in Patients With Isolated DystoniaHenrique OliveiraNo ratings yet
- Cognitive Flexibility in Primary Dystonia: Eceived Inal Evision CceptedDocument9 pagesCognitive Flexibility in Primary Dystonia: Eceived Inal Evision CceptedHenrique OliveiraNo ratings yet
- Noc120108 580 586Document7 pagesNoc120108 580 586Henrique OliveiraNo ratings yet
- Nejm 199710163371604Document7 pagesNejm 199710163371604Henrique OliveiraNo ratings yet
- Preprints202304 0108 v1Document25 pagesPreprints202304 0108 v1Henrique OliveiraNo ratings yet
- Nihms 212798Document21 pagesNihms 212798Henrique OliveiraNo ratings yet
- A Countryside For Health and Well-Being: The Physical and Mental Health Benefits of Green ExerciseDocument137 pagesA Countryside For Health and Well-Being: The Physical and Mental Health Benefits of Green Exercisecarysbriddon815No ratings yet
- Smart Baby Shield Brochure PDFDocument13 pagesSmart Baby Shield Brochure PDFPeterHengNo ratings yet
- UntitledDocument334 pagesUntitledLocalVet TunariNo ratings yet
- Notes and Assignments For Unit 1 Essentials of Diseases and ConditionsDocument5 pagesNotes and Assignments For Unit 1 Essentials of Diseases and Conditionscindyfuller68No ratings yet
- Hydrogen Hydroxide: Acid-Base Balance Overview of Acids and Bases DescriptionDocument15 pagesHydrogen Hydroxide: Acid-Base Balance Overview of Acids and Bases DescriptionElisha WorworNo ratings yet
- Respiratory NCLEX Practice Test Part 1: Guillain-Barré SyndromeDocument20 pagesRespiratory NCLEX Practice Test Part 1: Guillain-Barré SyndromeHasan A AsFour100% (2)
- Introduction To Epidemiology: The Basic Science of Public HealthDocument34 pagesIntroduction To Epidemiology: The Basic Science of Public Healthapi-19641337100% (1)
- Ashley Lemke v. Soap Korner LLCDocument14 pagesAshley Lemke v. Soap Korner LLCMichael_Lee_RobertsNo ratings yet
- Set 5, Reumatology, ArpanaDocument14 pagesSet 5, Reumatology, ArpanaSahana hadaNo ratings yet
- PhcogCommn 13 1 9Document6 pagesPhcogCommn 13 1 9Priyanka SujithNo ratings yet
- Brauchle - Elder Assessment Paper - Nur 321Document15 pagesBrauchle - Elder Assessment Paper - Nur 321api-405374041No ratings yet
- Emerging Infectious DiseasesDocument175 pagesEmerging Infectious Diseasesmani100% (2)
- My Co PlasmaDocument70 pagesMy Co Plasmatummalapalli venkateswara raoNo ratings yet
- NCS 17th June NewsletterDocument6 pagesNCS 17th June NewsletterstaffncsNo ratings yet
- Management Foreign BodyDocument6 pagesManagement Foreign BodyRahmatia SyukrinaNo ratings yet
- CIE A Level Biology - Gas ExchangeDocument14 pagesCIE A Level Biology - Gas ExchangeSaraNo ratings yet
- Case Write Up Report 5 Umbilical Hernia: SURGERY 1-2022/2023Document6 pagesCase Write Up Report 5 Umbilical Hernia: SURGERY 1-2022/2023RSNo ratings yet
- Ariana's Reasearch PaperDocument8 pagesAriana's Reasearch Paperapi-281014657No ratings yet
- YersiniaDocument13 pagesYersiniamicrobzNo ratings yet
- Polydipsia & Polyuria Tutorial, March 16,3Document45 pagesPolydipsia & Polyuria Tutorial, March 16,3Abdurazzag ShumakhiNo ratings yet
- Autistic Spectrum Disorders in Children, Pediatric Habilitation Series Volume 12 (Marcel Dekker, 2004)Document337 pagesAutistic Spectrum Disorders in Children, Pediatric Habilitation Series Volume 12 (Marcel Dekker, 2004)TOTEANU CRISTINANo ratings yet
- Unhappy Meals - Michael Pollan - The New York TimesDocument25 pagesUnhappy Meals - Michael Pollan - The New York TimesBob0% (1)
- Article-PDF-baljeet Singh Puneet Bajaj Grunam Singh-141Document3 pagesArticle-PDF-baljeet Singh Puneet Bajaj Grunam Singh-141barcimNo ratings yet
- Noort DrugDocument5 pagesNoort Drugapi-293189177No ratings yet
- Incident RatesDocument7 pagesIncident RatesSamantha Meril PandithaNo ratings yet
- Narrative Pathophysiology of Varicose VeinsDocument2 pagesNarrative Pathophysiology of Varicose VeinsKim SunooNo ratings yet
- Natural History of Disease and Infectious Disease Cycle 2Document40 pagesNatural History of Disease and Infectious Disease Cycle 2elsawzgoodNo ratings yet
- PDF 20221127 181837 0000Document16 pagesPDF 20221127 181837 0000Lowella Rose C. DonguinesNo ratings yet