Download as pdf or txt
You might also like
- ACTION Personal Trainer Certification Textbook v2Document334 pagesACTION Personal Trainer Certification Textbook v2dreamsheikh100% (12)
- All Knowmedge Internal Medicine FlashcardDocument22 pagesAll Knowmedge Internal Medicine Flashcardrub100% (4)
- Non Viral HepatitisDocument40 pagesNon Viral Hepatitisostaz2000100% (1)
- Addison Disease: Diagnosis and Initial ManagementDocument4 pagesAddison Disease: Diagnosis and Initial ManagementTeguh RahNo ratings yet
- Mental Health-Questions Updated 012005Document9 pagesMental Health-Questions Updated 012005Ramon Carlo AlmiranezNo ratings yet
- Adrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal MedicineDocument24 pagesAdrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal Medicineraed faisalNo ratings yet
- Parathyroid DisordersDocument44 pagesParathyroid DisordersBIAN ALKHAZMARI100% (1)
- Causes of Diffuse Hyperpigmentation EndocrinopathiesDocument9 pagesCauses of Diffuse Hyperpigmentation EndocrinopathiesAbdul QuyyumNo ratings yet
- Vetcpd Adrenal Disease Notes Christopher Scudder BVSC (Dist) Mvetmed (Dist) PHD Dipacvim Mrcvs Christopher - Scudder@Southfields - Co.UkDocument21 pagesVetcpd Adrenal Disease Notes Christopher Scudder BVSC (Dist) Mvetmed (Dist) PHD Dipacvim Mrcvs Christopher - Scudder@Southfields - Co.UkStefana UrsuNo ratings yet
- Clinical Immunology 6-11-2022: Immunological Diseases of The Endocrine SystemDocument30 pagesClinical Immunology 6-11-2022: Immunological Diseases of The Endocrine Systemphoto copyhemnNo ratings yet
- The Parathyroid Gland: DR - Umalkhayr Omar, MDDocument36 pagesThe Parathyroid Gland: DR - Umalkhayr Omar, MDgibreilNo ratings yet
- Thyroiditis and Parathyroid GlandDocument29 pagesThyroiditis and Parathyroid GlandTheoder RobinsonNo ratings yet
- MRCPass Notes For MRCP 1 - EnDOCRINOLOGYDocument12 pagesMRCPass Notes For MRCP 1 - EnDOCRINOLOGYsabdali100% (1)
- Abnormal Clinical Chemistry & TDM in CancerDocument44 pagesAbnormal Clinical Chemistry & TDM in CancerkinjalkaNo ratings yet
- Your Online Nursing Notes : Addison'S Disease Basic InfoDocument4 pagesYour Online Nursing Notes : Addison'S Disease Basic InfoseigelysticNo ratings yet
- Endocrinology NotesDocument12 pagesEndocrinology Notesrandiey john abelleraNo ratings yet
- Stunted Growth: Addison DiseaseDocument32 pagesStunted Growth: Addison DiseaseAshim AbhiNo ratings yet
- AddisonsdiseaseDocument5 pagesAddisonsdiseasenessimmounir1173No ratings yet
- Summary of Medical EmergenciesDocument24 pagesSummary of Medical Emergenciesbasharswork99No ratings yet
- Addison Disease: Diagnosis and Initial ManagementDocument5 pagesAddison Disease: Diagnosis and Initial ManagementI Gede SubagiaNo ratings yet
- Pathology of Common Glomerular Syndromes: DR Purushotham KrishnappaDocument34 pagesPathology of Common Glomerular Syndromes: DR Purushotham KrishnappaTarin IslamNo ratings yet
- Adrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing SyndromeDocument46 pagesAdrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing Syndromeyuyu tuptupNo ratings yet
- Adrenal Insufficiency.Document17 pagesAdrenal Insufficiency.Hala AhmadNo ratings yet
- Thyrotoxicosis: By: DR Mukesh Kumar Samota PG (M.D. Medicine) Medical College Jhalawar (RajasthanDocument40 pagesThyrotoxicosis: By: DR Mukesh Kumar Samota PG (M.D. Medicine) Medical College Jhalawar (RajasthanShravani ShagapuramNo ratings yet
- Adrenal Insufficiency and Cushing's Disease-1Document34 pagesAdrenal Insufficiency and Cushing's Disease-1Mwanja MosesNo ratings yet
- Chronic Liver DiseasesDocument24 pagesChronic Liver DiseasestabarekNo ratings yet
- Grand Round Case Presentation: by DR Sanjay Khare MD MedicineDocument19 pagesGrand Round Case Presentation: by DR Sanjay Khare MD MedicineHrishikeshNo ratings yet
- Parathyroid DiseaseDocument10 pagesParathyroid Diseasemohammedghassan53No ratings yet
- Primary HyperparathyroidismDocument13 pagesPrimary Hyperparathyroidismqayyum consultantfpscNo ratings yet
- Addison's DseDocument9 pagesAddison's DseKath RubioNo ratings yet
- Primary and Secondary HyperparathyroidismDocument13 pagesPrimary and Secondary Hyperparathyroidismaileen agustinNo ratings yet
- Hypocalcemia: Author: Christopher B Beach, MD, FACEP, FAAEM, Associate Professor and ViceDocument65 pagesHypocalcemia: Author: Christopher B Beach, MD, FACEP, FAAEM, Associate Professor and ViceronelnNo ratings yet
- Adrenal Insufficiency & Adrenal Crisis: Emergency Medicine CH 217Document30 pagesAdrenal Insufficiency & Adrenal Crisis: Emergency Medicine CH 217Saroj Kanta SahuNo ratings yet
- 20 Endocrine Disease and AnaesthesiaDocument0 pages20 Endocrine Disease and AnaesthesiajuniorebindaNo ratings yet
- Addison's DiseaseDocument3 pagesAddison's Diseaseavinash dhameriyaNo ratings yet
- Adrenocortical DisordersDocument73 pagesAdrenocortical DisordersReunita ConstantiaNo ratings yet
- Nephrology: Omar K MRCP IrelandDocument54 pagesNephrology: Omar K MRCP IrelandManmeet SNo ratings yet
- אלון קלציום חלק 3Document25 pagesאלון קלציום חלק 3Alon GoldfainerNo ratings yet
- Hemolytic Uremic Syndrome: Prof. Pediatric Nephrology Sindh Institute of Urology & Transplanatation PakistanDocument111 pagesHemolytic Uremic Syndrome: Prof. Pediatric Nephrology Sindh Institute of Urology & Transplanatation PakistanDr. Mir Uzair HashmiNo ratings yet
- Nephrotic SyndromeDocument28 pagesNephrotic SyndromeJohn chrisant Mwansa the future presdoNo ratings yet
- Hyper para Thyroid Is MDocument3 pagesHyper para Thyroid Is MAriefNo ratings yet
- 21 CP Endocrine 2Document73 pages21 CP Endocrine 2Aman Singh RaoNo ratings yet
- Pembahasan UKDI CLINIC 3 Batch Mei 2016Document662 pagesPembahasan UKDI CLINIC 3 Batch Mei 2016widi kusumaNo ratings yet
- 2 - Parathyroid GlandDocument21 pages2 - Parathyroid Glandtaha55860No ratings yet
- Sle 1Document36 pagesSle 1Votey CHNo ratings yet
- Clinical and Biochemical Spectrum of Hypokalemic Paralysis in NorthDocument9 pagesClinical and Biochemical Spectrum of Hypokalemic Paralysis in NorthMelanton Ifan Fernando RajagukgukNo ratings yet
- Lec#49 Calcium DisordersDocument105 pagesLec#49 Calcium DisordersKhaldoun AlmomaniNo ratings yet
- Addison Diseases LecDocument40 pagesAddison Diseases LecSalman RabbaniNo ratings yet
- Note For H.Pylori Antigen TestDocument12 pagesNote For H.Pylori Antigen TestKrishna ShresthaNo ratings yet
- LithiumDocument4 pagesLithiumapi-3797941100% (1)
- Practice: Investigating Hyperkalaemia in AdultsDocument6 pagesPractice: Investigating Hyperkalaemia in AdultsJbarrianNo ratings yet
- Endocrine SystemDocument59 pagesEndocrine Systemayesharajput5110No ratings yet
- Adrenal DisordersDocument36 pagesAdrenal DisordersMalueth AnguiNo ratings yet
- Reye'S Syndrome: Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocument7 pagesReye'S Syndrome: Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreeNo ratings yet
- Adrenal InsufficiencyDocument2 pagesAdrenal InsufficiencyTracy NwanneNo ratings yet
- Addisons DiseaseDocument14 pagesAddisons DiseaseJils SureshNo ratings yet
- Gds137 Slide HyperthyroidismDocument30 pagesGds137 Slide HyperthyroidismLouie Kem Anthony BabaranNo ratings yet
- Parathyroid Gland and Other Endocrine GlandsDocument35 pagesParathyroid Gland and Other Endocrine GlandsDrRahma Ali HeissNo ratings yet
- Hypokalemia Disease AmnaDocument5 pagesHypokalemia Disease AmnaIzhar AhmadNo ratings yet
- Pituitary &thyroid NotesDocument7 pagesPituitary &thyroid NotesAli salimNo ratings yet
- Systemic Lupus ErythematosusDocument37 pagesSystemic Lupus ErythematosusFirman Ichlasul AmalNo ratings yet
- NCM 106 FinalsDocument55 pagesNCM 106 FinalsKyle BagacNo ratings yet
- Th1/Th2 Dominance Symptoms ListDocument3 pagesTh1/Th2 Dominance Symptoms ListXemantic100% (1)
- PendragonDocument8 pagesPendragonAllen Peter WeixlerNo ratings yet
- Dr. Bhatia Medical Coaching Institution Hyderabad Bio-Chemistry - 2Document5 pagesDr. Bhatia Medical Coaching Institution Hyderabad Bio-Chemistry - 2PNo ratings yet
- A Guide To Children's Palliative CareDocument21 pagesA Guide To Children's Palliative CareAndrés JiménezNo ratings yet
- How-To-Cope-With-Hearing-Voices 2016Document22 pagesHow-To-Cope-With-Hearing-Voices 2016api-247002951No ratings yet
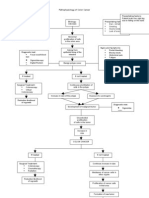
- Pa Tho Physiology of Colon CancerDocument2 pagesPa Tho Physiology of Colon Cancernick_nock0893% (14)
- HemostazaDocument7 pagesHemostazaMischa VlăsceanuNo ratings yet
- Exercise1 - Valencia Yoanna - 205090307111012Document3 pagesExercise1 - Valencia Yoanna - 205090307111012Valencia YoannaNo ratings yet
- Hiv AidsDocument41 pagesHiv AidsNela Rosa Harianja100% (1)
- Elise Freel ResumeDocument2 pagesElise Freel Resumeapi-676601982No ratings yet
- Medication: Expected Pharmacological Action Therapeutic UseDocument1 pageMedication: Expected Pharmacological Action Therapeutic UseMike EveretteNo ratings yet
- Tcc501 720 Nutritionclaims En-UsDocument16 pagesTcc501 720 Nutritionclaims En-UsMichael BradfordNo ratings yet
- Vertigo MeniereDocument5 pagesVertigo MeniereHamba AllahNo ratings yet
- Chitoglucan New OverviewDocument6 pagesChitoglucan New OverviewmjmorcelliNo ratings yet
- Post Op Alveoloplasty - RRR - 1 PDFDocument1 pagePost Op Alveoloplasty - RRR - 1 PDFAndykaYayanSetiawanNo ratings yet
- Vasculitis SyndromesDocument9 pagesVasculitis Syndromesapi-3704562No ratings yet
- Pub1566 WebDocument124 pagesPub1566 WebRadoi Sandina RodicaNo ratings yet
- Qs 221021 MCQ Part 1 November 2021Document4 pagesQs 221021 MCQ Part 1 November 2021dayahjarisNo ratings yet
- Myasthenia GravisDocument3 pagesMyasthenia Gravisapi-3822433100% (2)
- Document PDFDocument18 pagesDocument PDFlilisNo ratings yet
- Q1/ Choose The Most Appropriate AnswerDocument11 pagesQ1/ Choose The Most Appropriate AnswerzainabNo ratings yet
- Eye ExerciseDocument3 pagesEye ExerciseBrylePeters DCSNo ratings yet
- Andrew Wakefield (2009) Response To Dr. Ari Brown and The Immunization Action CoalitionDocument18 pagesAndrew Wakefield (2009) Response To Dr. Ari Brown and The Immunization Action CoalitionEMFsafety100% (2)
- Hemophilia PPT 4th PeriodDocument12 pagesHemophilia PPT 4th PeriodNasser AlqahtaniNo ratings yet
- Positioning of The Patient For Abdominal ExaminationDocument8 pagesPositioning of The Patient For Abdominal ExaminationDoctor Saleem RehmanNo ratings yet
- Ventilator Bundle (IHI Tool) : Submitted By: Institute For Healthcare ImprovementDocument12 pagesVentilator Bundle (IHI Tool) : Submitted By: Institute For Healthcare ImprovementYamto TlNo ratings yet
- Mycology Board Review Presentation10Document54 pagesMycology Board Review Presentation10Foysal SirazeeNo ratings yet