Download as pdf or txt
You might also like
- DPWH PDM PiceDocument55 pagesDPWH PDM Picemmabee100% (4)
- Esg Policy TemplateDocument13 pagesEsg Policy Templatemanish026No ratings yet
- 00 - HUAWEI - Training IntroductionDocument27 pages00 - HUAWEI - Training IntroductionSav SashaNo ratings yet
- CS Form No. 34 A Plantilla of Casual Appointment Regulated CTDDocument2 pagesCS Form No. 34 A Plantilla of Casual Appointment Regulated CTDMaria Theresa Dolores100% (4)
- Workday Interviews Q & ADocument155 pagesWorkday Interviews Q & AMahesh Chikoti56% (9)
- Application Form Community Officer 2023Document6 pagesApplication Form Community Officer 2023Mariana CobzacNo ratings yet
- For Instructions - See Sack of Form DR-1Document1 pageFor Instructions - See Sack of Form DR-1Zach EdwardsNo ratings yet
- Shams Onboarding Form Direct ClientDocument9 pagesShams Onboarding Form Direct ClientDany QasasNo ratings yet
- Enclosed: Latest CV: Application FormatDocument3 pagesEnclosed: Latest CV: Application FormatNavaneetha LakshmanNo ratings yet
- Application Registration 350 Research Grants enDocument3 pagesApplication Registration 350 Research Grants enPatrick Tejada AdriazolaNo ratings yet
- Sales Associate ApplicationDocument2 pagesSales Associate ApplicationRamiro LopezNo ratings yet
- Sales PDFDocument2 pagesSales PDFRamiro LopezNo ratings yet
- Confidential: Joining FormDocument4 pagesConfidential: Joining Formavinash raoNo ratings yet
- Application Form - Caribarang - IdDocument4 pagesApplication Form - Caribarang - IdtuginoNo ratings yet
- RegistrationForm IbriDocument2 pagesRegistrationForm Ibrirenuthakkar01No ratings yet
- Perception REOIDocument14 pagesPerception REOIAtul GargNo ratings yet
- Applicant's Data Format 4.Document16 pagesApplicant's Data Format 4.Premanand ShenoyNo ratings yet
- Adobe Scan May 27, 2024Document5 pagesAdobe Scan May 27, 2024Priyanka KushwahaNo ratings yet
- 2006 08 01 - DR1Document1 page2006 08 01 - DR1Zach EdwardsNo ratings yet
- Site/Office Access Request From: Visitors' Information TimeDocument1 pageSite/Office Access Request From: Visitors' Information TimeslimaneNo ratings yet
- Training Bond Agreement SampleDocument3 pagesTraining Bond Agreement SampleSyarifah Mohd Nordin100% (1)
- PHREB Form No. 1.1a Application For Accreditationof Specialty ClinicsDocument5 pagesPHREB Form No. 1.1a Application For Accreditationof Specialty ClinicsDawn CasuncadNo ratings yet
- Reimbursement Claim FormDocument2 pagesReimbursement Claim FormanjnaNo ratings yet
- Reimbursement Claim FormDocument3 pagesReimbursement Claim FormGanesh Kumar100% (1)
- Medi Assist Complete FormDocument4 pagesMedi Assist Complete FormKhushi ChauhanNo ratings yet
- Curriculum Vitae of The Technical Intern Trainee: Reference Form 1-3Document19 pagesCurriculum Vitae of The Technical Intern Trainee: Reference Form 1-3Andang Tri MulyoNo ratings yet
- Application Form - WiproDocument4 pagesApplication Form - WiproVictorBotezNo ratings yet
- Candidate Personal Data SheetDocument3 pagesCandidate Personal Data SheetIndra Nath MishraNo ratings yet
- Reimbursement - Claim - Form and Check List RandstadDocument3 pagesReimbursement - Claim - Form and Check List RandstadSajed AliNo ratings yet
- BBCP4103 Career Planning and DevelopmentDocument8 pagesBBCP4103 Career Planning and DevelopmentSimon RajNo ratings yet
- Affidavit Firm UpnedaDocument1 pageAffidavit Firm Upnedawevaba5480No ratings yet
- Aetna Group Life ApplicationDocument3 pagesAetna Group Life ApplicationLeslie EchinNo ratings yet
- Last Date:: 10 Jun 2019: UMS Navigation Important Links Change PasswordDocument1 pageLast Date:: 10 Jun 2019: UMS Navigation Important Links Change PasswordGaurav RaiNo ratings yet
- The Art ofDocument5 pagesThe Art ofKara Van ArsdaleNo ratings yet
- I No.I Name I Email I Contact No. I: Idea Submission FormDocument4 pagesI No.I Name I Email I Contact No. I: Idea Submission FormpulkitNo ratings yet
- Register of Chemicals 1Document2 pagesRegister of Chemicals 1AMIR AFHAMNo ratings yet
- Dummy Reimbursement Claim Form Part A & BDocument2 pagesDummy Reimbursement Claim Form Part A & Bmayo gamerNo ratings yet
- Agent Application Form For Representing UNICDocument2 pagesAgent Application Form For Representing UNICEdu DharmasenaNo ratings yet
- Search For Outstanding Government Workers: Group CategoryDocument4 pagesSearch For Outstanding Government Workers: Group CategorychaneyNo ratings yet
- 9aa12807 Application Form - Digital CampaignerDocument4 pages9aa12807 Application Form - Digital CampaignerMagda LenaNo ratings yet
- Employee Application Form GEMS EnjoyDocument5 pagesEmployee Application Form GEMS Enjoydevilsucker9No ratings yet
- Mgt. Application-Square Textiles PLCDocument4 pagesMgt. Application-Square Textiles PLCnasim1761No ratings yet
- Expression of Interest For Partnership TemplateDocument3 pagesExpression of Interest For Partnership Templatedinesh.mhrhNo ratings yet
- EPD Form - ExperiencedDocument4 pagesEPD Form - ExperiencedVaishali SinghNo ratings yet
- Emp Application Form New 1Document4 pagesEmp Application Form New 1Mateen MughalNo ratings yet
- Master Application Form Version Sept 2022Document9 pagesMaster Application Form Version Sept 2022EMMANUEL TETTEHNo ratings yet
- Application FormatDocument6 pagesApplication Formatvinita123mauryaNo ratings yet
- Tati Nomination FormsDocument16 pagesTati Nomination FormsAl Manar PetroleumNo ratings yet
- Leadership Greatness and Organization EfDocument8 pagesLeadership Greatness and Organization EfSinta NoviaNo ratings yet
- Nigeria Computer Society - Individual-Membership-Form-06-02-2020Document5 pagesNigeria Computer Society - Individual-Membership-Form-06-02-2020Raphael EmediongNo ratings yet
- Company Name: Private & Confidential Submitted On: (For Office Use Only)Document3 pagesCompany Name: Private & Confidential Submitted On: (For Office Use Only)Sourabh KarmakarNo ratings yet
- Internship Form: (To Be Filled by Applicant)Document5 pagesInternship Form: (To Be Filled by Applicant)akber khan khanNo ratings yet
- AICTE - Monster - Com MoUDocument5 pagesAICTE - Monster - Com MoUSanjiv ErryNo ratings yet
- Xyz LTD: Application For Employment (Should Be Filled by Candidate Only) Instruction To Fill in The FormDocument5 pagesXyz LTD: Application For Employment (Should Be Filled by Candidate Only) Instruction To Fill in The FormKhalid HashmiNo ratings yet
- Pergas Employment Application Form-2024.01.25Document4 pagesPergas Employment Application Form-2024.01.25nanahasanaharrafiNo ratings yet
- Project Report FormatDocument17 pagesProject Report FormatAdil Javed CHNo ratings yet
- B.M.S. College of Engineering, Bengaluru-19: Application For Faculty PositionDocument5 pagesB.M.S. College of Engineering, Bengaluru-19: Application For Faculty PositioncrmreddyNo ratings yet
- Organizational Profiling Instrument: A. Basic InformationDocument8 pagesOrganizational Profiling Instrument: A. Basic InformationAbdulhamid Alawi JrNo ratings yet
- PHREB Form No. 1.2 Annual Report - October 29 2021 1 1Document4 pagesPHREB Form No. 1.2 Annual Report - October 29 2021 1 1Dawn CasuncadNo ratings yet
- Ma. Katherine InocencioDocument1 pageMa. Katherine InocencioVERA FilesNo ratings yet
- Club Pilates - 2015-10-28 - FDD - Xponential FitnessDocument233 pagesClub Pilates - 2015-10-28 - FDD - Xponential FitnessFuzzy PandaNo ratings yet
- Methodology of Installation of FencingDocument3 pagesMethodology of Installation of FencingA MakkiNo ratings yet
- Project Finance Application FormDocument16 pagesProject Finance Application FormAlidu Abdul-MajeedNo ratings yet
- Information Systems For ManagersDocument9 pagesInformation Systems For ManagersBijesh SiwachNo ratings yet
- Graduation Research ProjectDocument109 pagesGraduation Research ProjectRachana DasNo ratings yet
- Retail Management Tutorial-6.docx-1Document6 pagesRetail Management Tutorial-6.docx-1Melody AdralesNo ratings yet
- A. Definition and Concept of Taxation B. Nature of TaxationDocument1 pageA. Definition and Concept of Taxation B. Nature of TaxationJames BarzoNo ratings yet
- Itu Publications For Vessels Operating in Port LimitDocument6 pagesItu Publications For Vessels Operating in Port LimitVM ExportNo ratings yet
- UNIT 2 Product Development &product Life CycleDocument18 pagesUNIT 2 Product Development &product Life Cycletherashijain16No ratings yet
- A Study On Customer Perception Towards Advaith Hyundai, BangaloreDocument99 pagesA Study On Customer Perception Towards Advaith Hyundai, Bangaloresridhar mNo ratings yet
- A Guide On Tax Incentives /exemptions Available To The Uganda InvestorsDocument57 pagesA Guide On Tax Incentives /exemptions Available To The Uganda InvestorsGODFREY JATHONo ratings yet
- Carpenter Cover Letter SampleDocument6 pagesCarpenter Cover Letter Sampleafdmgoqxi100% (1)
- Corporate Attributes and Creative Accounting of Listed Consumer Firms in NigeriaDocument9 pagesCorporate Attributes and Creative Accounting of Listed Consumer Firms in NigeriaBOHR International Journal of Advances in Management ResearchNo ratings yet
- A Report On Organization StudyDocument63 pagesA Report On Organization StudyGowtham KSNo ratings yet
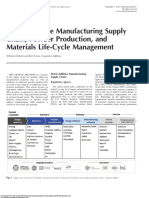
- Metal Additive Manufacturing Supply Chain, Powder Production, and Materials Life Cycle ManagementDocument14 pagesMetal Additive Manufacturing Supply Chain, Powder Production, and Materials Life Cycle ManagementtinaNo ratings yet
- Short and Sweet: Sherman Holbert's Mid-Century Mille Lacs Lake Maple Syrup ExperiementDocument9 pagesShort and Sweet: Sherman Holbert's Mid-Century Mille Lacs Lake Maple Syrup ExperiementMatt ThomasNo ratings yet
- The ASEAN Conversation - Muhammad Agung SaputraDocument2 pagesThe ASEAN Conversation - Muhammad Agung SaputraDewi PurnamasariNo ratings yet
- (Free Scores - Com) Lucato Fabrice Sola 95490 214Document8 pages(Free Scores - Com) Lucato Fabrice Sola 95490 214Nooi StrynckxNo ratings yet
- Grocery GuruDocument51 pagesGrocery GuruAbhishek Gautam0% (1)
- Hyped Mangoes Portfolio - Manila Malls-JcoDocument46 pagesHyped Mangoes Portfolio - Manila Malls-JcoMaria AlvarezNo ratings yet
- Dacanay vs. Asistio, Jr.Document1 pageDacanay vs. Asistio, Jr.Bryce KingNo ratings yet
- QXC210407-L1048 Crusher XC-GD20HP (Columbia+Ever Edinson Monsalve Salcedo)Document4 pagesQXC210407-L1048 Crusher XC-GD20HP (Columbia+Ever Edinson Monsalve Salcedo)Ever Edinson Monsalve SalcedoNo ratings yet
- Qci 9310 190.uDocument18 pagesQci 9310 190.uDaniel CorellaNo ratings yet
- Wordbox SMS ProposalDocument5 pagesWordbox SMS ProposalSATISH WORDBOXNo ratings yet
- Duplicate Result Card Application FormDocument4 pagesDuplicate Result Card Application FormShoaib akhterNo ratings yet
- State Bank of India Vrs Case Study: By: Saurabh AmbaselkarDocument17 pagesState Bank of India Vrs Case Study: By: Saurabh AmbaselkarSaurabh Ambaselkar0% (1)