Download as pdf or txt
You might also like
- Social Epidemiology-Oxford University Press 2014Document641 pagesSocial Epidemiology-Oxford University Press 2014Katherine Kath75% (4)
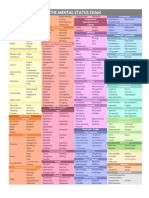
- Mse Cheat Sheet - Us Letter (Printable)Document1 pageMse Cheat Sheet - Us Letter (Printable)Ai Hwa Lim100% (1)
- Sociology Adolescent DrugDocument21 pagesSociology Adolescent DrugPravar JainNo ratings yet
- 1 s2.0 S0277953624000406 MainDocument8 pages1 s2.0 S0277953624000406 MainCGL Acting StudioNo ratings yet
- Summary of ReadingsDocument5 pagesSummary of Readingsmaricrisc.cagaNo ratings yet
- Social Science & Medicine: Phil Brown, Mercedes Lyson, Tania JenkinsDocument5 pagesSocial Science & Medicine: Phil Brown, Mercedes Lyson, Tania JenkinsVivian DiazNo ratings yet
- Introduction To Medical SociologyDocument16 pagesIntroduction To Medical SociologyGiorgi Jafaridze100% (1)
- Journal 2 InggDocument13 pagesJournal 2 InggNova LianaNo ratings yet
- People and SocietyDocument24 pagesPeople and Societynata.yamshinskayaNo ratings yet
- Notes For TestDocument44 pagesNotes For TestJingosi RAMPHARWANENo ratings yet
- 1-s2-1.0-S0277953608001093-mainDocument9 pages1-s2-1.0-S0277953608001093-mainVanessa MouraNo ratings yet
- Research Paper FinalDocument11 pagesResearch Paper Finalapi-644440815No ratings yet
- Sociological ReflectionsDocument23 pagesSociological Reflectionsavani dharNo ratings yet
- Theories of Practice and Public Health Understanding Un Healthy PracticesDocument16 pagesTheories of Practice and Public Health Understanding Un Healthy PracticesjuanpaNo ratings yet
- Editorial: Social Ties and Health Promotion: Suggestions For Population-Based ResearchDocument5 pagesEditorial: Social Ties and Health Promotion: Suggestions For Population-Based ResearchamaliaNo ratings yet
- Sociology 2 Final PorductDocument4 pagesSociology 2 Final Porducthina rasoolNo ratings yet
- Sociological PerspectiveDocument2 pagesSociological PerspectiveHania AdilNo ratings yet
- Reflective JournalDocument3 pagesReflective JournalArchi PrajapatiNo ratings yet
- Different Social Network and Social SupportDocument11 pagesDifferent Social Network and Social SupportIra Nur HumairaNo ratings yet
- Lecture 42: New Issues Before The Sociologists Slide 1Document18 pagesLecture 42: New Issues Before The Sociologists Slide 1Jaf ShahNo ratings yet
- Comprender Los Factores Sociales y Las Desigualdades en Salud. Progreso Del Siglo 20 y Perspectivas Del Siglo 21Document19 pagesComprender Los Factores Sociales y Las Desigualdades en Salud. Progreso Del Siglo 20 y Perspectivas Del Siglo 21IVAN DARIO RODRIGUEZ SALAMANCANo ratings yet
- The Impact of Social Norms On The Mental Health of Young PeopleDocument10 pagesThe Impact of Social Norms On The Mental Health of Young PeopleOla Hamdy Aly Abdelrazek AlyNo ratings yet
- Community Psychology Unit 1-7Document55 pagesCommunity Psychology Unit 1-7renukamuraliNo ratings yet
- Medical SociologyDocument14 pagesMedical SociologymymagicookieNo ratings yet
- Social Media Addiction - Concept PaperDocument11 pagesSocial Media Addiction - Concept PaperravenlucernasNo ratings yet
- Associations Between Loneliness and Perceived Social Support and Outcomes of Mental Health Problems: A Systematic ReviewDocument16 pagesAssociations Between Loneliness and Perceived Social Support and Outcomes of Mental Health Problems: A Systematic ReviewMonica TrifitrianaNo ratings yet
- Social Causation and Social ConstructionDocument6 pagesSocial Causation and Social Constructionhuberpadilla100% (1)
- Untitled DocumentDocument12 pagesUntitled DocumentKritika GuptaNo ratings yet
- (1989) Waitzkin - A Critical Theory of Medical Discourse PDFDocument20 pages(1989) Waitzkin - A Critical Theory of Medical Discourse PDFjoaquín arrosamenaNo ratings yet
- Sociology and Health ArticleDocument19 pagesSociology and Health ArticleAna Victoria Aguilera RangelNo ratings yet
- 1 s2.0 S0028390821000721 MainDocument21 pages1 s2.0 S0028390821000721 MainazizaNo ratings yet
- Juvenile Drug AddictionDocument5 pagesJuvenile Drug Addictionmcharo895No ratings yet
- Why Study Social ScienceDocument2 pagesWhy Study Social ScienceJoyce OrdaNo ratings yet
- Definitions: The Social Determinants of Health. SummaryDocument4 pagesDefinitions: The Social Determinants of Health. SummaryS VaibhavNo ratings yet
- PLS 3 Mid Term Analyzing Social Problems SodiqDocument8 pagesPLS 3 Mid Term Analyzing Social Problems SodiqReal LJ GagnonNo ratings yet
- Drug and Substance AbuseDocument5 pagesDrug and Substance AbuseWafula RonaldNo ratings yet
- Social Problems Community Psychology Vs Public Health ApproachDocument7 pagesSocial Problems Community Psychology Vs Public Health ApproachDalene Kirsten100% (1)
- LC459 CW1 SOH (Jubair) (Feedback)Document10 pagesLC459 CW1 SOH (Jubair) (Feedback)Death StrokeNo ratings yet
- COMMUNITY PSYCHOLOGY - Handout For StudentsDocument10 pagesCOMMUNITY PSYCHOLOGY - Handout For StudentsArunima RoyNo ratings yet
- 02 Dwornik CopyEdited 22 2 FinalDocument16 pages02 Dwornik CopyEdited 22 2 FinalShir LeyNo ratings yet
- 30.08.22 - All Medicine Is SocialDocument4 pages30.08.22 - All Medicine Is SocialPola PhotographyNo ratings yet
- The Major Health Implicationsof Social ConnectionDocument9 pagesThe Major Health Implicationsof Social ConnectionMaggay LarsNo ratings yet
- Labeling TheoryDocument9 pagesLabeling TheoryvaleriaguesthouseNo ratings yet
- Suicide Edited 2Document12 pagesSuicide Edited 2RanitaNo ratings yet
- Sociological Imagination AssignmentDocument4 pagesSociological Imagination AssignmentjiyakochharNo ratings yet
- Conrad & Barker - The Social Construction of IllnessDocument14 pagesConrad & Barker - The Social Construction of Illnesstomaa08No ratings yet
- Sociology and Oral HealthDocument27 pagesSociology and Oral HealthPrabhu Aypa100% (1)
- Akhter - Influences of Social Issues On Type 1 Diabetes Self Management Are We Doing EnoughDocument7 pagesAkhter - Influences of Social Issues On Type 1 Diabetes Self Management Are We Doing EnoughAlexandraNo ratings yet
- Mental Health and Societ Meenu WalterDocument7 pagesMental Health and Societ Meenu Waltervihaansingh323No ratings yet
- Ayoko NaDocument2 pagesAyoko Na9gj7hcbqn5No ratings yet
- Cislaghi & Heise 2020 - Gender As A TermDocument16 pagesCislaghi & Heise 2020 - Gender As A TermRia AnggrainiNo ratings yet
- A Critical Theory of Medical DiscourseDocument21 pagesA Critical Theory of Medical DiscourseMarita RodriguezNo ratings yet
- (Julie McLeod and Katie Wright) The Talking Cure in Everyday Life Gender, Generations and FriendshipDocument19 pages(Julie McLeod and Katie Wright) The Talking Cure in Everyday Life Gender, Generations and FriendshipValerita83No ratings yet
- Social Representations Psychologyst Luisa CadenaDocument19 pagesSocial Representations Psychologyst Luisa CadenaLuisa Fernanda CadenaNo ratings yet
- Bryant - 2016 - Chapter 2-Ways of KnowingDocument34 pagesBryant - 2016 - Chapter 2-Ways of Knowingisabella brantonNo ratings yet
- Review of The Roots of Youth Violence Literature Reviews Social Disorganization TheoryDocument6 pagesReview of The Roots of Youth Violence Literature Reviews Social Disorganization Theoryc5rc7pprNo ratings yet
- Sociology and Public Health Perspectives For ApplicationDocument7 pagesSociology and Public Health Perspectives For ApplicationAmanda KeslyNo ratings yet
- Lippincott Williams & Wilkins Is Collaborating With JSTOR To Digitize, Preserve and Extend Access To Medical CareDocument13 pagesLippincott Williams & Wilkins Is Collaborating With JSTOR To Digitize, Preserve and Extend Access To Medical CareMónica MartínezNo ratings yet
- Social and Structural Determinants of HealthDocument6 pagesSocial and Structural Determinants of HealthABIGAIL DAVILANo ratings yet
- Ties That Enable: Community Solidarity for People Living with Serious Mental Health ProblemsFrom EverandTies That Enable: Community Solidarity for People Living with Serious Mental Health ProblemsNo ratings yet
- Ursin 1993 - Psychobiology of Coping and Defence StrategiesDocument6 pagesUrsin 1993 - Psychobiology of Coping and Defence StrategiesValentin KalinovNo ratings yet
- Vaillant, Bond, Vaillant 1986 - An Empirically Validated Hierarchy of Defense MechanismsDocument9 pagesVaillant, Bond, Vaillant 1986 - An Empirically Validated Hierarchy of Defense MechanismsValentin KalinovNo ratings yet
- Johnson 1999 - Three Psychodynamic Perspectives On AddictionDocument25 pagesJohnson 1999 - Three Psychodynamic Perspectives On AddictionValentin KalinovNo ratings yet
- Rusnakova2014 - Codependency in Alcoholic FamiliesDocument7 pagesRusnakova2014 - Codependency in Alcoholic FamiliesValentin KalinovNo ratings yet
- Pryor2009 - Codependency and Bowen Undifferentiated SelfDocument5 pagesPryor2009 - Codependency and Bowen Undifferentiated SelfValentin KalinovNo ratings yet
- Cermak1986 - Diagnostic Criteria For CodependencyDocument7 pagesCermak1986 - Diagnostic Criteria For CodependencyValentin KalinovNo ratings yet
- Arnold1990 - Codependency. Hospital As A Dysfunctional FamilyDocument4 pagesArnold1990 - Codependency. Hospital As A Dysfunctional FamilyValentin KalinovNo ratings yet
- Kendler Mental Disorders PDFDocument8 pagesKendler Mental Disorders PDFJoaquín OlivaresNo ratings yet
- STEP Scale For Time and Space PsychosisDocument11 pagesSTEP Scale For Time and Space PsychosisValentin KalinovNo ratings yet
- How To Motivate Yourself To Study-Study Motivation For StudentsDocument2 pagesHow To Motivate Yourself To Study-Study Motivation For StudentsMuhammad Shamoeel Ul NaeemNo ratings yet
- COM60904 InnovativeMedia 202303 AB3 FignonDocument2 pagesCOM60904 InnovativeMedia 202303 AB3 FignonLINGTAO FENGNo ratings yet
- The Role of Program Leaders in The Use oDocument137 pagesThe Role of Program Leaders in The Use oRodel Ramos DaquioagNo ratings yet
- Trauma and TreatmentDocument16 pagesTrauma and Treatmentj.jaffrin.jNo ratings yet
- Bullying Research Project 1Document19 pagesBullying Research Project 1api-355285322No ratings yet
- African American Health and Race Student SyllabusDocument7 pagesAfrican American Health and Race Student Syllabusapi-630325386No ratings yet
- The Wisdom of Psychopaths: What Saints, Spies, and Serial Killers Can Teach Us About SuccessDocument4 pagesThe Wisdom of Psychopaths: What Saints, Spies, and Serial Killers Can Teach Us About SuccessTeo AndreiNo ratings yet
- Internship Application Form: CRY-Child Rights and YouDocument4 pagesInternship Application Form: CRY-Child Rights and YoukakuNo ratings yet
- Rating Scales in PsychiatryDocument130 pagesRating Scales in PsychiatryMyeloma Protein100% (2)
- BUS105 Tutor-Marked Assignment Jan 2021 SemesterDocument4 pagesBUS105 Tutor-Marked Assignment Jan 2021 SemesterDaniyal AsifNo ratings yet
- Analytical Psychology-Carl JungDocument47 pagesAnalytical Psychology-Carl JungLucy MuemaNo ratings yet
- BES Guide To Interdisciplinary ResearchDocument36 pagesBES Guide To Interdisciplinary ResearchYuan WangNo ratings yet
- Amare GlobalDocument4 pagesAmare GlobalRenz Calex Cojamco SorianoNo ratings yet
- Functions of Attitudes: Attitude NotesDocument2 pagesFunctions of Attitudes: Attitude NotesTanisha AgarwalNo ratings yet
- Ogl 220 Module 2 Ei and Empathy WorksheetDocument2 pagesOgl 220 Module 2 Ei and Empathy Worksheetapi-670788105No ratings yet
- Personal Self-Care Plan: Day/Time Duration Body Mind Spirit Emotions Relationships WorkDocument1 pagePersonal Self-Care Plan: Day/Time Duration Body Mind Spirit Emotions Relationships WorkDen Mark LavillesNo ratings yet
- Detailed Lesson Plan in HealthDocument12 pagesDetailed Lesson Plan in HealthcherryannielosauragirayNo ratings yet
- S4 - SG - HOTS in Practice (English)Document14 pagesS4 - SG - HOTS in Practice (English)Iries DanoNo ratings yet
- Understanding The Experience of Drug Reformists Vis-À-Vis Demographic Profile of Drug Surrenderees in The Province of PampangaDocument19 pagesUnderstanding The Experience of Drug Reformists Vis-À-Vis Demographic Profile of Drug Surrenderees in The Province of PampangaRayNo ratings yet
- Per Dev ActivityDocument40 pagesPer Dev ActivityRhona Durangparang Benologa100% (2)
- Zarit Burden InventoruDocument1 pageZarit Burden InventoruAbeerah TariqNo ratings yet
- Ethiraj College For Women (Autonomous)Document4 pagesEthiraj College For Women (Autonomous)hemavathi .ANo ratings yet
- Client-Counsellor Feedback FormDocument1 pageClient-Counsellor Feedback FormsadiaghantyNo ratings yet
- Architectural Thesis On Mental HospitalDocument6 pagesArchitectural Thesis On Mental Hospitalaprilblountjackson100% (2)
- Chapter 1 Slides - IPS131Document36 pagesChapter 1 Slides - IPS131Nosipho MsimangoNo ratings yet
- Worry Models - ReviewDocument14 pagesWorry Models - ReviewSibealNo ratings yet
- Performance Appraisal Methods: Past Oriented Methods Consists ofDocument7 pagesPerformance Appraisal Methods: Past Oriented Methods Consists ofNang NangNo ratings yet
- Oxford Casof Forensic Psychiatry 1St Edition Nigel Eastman Full ChapterDocument64 pagesOxford Casof Forensic Psychiatry 1St Edition Nigel Eastman Full Chapterdavid.lucero121100% (5)
- Past-LifeMemoriesScopingreview Explore22 PDFDocument9 pagesPast-LifeMemoriesScopingreview Explore22 PDFchotu yadavNo ratings yet