Download as docx, pdf, or txt
You might also like
- TAMU EssaysDocument7 pagesTAMU EssaysAnakin Skywalker100% (2)
- CB Final Project On K&N'sDocument35 pagesCB Final Project On K&N'sGOHAR GHAFFARNo ratings yet
- Columbus - Hero or VillainDocument4 pagesColumbus - Hero or Villainapi-264258719No ratings yet
- Health Promotion of The Toddler and FamilyDocument44 pagesHealth Promotion of The Toddler and FamilyJuanaly BadiolaNo ratings yet
- Examples of Physical Development MilestonesDocument10 pagesExamples of Physical Development MilestonesJeko Betguen Palangi100% (1)
- Health Promotion of The Toddler and Family: by Nawal Galet Al-MataryDocument31 pagesHealth Promotion of The Toddler and Family: by Nawal Galet Al-Mataryjuanamay30gmailcomNo ratings yet
- EDUC 101 Final RevisionDocument48 pagesEDUC 101 Final RevisionKate SubacNo ratings yet
- Development TestDocument18 pagesDevelopment TesthypsdreamerNo ratings yet
- Child and Adolescent Development NotesDocument20 pagesChild and Adolescent Development NotesJacqueline Llano50% (2)
- Early Childhood StageDocument127 pagesEarly Childhood StageCat JimenezNo ratings yet
- Unit 2 Human Growth DevelopmentDocument15 pagesUnit 2 Human Growth DevelopmentMarcelo Jorge EuredjianNo ratings yet
- 7.0 Principles of Normal Development in Infancy and Early ChildhoodDocument9 pages7.0 Principles of Normal Development in Infancy and Early ChildhoodMary Jane Sebial ManceraNo ratings yet
- EbookDocument9 pagesEbookod armyNo ratings yet
- Orca Share Media1581242252384Document647 pagesOrca Share Media1581242252384Laila UbandoNo ratings yet
- Early ChildhoodDocument5 pagesEarly ChildhoodAnjali PariharNo ratings yet
- 4 InfancyDocument47 pages4 InfancyMary Joyce TalamanteNo ratings yet
- InfancyDocument64 pagesInfancysiddiquimahrukh82No ratings yet
- Early ChildhoodDocument43 pagesEarly Childhoodbukhari.humna12No ratings yet
- Physical DevelopmentDocument20 pagesPhysical DevelopmentKeith SantosNo ratings yet
- Group 2 Toddler and Family - 20231018 - 091549 - 0000Document46 pagesGroup 2 Toddler and Family - 20231018 - 091549 - 0000Romar Vincent Orig EyoNo ratings yet
- Group 2 Script (MCN)Document13 pagesGroup 2 Script (MCN)Karly Alissa TarubalNo ratings yet
- 123 EducDocument5 pages123 EducTitus NumerousNo ratings yet
- Physical Development of Infants and ToddlersDocument39 pagesPhysical Development of Infants and ToddlersMylene Mahinay67% (3)
- Child Growth and Physical DevelopmentDocument18 pagesChild Growth and Physical DevelopmentJenny-Vi Tegelan LandayanNo ratings yet
- Module 2 - Who Is The Child and Adolescent Learner...Document30 pagesModule 2 - Who Is The Child and Adolescent Learner...Tintin Llauderes LloricoNo ratings yet
- Childhood FinalDocument43 pagesChildhood FinalBlack PinkNo ratings yet
- Facilitating Learning GrowthDocument11 pagesFacilitating Learning GrowthEce CapiliNo ratings yet
- HUMAN GROWTH AND DEVELOPMENT and FACILITATING LEARNINGDocument5 pagesHUMAN GROWTH AND DEVELOPMENT and FACILITATING LEARNINGzhai bambalanNo ratings yet
- The Normal Toddler Growth and DevelopmentDocument8 pagesThe Normal Toddler Growth and DevelopmentJils SureshNo ratings yet
- The Child and Adolescent LearnerDocument47 pagesThe Child and Adolescent LearnerGladys GasgaNo ratings yet
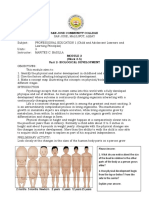
- San Jose Community CollegeDocument6 pagesSan Jose Community CollegeAnabel Jason BobilesNo ratings yet
- Child and Adolescent DevelopmentDocument19 pagesChild and Adolescent DevelopmentBenedickNo ratings yet
- Infancy, Thenewborn, and Infant Development: Mendoza, Jnymelrose Delacruz, Janella Rebogbog, Dianne Savari, DannyroseDocument24 pagesInfancy, Thenewborn, and Infant Development: Mendoza, Jnymelrose Delacruz, Janella Rebogbog, Dianne Savari, DannyroseHyacinth AlexaNo ratings yet
- MODULE 7 - Infancy and ToddlerhoodDocument22 pagesMODULE 7 - Infancy and ToddlerhoodRachelle DalingNo ratings yet
- Report BroadcastingDocument5 pagesReport BroadcastingkasjdkasNo ratings yet
- Milestone FinalDocument21 pagesMilestone FinalFransric TinampayNo ratings yet
- The Family With A ToddlerDocument36 pagesThe Family With A ToddlerDaryl Adrian RecaidoNo ratings yet
- Psychology-Development: Continuity/DiscontinuityDocument16 pagesPsychology-Development: Continuity/DiscontinuitymacaronloverNo ratings yet
- Physical Development of Infants and ToddlersDocument40 pagesPhysical Development of Infants and ToddlersIcah Mae D. Salo100% (1)
- Physical Development InfantsDocument36 pagesPhysical Development InfantsChrisel Joy Dela CruzNo ratings yet
- Edcad NotesDocument15 pagesEdcad NotesshaigestNo ratings yet
- ToddlerDocument60 pagesToddlerNasir AunaNo ratings yet
- Physical Development of Infants and ToddlersDocument30 pagesPhysical Development of Infants and ToddlersDiana Garcia SaclutiNo ratings yet
- INFANCY - Birth (One Month To 12 Months)Document7 pagesINFANCY - Birth (One Month To 12 Months)Sheena Irish AriosaNo ratings yet
- BABYHOODDocument67 pagesBABYHOODAna GNo ratings yet
- Infancy: by Shahla ArshadDocument32 pagesInfancy: by Shahla ArshadSana ShahNo ratings yet
- Growth and Development of Newborn To InfancyDocument54 pagesGrowth and Development of Newborn To Infancymerin sunilNo ratings yet
- Profed 1233Document24 pagesProfed 1233Rena UnanNo ratings yet
- PreschoolersDocument22 pagesPreschoolersShamae Perez100% (1)
- Masterfile Let ReviewerDocument1,566 pagesMasterfile Let ReviewerCLester MadShadowNo ratings yet
- MHGMGMDocument455 pagesMHGMGMEd Doloriel MoralesNo ratings yet
- Infancy: Birth To 2 YearsDocument52 pagesInfancy: Birth To 2 YearsVani JainNo ratings yet
- Infancy and ToddlerhoodDocument25 pagesInfancy and ToddlerhoodMark SultanNo ratings yet
- Professıonal Educatıon Test Questions and AnswersDocument778 pagesProfessıonal Educatıon Test Questions and Answersalger clerigoNo ratings yet
- Prof Ed N5 Child and AdolescentDocument20 pagesProf Ed N5 Child and Adolescentarmand rodriguezNo ratings yet
- Physical Development of Infants and ToddlersDocument31 pagesPhysical Development of Infants and ToddlersLeo Evidor100% (1)
- Infancy and ToddlerhoodDocument156 pagesInfancy and ToddlerhoodIrene Pulas100% (1)
- Group 3 Early Childhood Pre SchoolerDocument13 pagesGroup 3 Early Childhood Pre SchoolerCatherine LeeNo ratings yet
- Masterfile Let ReviewerDocument644 pagesMasterfile Let ReviewerApril Claire Pineda Manlangit50% (4)
- Parenting Toddlers Years Survival Guide for First-Time Dads: Navigating the Turbulent Toddler Terrain: A First-Time Dad's Survival GuideFrom EverandParenting Toddlers Years Survival Guide for First-Time Dads: Navigating the Turbulent Toddler Terrain: A First-Time Dad's Survival GuideNo ratings yet
- Stimulating Your Little One's Mind: Everything you need to help your newborn discover the worldFrom EverandStimulating Your Little One's Mind: Everything you need to help your newborn discover the worldRating: 3 out of 5 stars3/5 (1)
- Corporal Punishment, Physical AbuseDocument10 pagesCorporal Punishment, Physical AbuseCarla Isabel Ramírez SantosNo ratings yet
- Leadership Styles For 5 StagesDocument18 pagesLeadership Styles For 5 Stagesbimal.greenroadNo ratings yet
- South Sudan Gender AnalysisDocument68 pagesSouth Sudan Gender AnalysisOxfamNo ratings yet
- Unit 8 Lesson 1: Parts of The BodyDocument2 pagesUnit 8 Lesson 1: Parts of The BodyNguyễn PhúcNo ratings yet
- What's Your Paradigm WorksheetDocument2 pagesWhat's Your Paradigm WorksheetBruna JennyferNo ratings yet
- Long Quiz On Rational Algebraic ExpressionsDocument2 pagesLong Quiz On Rational Algebraic ExpressionsMARVIN ASILONo ratings yet
- Grammar BeGoingTo1 18821-1Document1 pageGrammar BeGoingTo1 18821-1CristinaNo ratings yet
- Development of Virtual Museum Model For YouthDocument5 pagesDevelopment of Virtual Museum Model For YouthSoumyadip RoyNo ratings yet
- Python Programming Notes - UNIT-IDocument69 pagesPython Programming Notes - UNIT-IGuru Chowdare MNo ratings yet
- Pe 2 - Introduction To DancesDocument57 pagesPe 2 - Introduction To DancesMelencio Dela Cruz INo ratings yet
- Content and Contextual Analysis of The Parisian LifeDocument7 pagesContent and Contextual Analysis of The Parisian LifeSowla sidoNo ratings yet
- Order SchedulingDocument26 pagesOrder Schedulingabhishek_s_gupta4753100% (1)
- KofiAgawu 2016 4TheRhythmicImaginati TheAfricanImaginationDocument40 pagesKofiAgawu 2016 4TheRhythmicImaginati TheAfricanImaginationMitia D'Acol100% (1)
- (Journal) Iain L. Densten and Judy H. Gray - Leadership Development and Reflection What Is The Connection PDFDocument6 pages(Journal) Iain L. Densten and Judy H. Gray - Leadership Development and Reflection What Is The Connection PDFAzwinNo ratings yet
- Research Paper Based On Weather Monitoring System Based in Raspberry PiDocument6 pagesResearch Paper Based On Weather Monitoring System Based in Raspberry PiParth PatelNo ratings yet
- Game Theory - Course Outline 2021Document4 pagesGame Theory - Course Outline 2021Mayank RanjanNo ratings yet
- Mindanao State University: College of Health Sciences Marawi CityDocument2 pagesMindanao State University: College of Health Sciences Marawi CityYanumy limb100% (1)
- Chapter 13 Nivea Case StudyDocument4 pagesChapter 13 Nivea Case Studylourdes germanNo ratings yet
- Building High Performing Teams: Facilitated by Marion StoneDocument34 pagesBuilding High Performing Teams: Facilitated by Marion Stoneumar.daha6484No ratings yet
- Variable Unit-Linked Training Manual: Vul/Ulp Licensing Manual (December 2014) I 1Document57 pagesVariable Unit-Linked Training Manual: Vul/Ulp Licensing Manual (December 2014) I 1Gus Delfin100% (1)
- Liljedahl v. Glassgow, 190 Iowa 827 (1921)Document6 pagesLiljedahl v. Glassgow, 190 Iowa 827 (1921)Jovelan V. EscañoNo ratings yet
- Reflection By: Wan Ahmad Fayadh Bin Wan IbrahimDocument3 pagesReflection By: Wan Ahmad Fayadh Bin Wan IbrahimcfghdftNo ratings yet
- Chapter 1, 2, 3 (Lovely)Document14 pagesChapter 1, 2, 3 (Lovely)Early Joy BorjaNo ratings yet
- Challenges Facing GraduateDocument95 pagesChallenges Facing GraduateGetu DeleluNo ratings yet
- Module 3 Literature ActivitiesDocument3 pagesModule 3 Literature ActivitiesAlexis Joy P. DangoNo ratings yet
- An Empirical Equation Relating Fatigue Limit and Mean Stress - NASA PDFDocument31 pagesAn Empirical Equation Relating Fatigue Limit and Mean Stress - NASA PDFjohnyboyNo ratings yet