Download as pdf or txt
You might also like
- Accommodations Tourist Arrival FormDocument1 pageAccommodations Tourist Arrival FormLia Eustaquio0% (1)
- Annex D - DILP Beneficiary FormDocument2 pagesAnnex D - DILP Beneficiary Formjulie cahilig71% (14)
- Benefit Guide Template 3Document18 pagesBenefit Guide Template 3TheChipper1979No ratings yet
- Salary Loan Record Form Rev2 (8.5 X 13)Document3 pagesSalary Loan Record Form Rev2 (8.5 X 13)KRYSTEL JUMANOYNo ratings yet
- SRS FormDocument2 pagesSRS FormJerz PortNo ratings yet
- Manila Science Recommendation FormDocument1 pageManila Science Recommendation FormWil MasongsongNo ratings yet
- Downloadable Application Form For Pasig City ScholarsDocument1 pageDownloadable Application Form For Pasig City ScholarsJohannah Mariano0% (3)
- Philippine Crop Insurance Corporation 1Document2 pagesPhilippine Crop Insurance Corporation 1LadyGrace BoniteNo ratings yet
- Deed of Sale - FormatDocument1 pageDeed of Sale - FormatAnne Aganap100% (1)
- CADACDocument58 pagesCADACBarangay Talon UnoNo ratings yet
- Diversity Lesson Plan: Book: Grade LevelDocument4 pagesDiversity Lesson Plan: Book: Grade Levelapi-334812888No ratings yet
- FM OO3 01.18 Kabuhayan Beneficiary Profile Form 022023Document1 pageFM OO3 01.18 Kabuhayan Beneficiary Profile Form 022023Mary Chris Celoso MedinaNo ratings yet
- Annex A1 - CS Form 100 - Revised 2023 - CSE (P) - A1 - Edited - A1Document2 pagesAnnex A1 - CS Form 100 - Revised 2023 - CSE (P) - A1 - Edited - A1marry-ann guinilingNo ratings yet
- EC Grievance Intake FormDocument1 pageEC Grievance Intake FormJelyn Bujatin100% (1)
- R E N E W A L F O R M: "Tulong Pang-Edukasyon para Sa Bulakenyo"Document2 pagesR E N E W A L F O R M: "Tulong Pang-Edukasyon para Sa Bulakenyo"T VinassaurNo ratings yet
- FORM2 - Oath of Undertaking-asof16June2021Document1 pageFORM2 - Oath of Undertaking-asof16June2021Ian Dione MartinezNo ratings yet
- Certificate of Non Disruption of ClassesDocument1 pageCertificate of Non Disruption of ClassesArianne Kimberlene AmorosoNo ratings yet
- Transaction SlipDocument2 pagesTransaction SlipSIMPLEJG88% (8)
- Meal Attendance and Registration FormDocument8 pagesMeal Attendance and Registration FormJaymeNo ratings yet
- LGBTQ FormDocument1 pageLGBTQ FormAbi GayleNo ratings yet
- Department-of-Agriculture-RXI ADocument2 pagesDepartment-of-Agriculture-RXI AMark Graganta56% (9)
- P3 CARES Application Form PDFDocument2 pagesP3 CARES Application Form PDFAnj Yonzon100% (3)
- PDS Blank FormDocument5 pagesPDS Blank Formax-120stNo ratings yet
- Form No. 01 Application For Fisheries InsuranceDocument1 pageForm No. 01 Application For Fisheries InsuranceCEDDFREY JOHN ENERIO AKUTNo ratings yet
- Certificate of Non RetirementDocument1 pageCertificate of Non RetirementLoida PatulotNo ratings yet
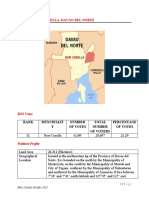
- Briefer New Corella, Davao Del Norte: Rank Muncipalit Y Number of Votes Total Number of Voters Percentage of VotesDocument4 pagesBriefer New Corella, Davao Del Norte: Rank Muncipalit Y Number of Votes Total Number of Voters Percentage of VotesYannah HidalgoNo ratings yet
- Damayan Membership Application Form: SCHOOL/OFFICE ADDRESSDocument1 pageDamayan Membership Application Form: SCHOOL/OFFICE ADDRESSRoselyn San Diego PacaigueNo ratings yet
- Sample Request Letter StandfanDocument1 pageSample Request Letter StandfanShinSan 77100% (1)
- Work and Financial PlanDocument1 pageWork and Financial PlanMarieta Alejo100% (1)
- SALN - Polly EnriquezDocument2 pagesSALN - Polly EnriquezJervel GuanzonNo ratings yet
- RA 9410 (CAM SUR Special Non Working Holiday) PDFDocument2 pagesRA 9410 (CAM SUR Special Non Working Holiday) PDFMD Prax100% (1)
- Position Descrition Form BlankDocument2 pagesPosition Descrition Form BlankAiness Aquino Duya100% (3)
- Certificate of IndigencyDocument4 pagesCertificate of IndigencyJOEL DACUMA BOLLIDONo ratings yet
- Office of The Sangguniang KabataanDocument2 pagesOffice of The Sangguniang KabataanMicky MoranteNo ratings yet
- Contract of Service Teacher LGU PaidDocument2 pagesContract of Service Teacher LGU PaidChele Tia100% (1)
- Boeform 101 Eapr 2012Document2 pagesBoeform 101 Eapr 2012Ma Victoria Lopez VaLenzuela20% (5)
- Deed of Sale of Jeepney VehicleDocument1 pageDeed of Sale of Jeepney VehicleJim Fernan Bristol Gonzales100% (2)
- (Insert Community Name) : Sample ResolutionDocument3 pages(Insert Community Name) : Sample Resolutionlito77No ratings yet
- Subscription Certificate PLDT Home Voice (Landline) and Data (Broadband) ServicesDocument3 pagesSubscription Certificate PLDT Home Voice (Landline) and Data (Broadband) Servicesneo14100% (1)
- Memorandum of AgreementDocument13 pagesMemorandum of AgreementAdrian AribatoNo ratings yet
- Dole Tupad ProgramDocument2 pagesDole Tupad ProgramGine Frencillo100% (1)
- Mun. Ordinance No. 010 (Pura Cockpit Arena)Document3 pagesMun. Ordinance No. 010 (Pura Cockpit Arena)fortunecNo ratings yet
- Groundbreaking Ceremony Program ScriptDocument4 pagesGroundbreaking Ceremony Program Scriptrodchiel.gensayaNo ratings yet
- Grade 4.oplan Kaluluwa - Pretest.SilentDocument2 pagesGrade 4.oplan Kaluluwa - Pretest.SilentMaria Venese AgapNo ratings yet
- Revised January 1992 Daily Wage PayrollDocument4 pagesRevised January 1992 Daily Wage PayrollJhem Martinez100% (1)
- Department of Omcatton: Schools Division Office of Camarxnies SurDocument6 pagesDepartment of Omcatton: Schools Division Office of Camarxnies SurVanessa CastilloNo ratings yet
- DepEd Order No. 35, S. 2003Document23 pagesDepEd Order No. 35, S. 2003Donnabelle VaronaNo ratings yet
- Endorsement-Letter-Lgu RizalDocument2 pagesEndorsement-Letter-Lgu RizalArdy Pamintuan0% (1)
- Letter To Brgy CaptainDocument1 pageLetter To Brgy CaptainSandy Lagata100% (1)
- Appendix 29 - CASH RECEIPTS RECORDDocument1 pageAppendix 29 - CASH RECEIPTS RECORDPau PerezNo ratings yet
- PAIS & RMD Table of Contents OkDocument3 pagesPAIS & RMD Table of Contents OkDerick James Ariola Casabal100% (1)
- Day Care Worker MasterlistDocument8 pagesDay Care Worker Masterlistshiena bignayNo ratings yet
- Appointment SK SecDocument1 pageAppointment SK SecAaliyah AlejandreNo ratings yet
- Miss Gay Grand International: Intelligence Impression (Preliminary)Document7 pagesMiss Gay Grand International: Intelligence Impression (Preliminary)Maria Karina FerrerasNo ratings yet
- Batelec Ii San Juan, Batangas: Paaralang Elementarya NG MarcalDocument2 pagesBatelec Ii San Juan, Batangas: Paaralang Elementarya NG MarcalChiela BagnesNo ratings yet
- Public Speaking in Public ServiceDocument5 pagesPublic Speaking in Public ServiceAceAsabuNo ratings yet
- Worksheet: Grade Six Second QuarterDocument5 pagesWorksheet: Grade Six Second QuarterCatherine Lagario Renante100% (1)
- Gcash Convinient Fee GuideDocument1 pageGcash Convinient Fee GuideZhiana Tangngob0% (1)
- Application For Provident Benefits (Apb) ClaimDocument2 pagesApplication For Provident Benefits (Apb) ClaimLIERANo ratings yet
- Ma. Perlita Binondo: Office of The Sangguniang KabataanDocument1 pageMa. Perlita Binondo: Office of The Sangguniang KabataanMicky MoranteNo ratings yet
- Idetect Profile Sheet BurgosDocument1 pageIdetect Profile Sheet BurgosGerome Bautista VInluanNo ratings yet
- Certification of No Pending Case DimeDocument1 pageCertification of No Pending Case DimeGilbert Guzman Turaray100% (1)
- 2017 TaxReturnDocument7 pages2017 TaxReturntripsrealplugNo ratings yet
- Parts FaDocument14 pagesParts Faadiladilzade98No ratings yet
- (PDF) Johnson VictorDocument6 pages(PDF) Johnson Victorchinmay vijay100% (1)
- Dac 100 Cat 2Document2 pagesDac 100 Cat 2Alistahr AmoloNo ratings yet
- SD - LO150 - Processes in Sales & DistributionDocument181 pagesSD - LO150 - Processes in Sales & Distributiondrbytes100% (1)
- Program HMMTFebruary2014Document10 pagesProgram HMMTFebruary2014xSonyWIiNo ratings yet
- ANM & GNMDocument66 pagesANM & GNMKaran SinghNo ratings yet
- Name: Teacher: Date: Score:: Probability Using A SpinnerDocument2 pagesName: Teacher: Date: Score:: Probability Using A SpinnerSara ShaiboonNo ratings yet
- LIT 1 FOOTNOTE TO YOUTH With ASSIGNMENTDocument6 pagesLIT 1 FOOTNOTE TO YOUTH With ASSIGNMENTAiel Legaspi EstepaNo ratings yet
- Activity 4Document3 pagesActivity 4Sittie Asnile MalacoNo ratings yet
- PRED Dharwad Circle 2018-19 SRDocument111 pagesPRED Dharwad Circle 2018-19 SRRameshkumar Hugar54% (13)
- O P Jindal Modern School, Hisar: Worksheet No. 3 Subject-Evs NAME: ................... ROLL NO. . Class 5Document2 pagesO P Jindal Modern School, Hisar: Worksheet No. 3 Subject-Evs NAME: ................... ROLL NO. . Class 5Raghav BansalNo ratings yet
- CombinepdfDocument208 pagesCombinepdfH. TэлмэнNo ratings yet
- Unit 1 Week 1Document15 pagesUnit 1 Week 1paramjyothiNo ratings yet
- Comptel Business Service Tool™: Functional DescriptionDocument25 pagesComptel Business Service Tool™: Functional DescriptionIvanIvanovNo ratings yet
- BiographyDocument6 pagesBiographyLucy del Carmen Mosquera Ibarguen100% (1)
- Taller de Ingles y Vocabulario ResueltoDocument11 pagesTaller de Ingles y Vocabulario ResueltoMayu Viloria100% (1)
- 06-23-18 EditionDocument31 pages06-23-18 EditionSan Mateo Daily JournalNo ratings yet
- RPS Literal ReadingDocument13 pagesRPS Literal ReadingFransiska Densiana LurukNo ratings yet
- Reading Passage 1Document13 pagesReading Passage 1Anh Lê Nguyễn KiềuNo ratings yet
- Conclusion Mustafa LutfiDocument9 pagesConclusion Mustafa LutfiAsmatullah KhanNo ratings yet
- Python Exception Handling - Try, Except and Finally PDFDocument1 pagePython Exception Handling - Try, Except and Finally PDFSyed Muhammad ShahbazNo ratings yet
- Shock Tunnel Studies of The Hypersonic Flowfield Around The Hypervelocity Ballistic Models With AerospikesDocument5 pagesShock Tunnel Studies of The Hypersonic Flowfield Around The Hypervelocity Ballistic Models With AerospikessaiNo ratings yet
- Understanding Community MediaDocument80 pagesUnderstanding Community MediaJuan Ramos MartínNo ratings yet
- Ens 301 0.5 MarkDocument16 pagesEns 301 0.5 Marknaveenssince04122002No ratings yet
- Spreading The NewsDocument3 pagesSpreading The NewsMENDEZ CHARLES ELMER C.No ratings yet
- The Merchant of Venice Act V QuizDocument3 pagesThe Merchant of Venice Act V QuizOnline SubsNo ratings yet
- Training CatalogDocument35 pagesTraining Catalogmohamed elsawafNo ratings yet