
Ceramic Bonded Inlays-Onlays: Case Series
Ceramic Bonded Inlays-Onlays: Case Series
You might also like
- Consumers Are People Too - FrogDocument36 pagesConsumers Are People Too - FrogMalek El BéjiNo ratings yet
- Immediate Dental Implant Placement Into Infected vs. Non-Infected Sockets: A Meta-AnalysisDocument7 pagesImmediate Dental Implant Placement Into Infected vs. Non-Infected Sockets: A Meta-Analysismarlene tamayoNo ratings yet
- Injection Overmolding For Aesthetics and Strength Part 2Document4 pagesInjection Overmolding For Aesthetics and Strength Part 2The Bioclear ClinicNo ratings yet
- Ultrasonic Periodontal Debridement: Theory and TechniqueFrom EverandUltrasonic Periodontal Debridement: Theory and TechniqueRating: 2.5 out of 5 stars2.5/5 (2)
- Exhibitor List 2019: Company Name Booth No. CountryDocument8 pagesExhibitor List 2019: Company Name Booth No. CountryBojana Dekic0% (1)
- Giuseppe-Marchetti-Composite-inlays-and-onlays-via-www.styleitaliano.orgDocument18 pagesGiuseppe-Marchetti-Composite-inlays-and-onlays-via-www.styleitaliano.orgBogdanŢimiraşNo ratings yet
- All Ceramic Inlay: A Case ReportDocument6 pagesAll Ceramic Inlay: A Case ReportIlsen ManzanillaNo ratings yet
- CADCAM Vs Traditional Ceramic InlayDocument10 pagesCADCAM Vs Traditional Ceramic InlayAya Ibrahim YassinNo ratings yet
- Direct Cuspal-Coverage Posterior Resin Composite Restorations: A Case ReportDocument8 pagesDirect Cuspal-Coverage Posterior Resin Composite Restorations: A Case ReportDinar ArdhananeswariNo ratings yet
- Ferrule PDFDocument7 pagesFerrule PDFVidya SenthuNo ratings yet
- Posterior Composite Restoration UpdateDocument10 pagesPosterior Composite Restoration UpdateBianca IovoaiaNo ratings yet
- Ceramics in Dentistry-Part I: Classes of MaterialsDocument6 pagesCeramics in Dentistry-Part I: Classes of MaterialsDilesh PradhanNo ratings yet
- Ceramic Inlay PreparationDocument9 pagesCeramic Inlay PreparationRaghu PratapNo ratings yet
- Esthetic Technique: Crown Considerations, Preparations, and Material Selection For Esthetic Metal-Ceramic RestorationsDocument16 pagesEsthetic Technique: Crown Considerations, Preparations, and Material Selection For Esthetic Metal-Ceramic RestorationsAyu Nur A'IniNo ratings yet
- Inlay OnlayDocument6 pagesInlay OnlayNur HayatiNo ratings yet
- IJEDe 15 03 Rocca 852 2Document22 pagesIJEDe 15 03 Rocca 852 2hannaly estradaNo ratings yet
- Eur JEsthet Dent 2013 MeyenbergDocument97 pagesEur JEsthet Dent 2013 Meyenbergsoma kiranNo ratings yet
- Clin DSDDocument5 pagesClin DSDAlfred OrozcoNo ratings yet
- INLAYDocument11 pagesINLAYMira AnggrianiNo ratings yet
- Aesthetic Rehab Visagism ConceptDocument7 pagesAesthetic Rehab Visagism ConceptvaamdevaaNo ratings yet
- Zucchelli Masterclass Course Program 2020Document11 pagesZucchelli Masterclass Course Program 2020ComarzzoNo ratings yet
- Cosmetic Dentistry CSD 2013Document3 pagesCosmetic Dentistry CSD 2013Rodrigo Daniel Vela RiveraNo ratings yet
- Vertical Ridge Augmentation and Soft Tissue Reconstruction of The Anterior Atrophic Maxillae - Urban2017Document12 pagesVertical Ridge Augmentation and Soft Tissue Reconstruction of The Anterior Atrophic Maxillae - Urban2017Claudio GuzmanNo ratings yet
- Dental ImplantsDocument9 pagesDental ImplantsPati Villalobos AntibiloNo ratings yet
- All Ceramic 5p PDFDocument6 pagesAll Ceramic 5p PDFWiwin Nuril FalahNo ratings yet
- Bulk Fill Composites For Class II Restorations by DentistryDocument12 pagesBulk Fill Composites For Class II Restorations by Dentistryddmorar486No ratings yet
- MagnificationDocument52 pagesMagnificationSiva KumarNo ratings yet
- Mclaren Smile AnalysisDocument15 pagesMclaren Smile AnalysisXavier Vargas PerezNo ratings yet
- The Endocrown - A Different Type of All-Ceramic Reconstruction For Molars - JcdaDocument10 pagesThe Endocrown - A Different Type of All-Ceramic Reconstruction For Molars - Jcdaabcder1234No ratings yet
- The International Journal of Periodontics & Restorative DentistryDocument10 pagesThe International Journal of Periodontics & Restorative Dentistrykevin1678No ratings yet
- Develop Lingual OrtoDocument68 pagesDevelop Lingual OrtoOrtodonti UnhasNo ratings yet
- Biologic Interfaces in Esthetic Dentistry Part IIDocument27 pagesBiologic Interfaces in Esthetic Dentistry Part IINoelia MadrizNo ratings yet
- Enrico Cassai The WORKING LENGTHDocument9 pagesEnrico Cassai The WORKING LENGTHAnca MartinoviciNo ratings yet
- 547792129c17bec4c106ead404e0c4ddDocument52 pages547792129c17bec4c106ead404e0c4ddHugoRoCkstarNo ratings yet
- Deliperi S - PPAD - 2005 PDFDocument9 pagesDeliperi S - PPAD - 2005 PDFAlfredo PortocarreroNo ratings yet
- Afraccion PDFDocument9 pagesAfraccion PDFzayraNo ratings yet
- AnyRidge EngwebDocument128 pagesAnyRidge EngwebPinky Tolani100% (1)
- HTTP WWW - Styleitaliano.org Esthetic Dentistry in PaediatricsDocument9 pagesHTTP WWW - Styleitaliano.org Esthetic Dentistry in PaediatricsAmee PatelNo ratings yet
- Course 2 Jordi Anna 2018 Brochure 1Document6 pagesCourse 2 Jordi Anna 2018 Brochure 1mhd ssaghNo ratings yet
- Telescopic Dentures: An Overlooked TechnologyDocument3 pagesTelescopic Dentures: An Overlooked TechnologyarchanglsNo ratings yet
- Noncarious Cervical Lesions As Abfraction Etiology Diagnosis and Treatmentmodalities of Lesions A Review Article 2161 1122 1000438 PDFDocument6 pagesNoncarious Cervical Lesions As Abfraction Etiology Diagnosis and Treatmentmodalities of Lesions A Review Article 2161 1122 1000438 PDFFaniaNo ratings yet
- Ultimate Ceramic Veneers A Laboratory-Guided Ultraconservative PreparationDocument15 pagesUltimate Ceramic Veneers A Laboratory-Guided Ultraconservative PreparationEvelina HaddadienNo ratings yet
- Zirconia in Dentistry Part 2. Evidence-BDocument33 pagesZirconia in Dentistry Part 2. Evidence-Bt723849No ratings yet
- EJED2 Dietschi 329Document18 pagesEJED2 Dietschi 329Alexis Alberto Rodríguez Jiménez100% (1)
- Posterior Indirect AdhesiveDocument34 pagesPosterior Indirect AdhesiveAlondra CevallosNo ratings yet
- Digital Smile Design: A Tool For Treatment Planning and Communication in Esthetic DentistryDocument10 pagesDigital Smile Design: A Tool For Treatment Planning and Communication in Esthetic Dentistrygilberto69No ratings yet
- 3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFDocument10 pages3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFAnisha AnilNo ratings yet
- Aesthetic Evolution - 7 Lessons of Indirect RestorationDocument10 pagesAesthetic Evolution - 7 Lessons of Indirect RestorationAndreea StaicuNo ratings yet
- Casebook IconVE 07022019 enDocument45 pagesCasebook IconVE 07022019 envanity fairNo ratings yet
- Criteria For The Selection of Restoration Materials PDFDocument8 pagesCriteria For The Selection of Restoration Materials PDFSofia BoteroNo ratings yet
- 2 - Evaluation of Bond Strength and Thickness of Adhesive Layer According To The Techniques of Applying Adhesives in Composite Resin RestorationsDocument7 pages2 - Evaluation of Bond Strength and Thickness of Adhesive Layer According To The Techniques of Applying Adhesives in Composite Resin RestorationskochikaghochiNo ratings yet
- Orhan 2021 (Book) - Ultrasonography in Dentomaxillofacial Diagnostics - SpringerDocument372 pagesOrhan 2021 (Book) - Ultrasonography in Dentomaxillofacial Diagnostics - SpringerlagianggenNo ratings yet
- Nanofilled Resin Composite Properties and Clinical Performance - A ReviewDocument18 pagesNanofilled Resin Composite Properties and Clinical Performance - A ReviewInside Dentistry educationNo ratings yet
- Digital Smile Design - Predictable Results (#741934) - 1117267Document6 pagesDigital Smile Design - Predictable Results (#741934) - 1117267yuumiNo ratings yet
- Clinical Tips: 25 For General PracticeDocument6 pagesClinical Tips: 25 For General PracticethiatuslNo ratings yet
- CDA June 2021 Journal - ISSUU - 060121Document56 pagesCDA June 2021 Journal - ISSUU - 060121abdulaziz alzaidNo ratings yet
- Advantages of Adhesive in DentistryDocument29 pagesAdvantages of Adhesive in DentistryAnonymous CY62A9No ratings yet
- Microsurgery in EndodonticsFrom EverandMicrosurgery in EndodonticsSyngcuk KimNo ratings yet
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionFrom EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNo ratings yet
- Analysis of Opaque, Peel-Off and Flex Rejects in the Electro Plating Process Using the Six Sigma Dmaic MethodDocument18 pagesAnalysis of Opaque, Peel-Off and Flex Rejects in the Electro Plating Process Using the Six Sigma Dmaic MethodInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Study to Effect of Reminiscence Therapy on Psychological Well-Being among Elderly Residing in Selected Old Age HomeDocument5 pagesA Study to Effect of Reminiscence Therapy on Psychological Well-Being among Elderly Residing in Selected Old Age HomeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Application of Project Management using CPM (Critical Path Method) and Pert (Project Evaluation and Review Technique) in the Nava House Bekasi Cluster Housing Development ProjectDocument12 pagesApplication of Project Management using CPM (Critical Path Method) and Pert (Project Evaluation and Review Technique) in the Nava House Bekasi Cluster Housing Development ProjectInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Comprehensive Review on the Therapeutic Potential of PectinDocument6 pagesA Comprehensive Review on the Therapeutic Potential of PectinInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Application of the Economic Order Quantity (EOQ) Method on the Supply of Chemical Materials in the Laboratory of PT. Fajar Surya Wisesa TbkDocument15 pagesApplication of the Economic Order Quantity (EOQ) Method on the Supply of Chemical Materials in the Laboratory of PT. Fajar Surya Wisesa TbkInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Rare Complication: Cardiac Arrest and Pulmonary Embolism in Polyarteritis NodosaDocument5 pagesA Rare Complication: Cardiac Arrest and Pulmonary Embolism in Polyarteritis NodosaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Integrated Border Security System on Human Trafficking in Bangladesh: The Mediating Effect of the Use of Advanced TechnologyDocument12 pagesThe Impact of Integrated Border Security System on Human Trafficking in Bangladesh: The Mediating Effect of the Use of Advanced TechnologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Quality Control to Reduce Appearance Defects at PT. Musical InstrumentDocument11 pagesQuality Control to Reduce Appearance Defects at PT. Musical InstrumentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Forecasting PM10 Concentrations Using Artificial Neural Network in Imphal CityDocument10 pagesForecasting PM10 Concentrations Using Artificial Neural Network in Imphal CityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of Carton Packaging Quality Control Using Statistical Quality Control Methods at PT XYZDocument10 pagesAnalysis of Carton Packaging Quality Control Using Statistical Quality Control Methods at PT XYZInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Quizlet's Usefulness for Vocabulary Learning: Perceptions of High-Level and Low-Level Chinese College EFL LearnersDocument5 pagesQuizlet's Usefulness for Vocabulary Learning: Perceptions of High-Level and Low-Level Chinese College EFL LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Enhancing Estimating the Charge Level in Electric Vehicles: Leveraging Force Fluctuation and Regenerative Braking DataDocument6 pagesEnhancing Estimating the Charge Level in Electric Vehicles: Leveraging Force Fluctuation and Regenerative Braking DataInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Entrepreneurial Adult Education as a Catalyst for Youth Employability in Disadvantaged AreasDocument9 pagesEntrepreneurial Adult Education as a Catalyst for Youth Employability in Disadvantaged AreasInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Role of Leadership Training in Developing Effective Police SupervisorsDocument17 pagesThe Role of Leadership Training in Developing Effective Police SupervisorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Health Care - An Android Application Implementation and Analyzing user Experience Using PythonDocument7 pagesHealth Care - An Android Application Implementation and Analyzing user Experience Using PythonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrusion Detection System with Ensemble Machine Learning Approaches using VotingClassifierDocument4 pagesIntrusion Detection System with Ensemble Machine Learning Approaches using VotingClassifierInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Synthetic and Natural Vitamin C Modulation of Leaded Paint-Induced Nephrotoxicity of Automobile Painters in Ile-Ife, Nigeria.Document21 pagesSynthetic and Natural Vitamin C Modulation of Leaded Paint-Induced Nephrotoxicity of Automobile Painters in Ile-Ife, Nigeria.International Journal of Innovative Science and Research TechnologyNo ratings yet
- Visitor Perception Related to the Quality of Service in Todo Tourism VillageDocument10 pagesVisitor Perception Related to the Quality of Service in Todo Tourism VillageInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Gravity Investigations Applied to the Geological Framework Study of the Mambasa Territory in Democratic Republic of CongoDocument9 pagesGravity Investigations Applied to the Geological Framework Study of the Mambasa Territory in Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Developing Digital Fluency in Early Education: Narratives of Elementary School TeachersDocument11 pagesDeveloping Digital Fluency in Early Education: Narratives of Elementary School TeachersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A New Model of Rating to Evaluate Start-ups in Emerging Indian MarketDocument7 pagesA New Model of Rating to Evaluate Start-ups in Emerging Indian MarketInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Proof of Concept Using BLE to Optimize Patients Turnaround Time (PTAT) in Health CareDocument14 pagesA Proof of Concept Using BLE to Optimize Patients Turnaround Time (PTAT) in Health CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Financial Prudence as Determinant of Employees’ Interest in Graduate StudyDocument13 pagesFinancial Prudence as Determinant of Employees’ Interest in Graduate StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design and Implementation of Software-Defined ReceiverDocument8 pagesDesign and Implementation of Software-Defined ReceiverInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Optimizing Bio-Implant Materials for Femur Bone Replacement:A Multi-Criteria Analysis and Finite Element StudyDocument5 pagesOptimizing Bio-Implant Materials for Femur Bone Replacement:A Multi-Criteria Analysis and Finite Element StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Crop Monitoring System with Water Moisture Levels Using ControllerDocument8 pagesCrop Monitoring System with Water Moisture Levels Using ControllerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Inclusive Leadership in the South African Police Service (SAPS)Document26 pagesInclusive Leadership in the South African Police Service (SAPS)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Naturopathic Approaches to Relieving Constipation: Effective Natural Treatments and TherapiesDocument9 pagesNaturopathic Approaches to Relieving Constipation: Effective Natural Treatments and TherapiesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fahfi/Mochaina Illegal Gambling Activities and its Average Turnover within Limpopo ProvinceDocument8 pagesFahfi/Mochaina Illegal Gambling Activities and its Average Turnover within Limpopo ProvinceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Year Wise Analysis and Prediction of Gold RatesDocument8 pagesYear Wise Analysis and Prediction of Gold RatesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Vegan LifeDocument116 pagesVegan Lifepelouse23100% (12)
- Female GenitaliaDocument96 pagesFemale GenitaliaJopaii TanakaNo ratings yet
- Materia Medica For Students Part I Ritu Kinra.00247 2introductionDocument5 pagesMateria Medica For Students Part I Ritu Kinra.00247 2introductionRohini Chaudhari33% (3)
- Revision Test 4 - Class 12D1 2021-2022Document7 pagesRevision Test 4 - Class 12D1 2021-2022Tenebrae LuxNo ratings yet
- HIRARC On Fertilisation - SI - 2022Document6 pagesHIRARC On Fertilisation - SI - 2022noor khairaniNo ratings yet
- Mark Keterangan: Acuan Perencanaan Alat Kesehatan Kode Rs 3216441 Form f3Document18 pagesMark Keterangan: Acuan Perencanaan Alat Kesehatan Kode Rs 3216441 Form f3igdNo ratings yet
- Kenya Basic Education Covid - 19 Emergency Response PlanDocument53 pagesKenya Basic Education Covid - 19 Emergency Response Planh3493061No ratings yet
- 1340701015binder2Document39 pages1340701015binder2CoolerAdsNo ratings yet
- List of Subject CodesDocument1 pageList of Subject CodesAnonymous YooNo ratings yet
- En Manu RVDocument90 pagesEn Manu RVMurat CanNo ratings yet
- New Wordpad DocumentDocument41 pagesNew Wordpad DocumentSherwin TuckerNo ratings yet
- PopipDocument2 pagesPopipRaj Kumar KNo ratings yet
- 1 RT08 Occupational Exposure WEBDocument87 pages1 RT08 Occupational Exposure WEBRichar Pinedo CadilloNo ratings yet
- Level 12 Analogies 2 PDFDocument3 pagesLevel 12 Analogies 2 PDFCarlson AberinNo ratings yet
- Ies RDocument3 pagesIes RNikoleta HirleaNo ratings yet
- Brief Introduction To HospitalDocument11 pagesBrief Introduction To Hospitalkanika jainNo ratings yet
- 2 Risk Identification FormDocument6 pages2 Risk Identification FormkamranNo ratings yet
- Predisposing Factor of Fungal InfectionDocument13 pagesPredisposing Factor of Fungal InfectionDitha RizkyNo ratings yet
- Medicaid Edit CodesDocument79 pagesMedicaid Edit CodesNeil GilstrapNo ratings yet
- August 7, 2015 Strathmore Times PDFDocument28 pagesAugust 7, 2015 Strathmore Times PDFStrathmore TimesNo ratings yet
- Medical Passport - Enteral NutritionDocument4 pagesMedical Passport - Enteral NutritionDovlet AmanovNo ratings yet
- Unilateral Neglect: Assessment and Rehabilitation: Richard P. Conti, Jacqueline M. ArnoneDocument10 pagesUnilateral Neglect: Assessment and Rehabilitation: Richard P. Conti, Jacqueline M. Arnonejerrin jacobNo ratings yet
- Case Report 2Document2 pagesCase Report 2respikNo ratings yet
- Safety Alert - Grinder WheelDocument3 pagesSafety Alert - Grinder WheelsarojNo ratings yet
- CGSM Form No. 1 Community SurveyDocument3 pagesCGSM Form No. 1 Community SurveyJulia PicoNo ratings yet
- Latent Autoimmune Diabetes in Adults TDDocument3 pagesLatent Autoimmune Diabetes in Adults TDapi-648595816No ratings yet
- Nursing Responsibilities For METRONIDAZOLEDocument1 pageNursing Responsibilities For METRONIDAZOLEIsrael Soria Espero63% (8)
- Lesson Plan in Health IV JonaDocument8 pagesLesson Plan in Health IV JonaJenelyn Limen100% (1)






















































































































Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Ceramic Bonded Inlays-Onlays: Case Series
1
Emna Boudabous, 2 Ilhem Ben Othmen* , 3Islam El Ayachi, 4Marwa Amara ,
5
Dalenda Hadyaoui, 6Zohra Nouira, 7Harzallah Belhassen ,8Mounir Cherif
Department of Fixed Prosthodontics, Research Laboratory of Occlusodontics and Ceramic, University of Monastir, Tunisia
Corresponding author: 2 Ilhem Ben Othmen*
Abstract:- Inlay/onlay restorations have emerged as a Among these options, bonded ceramic inlays-onlays
conservative and effective approach to restore posterior stand out as a contemporary, highly aesthetic, and
teeth with extensive cavities, while considering aesthetic, conservative therapeutic choice for restoring decayed teeth,
biological, and mechanical factors. This restorative whether vital or pulpless. However, their success and
technique has gained significant popularity in routine longevity rely on achieving a precise alignment between
dental practice and has been extensively documented in clinical indications, adherence to preparation principles,
scientific literature, owing to advancements in digital careful selection of materials, and appropriate bonding
technologies and contemporary aesthetic materials. protocols.
Nonetheless, the effectiveness and durability of
inlay/onlay restorations hinge upon achieving optimal Case Report 1
alignment between clinical indications, preparation A female patient, aged 40, with good overall health,
principles, material selection, and bonding protocols. In presented at the Fixed Prosthodontics Department at the
this article, an updated perspective on this type of partial dental clinic in Monastir seeking dental consultation for the
prosthesis is presented through two clinical cases report: restoration of her endodontically treated first molar filled
the first case report which describes the rehabilitation of with a defective amalgam. The patient did not exhibit any
a severely damaged maxillary molar using an Indirect parafunctional habits. Upon removal of the filling on the
CAD/CAM fabricated ceramic inlay-onlay, thereby first molar, a moderate occluso-proximal cavity was
shedding light on the latest advancements in this field. observed, with the decay extending near the gingiva.
The second case report that illustrates the restoration of Considering the extent of the decay and the patient's
two pulpless premolars previously filled with GIC (Glass aesthetic expectations, a lithium disilicate-reinforced glass-
Inomer cement) with two indirect CAD/CAM inlays and ceramic inlay-onlay was fabricated using indirect
onlays using lithium disilicate-reinforced glass-ceramic CAD/CAM technology, in alignment with the principles of
materials the therapeutic gradient.
I. INTRODUCTION
In modern dental practice, the principles of tissue
preservation and therapeutic gradient have become essential,
driven by advancements in digital technology and the
availability of contemporary aesthetic materials. The
introduction of adhesive techniques has facilitated the
adoption of a conservative approach that prioritizes the
preservation of dental tissue, minimizing the need for
extensive peripheral preparation when restoring teeth. The
emergence of minimally invasive aesthetic dentistry has
revolutionized the restoration of devitalized teeth. Even in
the presence of moderate decay, it is now possible to select
root-free prosthetic solutions for these teeth.
Bonded indirect restorations represent a significant Fig 1 Initial state
advancement in restorative dentistry over the past few
decades. They offer numerous advantages in terms of Pre-prosthetic treatment encompasses scaling and root
aesthetics, biology, and biomechanics when restoring the planing procedures, as well as effective oral hygiene
dental structure. Indirect bonded partial restorations (IBCRs) motivation techniques.
can be broadly categorized into two main types: anterior
IBCRs, including veneers and chips, and posterior IBCRs, The preparation phase for prosthetic treatment involves
encompassing inlays, onlays, overlays, veenerlays, and table the removal of irreversibly damaged tissue. A specific
tops. coronal layout is essential to optimize the placement and
longevity of the prosthetic element. The following
parameters should be taken into consideration:
IJISRT23AUG751 www.ijisrt.com 1651
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
The floor and axial walls should feature rounded angles.
Internal walls should exhibit a divergence of at least 10°.
Clear cavo-superficial limits should be established
without the use of bevels.
Occlusal impacts should not coincide with the tooth-
restoration interface.
The main isthmus should have a minimum width of
2mm.
The mesiodistal width of the proximal box must be at
least 1mm.
Restorations should have a minimum thickness of 2mm
at the occlusal groove.
The cervical level should have residual walls with a
minimum width of 2mm, while the occlusal level should
have walls of at least 1mm in width.
Restorative materials should have a thickness of 1.5 to
2mm at the level of covered cusps.
It is recommended to establish a defined limit at the Fig 4 Lithium Disilicate-Reinforced Glass-Ceramic Inlay on
covered cusps, known as a congeal limit. Model
Try in and Bonding :
To evaluate the aesthetic appearance of the inlay-onlay
restoration, a fitting procedure was performed, following a
specific bonding protocol. Initially, a watertight surgical
drape was applied to isolate the tooth, ensuring a dry
working area. The inner surface of the restoration, known as
the denture intrados, was etched using 10% hydrofluoric
acid for 30 seconds and subsequently treated with a silane
coupling agent. Simultaneously, the tooth surface underwent
etching with 37% orthophosphoric acid: 30 seconds on
enamel and 20 seconds on dentin. An adhesive agent was
then applied without light-curing to avoid excessive
thickness. The inlay-onlay prosthesis was carefully placed,
and a dual-setting luting resin, such as Variolink®, was
injected. Each side of the restoration underwent 40 seconds
of light-curing to ensure proper polymerization and bonding
between the prosthesis and the tooth structure.
Fig 2 Proximale Inlay Preparation + Proximal Margin Treatment of Restoration Intrados
Relocation
Fig 5 Application of Hydrofluoric Acid: Chalky White
Appearance
Fig 3 One-Phase Impression
IJISRT23AUG751 www.ijisrt.com 1652
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Fig 6 Silane Application on the Inlay Intrados Fig 9 Bonding
Dental Surface Treatment
Fig 10 Photopolymerization
Control :
Fig 7 Etching with 37% Orthosphoric Acid Followed by After one week's bonding, the dynamic occlusion was
Rinsing and Drying checked and polished.
Fig 8 Adhesive Application Fig 11 Final Result
IJISRT23AUG751 www.ijisrt.com 1653
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Case report 2: moderate-sized occluso-proximal cavities were detected,
A healthy 28-year-old patient consulted the Fixed with the decay extending near the gingival margin.
Prosthodontics Department at the dental clinic in Monastir Considering the extent of decay, the patient's requirements,
to restore two pulpless premolars previously filled with GIC and the therapeutic gradient, the treatment plan involved
(Glass Inomer cement). She has high aesthetic expectations. fabricating two indirect CAD/CAM inlays and onlays using
Endobuccal examination revealed two proximal GIC fillings lithium disilicate-reinforced glass-ceramic materials. In this
on teeth 24 and 25. Occlusion examination showed canine case, it is crucial to perform a cervical margin relocation
protection on both sides without any parafunctional habits. using composite resin to optimize bonding and facilitate the
Smile analysis indicated a generally favorable situation, impression-taking process. This step will enhance the
except for the mesial part of the teeth being uncovered. overall success of the restorations.
Upon removal of the existing fillings on the two premolars,
Fig 12 Initial state
Fig 13 Proximale Inlay Preparation + Proximal Margin
Relocation Fig 15 Lithium Disilicate - Reinforced Glass - Ceramic
Inlay on Model
Fig 16 Application of Hydrofluoric Acid: Chalky White
Fig 14 One-Phase Impression Appearance
IJISRT23AUG751 www.ijisrt.com 1654
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Fig 20 Bonding
Fig 17 Silane Application on the Inlay Intrados
Fig 21 Light-Curing
Fig 22 Final result
Fig 18 Etching with 37% Orthosphoric Acid
II. DISCUSSION
To restore endodontically treated teeth, practitioners
commonly utilize peripheral restorations with or without
posts. In modern dentistry, treatment decisions are guided by
various principles, including the therapeutic gradient,
biomimicry/biocompatibility, tissue preservation, and
adhesion. The selection of the least invasive technique
appropriate for the clinical situation is recommended,
aligning with the principles of tissue sparing and the
therapeutic gradient concept.
Multiple restorative options have been proposed for
pulpless teeth, ranging from the least invasive to the most
invasive approaches. These include direct composite resin
restorations, bonded partial restorations (such as inlay-only,
Fig 19 Adhesive Application overlay, and endocrown), and full-coverage crowns.1
IJISRT23AUG751 www.ijisrt.com 1655
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Direct composite resin restorations are mainly contraindications should be considered, including cases
indicated for teeth with minimal or moderate decay and no where more than half of the tooth structure is missing,
significant discoloration, within a favorable occlusal presence of parafunctional habits, pronounced cuspal
conditions. However, in the presence of a large cavity, the inclination, and anterior teeth.
stresses experienced during polymerization shrinkage of
composites using the direct technique are significant and can The choice of restoration technique and material for
lead to recurrent caries, cracks, or fractures.2,3 endodontically treated teeth should be guided by the extent
of tooth decay. While standardized preparations are no
In those two clinical cases, the loss of substance occurs longer recommended, certain criteria must be respected.
at the expense of a proximal wall with a loss of more than These include ensuring uniform depth and width of the
one-third of the buccolingual width. In such cases, the direct preparation, with a minimum width of 1.5mm for composite
technique cannot be performed primarily due to mechanical restorations and 2mm for ceramic restorations. The cavity
reasons. Therefore, an indirect bonded partial restoration is bottom should be flat, the walls should have a minimum
recommended, which represents an essential aspect of the divergence of 10°, and the preparation profile should have a
modern therapeutic armamentarium in dentistry.4 wide fillet or shoulder with a rounded internal angle. The
peripheral limit of the preparation should be supragingival,
Although limited studies have been conducted on the and the occlusal limit should be located outside the areas of
prognosis of indirect bonded partial restorations for pulpless occlusal impact, whether in the occlusal intercuspal position
teeth, a study by Chrepa et al. involving 31 premolars and or dynamic occlusion.8,9,10,11
158 molars reported a survival rate of 96.8% at 37 months. 5
Cuspidial coverage may be indicated in certain
Bonded inlay-onlays are considered reliable, situations, such as when the thickness of the amelo-dentinal
conservative, modern, and aesthetically pleasing therapeutic wall is less than 1mm occlusally and 2mm cervically after
solutions due to advancements in materials and digital caries removal, when the interocclusal maximum (IOM)
dentistry. Studies have shown a high success rate (90% at 12 occlusion touches the dento-prosthetic joint, when the tooth
years) for bonded inlay-onlays, although failures, despite is pulpless and all cusps need to be covered, when a cusp
their relatively low in rate (1.9%), should not be overlooked. supports a laterally positioned group protection guide, in the
According to Otto's 2017 study, failures in these restorations case of deep cavities that increase the risk of fractures, and
can be attributed to ceramic fracture (65%), tooth fracture when the height/width ratio of a cusp is greater than 1,
(13%), secondary caries (18%), and endodontic problems increasing the risk of fractures below the amelo-cemental
(4%). junction. However, cuspidial coverage should only be
performed when the indication is well-established, as it may
This study found also that inlay-onlay restorations in contradict the principle of tissue economy.9,10 In certain
premolars presented a significantly lower risk compared to situations, fragile residual walls can be preserved using a
molars.6 This finding was consistent with another study that dentin substitute such as hybrid or fluid composite or bulk
also observed a similar pattern.7 However, the analyzed data fill.
did not provide conclusive evidence regarding the specific
reasons behind this discrepancy. It remains unclear whether This technique, known as immediate dentin
this difference is due to technical factors, such as variations sealing (IDS), creating a hybrid layer between the adhesive
in tooth anatomy or load-bearing capacity, or if it is and the demineralized dentin collagen surface after
influenced by better accessibility for treatment or the preparation and before taking the impression. The adhesive
patients' oral hygiene practices.6 Further research is used typically involves a 3-stage pre-etch (MR) (MR3)
warranted to explore these factors and establish a more system, as it provides better water resistance compared to
definitive understanding of the observed variations in risk self-etch systems. IDS offers biological and clinical
between premolars and molars in relation to inlay-onlay advantages, such as eliminating the risk of bacterial
restorations. contamination of dentin, improving adaptation of the
prosthetic part, harmonizing the internal architecture of the
To minimize these complications and failures, it is preparation when performed with a fluid composite, and
essential to carefully consider the indications for this type of reducing post-operative sensitivity in cases of pulpless
restoration, choose the appropriate material, and adhere to teeth.12 Cervical margin elevation involves relocating the
the principles of preparation and bonding protocols. cervical margin to a supragingival level (generally around 1
to 1.5mm) by bonding a plastic phase material to the
Inlays and onlays are particularly useful in situations intrasulcular margin. This technique aims to preserve as
such as substantial loss of substance greater than one-third much tooth tissue as possible and facilitate the registration
of the buccolingual width or loss of a cusp, as well as in Site of preparation contours. Recent studies have shown that this
1-2, stage 3-4 (according to the SisTa classification), and for technique reduces ceramic fractures when the preparation
multiple restorations on the same arch to achieve precise margin is below the enamel-cement junction.13,14
occlusal and proximal contacts, restore the occlusal plane,
maintain satisfactory periodontal and occlusal status, and
accommodate pulp or pulpless teeth with juxta/supragingival
cavities and good oral hygiene. However, several
IJISRT23AUG751 www.ijisrt.com 1656
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Dental restorations can be accomplished using various When selecting a material for dental restoration,
materials, including composites and ceramics. Composite several factors should be considered. The restoration of the
resins are available in two forms: micro-filled and hybrid antagonist tooth is crucial to consider, as it is preferable to
composites. Micro-filled composites pose a risk of fatigue choose the same material for both teeth to ensure similar
overload and intra-material fractures, whereas hybrid wear. The substrate to which the material is bonded is also
composites offer superior mechanical resistance and important, and a material with a modulus of elasticity close
enhanced aesthetic properties. Vitreous matrix ceramics are to that of dental tissue is preferred to ensure similar
commonly employed due to their excellent bonding deformation during functional movements. Glass-ceramic
characteristics. Glass-ceramics enriched with leucite crystals restorations are preferable when bonding to enamel,
or lithium disilicate crystals are suitable for all types of while composite restorations are preferred when bonding to
partial restorations and can be fabricated either by pressing dentin. The presence of parafunctions, such as bruxism, is
from an ingot or through CAD/CAM techniques. 1,15,16 another factor to consider. In such cases, a composite
Lithium disilicate-enriched glass-ceramic inlays-onlays restoration is preferable, as ceramic may break. Composite
demonstrate outstanding performance and reliability, with is also the material of choice for repairs, as it is easy to
estimated survival rates ranging between 92% and 95% at 5 repair and readjust. Patient aesthetic requirements should
years and 91% at 10 years. Nine machinable CAD/CAM also be considered, as ceramic has good optical properties
blocks currently available in the market fall into the and leads to satisfactory aesthetic results compared to
category of "hybrid" materials, including nanoceramic-filled composite. However, if the buccal margin is too visible, a
resins and polymer-infiltrated ceramics.17 composite restoration can be made in the mouth after
bonding. Ceramic remains the most biocompatible
material biologically, with regard to the tissue
microenvironment.16,18
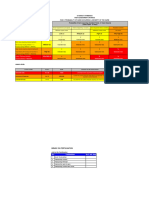
Table 1 Comparison of the Properties of Composites and Ceramics for Partial Single-Tooth Restorations
Parameters Ceramics composites
Ease of clinical procedures + ++
Ease of + +++
Laboratory
Intra-oral repairs and touch-ups Buccal 0 ++
Aesthetics: - short-term +++ +++
- long-term +++ ++
Polishing + ++
Material wear resistance +++ ++
Fragility + ++
Bonding efficiency +++ +
Coefficient of thermal expansion ++ ++
Chemical stability +++ +
Biocompatibility +++ ++
Cost 0 +
III. CONCLUSION [4]. Mondelli J, Sene F, Ramos RP, Benetti AR. Tooth
structure and fracture strength of cavities. Braz Dent J.
Bonded partial restorations can be an alternative 2007;18(2):134-8.
treatment option for moderately decayed teeth. The principle [5]. Chrepa, V.; Konstantinidis, I.; Kotsakis, G.A.; Mitsias,
of tissue preservation should also apply to decayed teeth. M.E. The survival of indirect composite resin onlays
Therefore, the use of a coronal-radicular anchor and for the restoration of root filled teeth: A retrospective
peripheral crown should not be systematic, but reserved for medium-term study. Int. Endod. J. 2014, 47, 967–973.
situations of severe decay, very unfavorable occlusal [6]. Otto T, Schneider D. Long-term clinical results of
contexts, and restorations where the quality of the substrate chairside Cerec CAD/CAM inlays and onlays: a case
would not be compatible with quality. series. Int J Prosthodont. 2008 Jan-Feb;21(1):53-9.
[7]. Reiss B, Clinical results of Cerec inlays in a dental
REFERENCES practice over a period of 18 years. Int J Comp Dent
2006;9:11-22
[1]. Decup F. Inlay, Onlay, Overlay. 2éme. paris.France; [8]. Emmanuel D, Zunzarren R. Evolution des formes de
2022. 83 p. préparation pour inlays/onlays postérieurs à la
[2]. Nandini S. Indirect resin composites. J Conserv Dent. mandibule. Réalités cliniques: revue européenne
2010 Oct;13(4):184-94. d’odontologie. 1 déc 2014;25:317‑26.
[3]. Pizzolotto L, Moraes RR. Resin Composites in
Posterior Teeth: Clinical Performance and Direct
Restorative Techniques. Dent J (Basel). 2022 Nov
27;10(12):222.
IJISRT23AUG751 www.ijisrt.com 1657
Volume 8, Issue 8, August – 2023 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[9]. Posterior indirect adhesive restorations: updated
indications and the Morphology Driven Preparation
Technique [Internet]. Quintessenz Verlags-GmbH.
[cité 15 janv 2023]. Disponible sur: https://www.
quintessence publishing.com/deu/en/article/852288
[10]. Restaurations_indirectes_posterieures.pdf [Internet].
[cité 16 janv 2023]. Disponible sur:
https://www.colibri.ac/wp-
content/uploads/Restaurations_indirectes_posterieures.
[11]. Rocca GT, Rizcalla N, Krejci I, Dietschi D. Evidence-
based concepts and procedures for bonded inlays and
onlays. Part II. Updated guidelines for cavity
preparation and restoration fabrication. CLINICAL
RESEARCH. 2015;10(3).
[12]. Hardan L, Devoto W, Bourgi R, Cuevas-Suárez CE,
Lukomska-Szymanska M, Fernández-Barrera MÁ, et
al. Immediate Dentin Sealing for Adhesive
Cementation of Indirect Restorations: A Systematic
Review and Meta-Analysis. Gels. mars 2022;8(3):175.
[13]. Samartzi TK, Papalexopoulos D, Ntovas P, Rahiotis C,
Blatz MB. Deep Margin Elevation: A Literature
Review. Dent J (Basel). 14 mars 2022;10(3):48.
[14]. Vertolli T, Martinsen B, Hanson C, Howard R,
Kooistra S, Ye L. Effect of Deep Margin Elevation on
CAD/CAM-Fabricated Ceramic Inlays. Operative
Dentistry. 3 avr 2020;45(6):608‑17.
[15]. Ma L, Guess PC, Zhang Y. Load-bearing properties of
minimal-invasive monolithic lithium disilicate and
zirconia occlusal onlays: finite element and theoretical
analyses. Dent Mater. juill 2013;29(7):742‑51.
[16]. Fan J, Xu Y, Si L, Li X, Fu B, Hannig M. Long-term
Clinical Performance of Composite Resin or Ceramic
Inlays, Onlays, and Overlays: A Systematic Review
and Meta-analysis. Operative Dentistry. 21 avr
2021;46(1):25‑44.
[17]. Yoon HI, Sohn PJ, Jin S, Elani H, Lee SJ. Fracture
Resistance of CAD/CAM-Fabricated Lithium
Disilicate MOD Inlays and Onlays with Various Cavity
Preparation Designs: Fracture Resistance of
CAD/CAM Lithium Disilicate. Journal of
Prosthodontics. févr 2019;28(2):e524‑9.
[18]. Randomized Clinical Trial of Indirect Resin Composite
and Ceramic Veneers: Up to 3-year Follow-up. The
Journal of Adhesive Dentistry. 1 mai
2013;15(2):181‑90.
IJISRT23AUG751 www.ijisrt.com 1658
You might also like
- Consumers Are People Too - FrogDocument36 pagesConsumers Are People Too - FrogMalek El BéjiNo ratings yet
- Immediate Dental Implant Placement Into Infected vs. Non-Infected Sockets: A Meta-AnalysisDocument7 pagesImmediate Dental Implant Placement Into Infected vs. Non-Infected Sockets: A Meta-Analysismarlene tamayoNo ratings yet
- Injection Overmolding For Aesthetics and Strength Part 2Document4 pagesInjection Overmolding For Aesthetics and Strength Part 2The Bioclear ClinicNo ratings yet
- Ultrasonic Periodontal Debridement: Theory and TechniqueFrom EverandUltrasonic Periodontal Debridement: Theory and TechniqueRating: 2.5 out of 5 stars2.5/5 (2)
- Exhibitor List 2019: Company Name Booth No. CountryDocument8 pagesExhibitor List 2019: Company Name Booth No. CountryBojana Dekic0% (1)
- Giuseppe-Marchetti-Composite-inlays-and-onlays-via-www.styleitaliano.orgDocument18 pagesGiuseppe-Marchetti-Composite-inlays-and-onlays-via-www.styleitaliano.orgBogdanŢimiraşNo ratings yet
- All Ceramic Inlay: A Case ReportDocument6 pagesAll Ceramic Inlay: A Case ReportIlsen ManzanillaNo ratings yet
- CADCAM Vs Traditional Ceramic InlayDocument10 pagesCADCAM Vs Traditional Ceramic InlayAya Ibrahim YassinNo ratings yet
- Direct Cuspal-Coverage Posterior Resin Composite Restorations: A Case ReportDocument8 pagesDirect Cuspal-Coverage Posterior Resin Composite Restorations: A Case ReportDinar ArdhananeswariNo ratings yet
- Ferrule PDFDocument7 pagesFerrule PDFVidya SenthuNo ratings yet
- Posterior Composite Restoration UpdateDocument10 pagesPosterior Composite Restoration UpdateBianca IovoaiaNo ratings yet
- Ceramics in Dentistry-Part I: Classes of MaterialsDocument6 pagesCeramics in Dentistry-Part I: Classes of MaterialsDilesh PradhanNo ratings yet
- Ceramic Inlay PreparationDocument9 pagesCeramic Inlay PreparationRaghu PratapNo ratings yet
- Esthetic Technique: Crown Considerations, Preparations, and Material Selection For Esthetic Metal-Ceramic RestorationsDocument16 pagesEsthetic Technique: Crown Considerations, Preparations, and Material Selection For Esthetic Metal-Ceramic RestorationsAyu Nur A'IniNo ratings yet
- Inlay OnlayDocument6 pagesInlay OnlayNur HayatiNo ratings yet
- IJEDe 15 03 Rocca 852 2Document22 pagesIJEDe 15 03 Rocca 852 2hannaly estradaNo ratings yet
- Eur JEsthet Dent 2013 MeyenbergDocument97 pagesEur JEsthet Dent 2013 Meyenbergsoma kiranNo ratings yet
- Clin DSDDocument5 pagesClin DSDAlfred OrozcoNo ratings yet
- INLAYDocument11 pagesINLAYMira AnggrianiNo ratings yet
- Aesthetic Rehab Visagism ConceptDocument7 pagesAesthetic Rehab Visagism ConceptvaamdevaaNo ratings yet
- Zucchelli Masterclass Course Program 2020Document11 pagesZucchelli Masterclass Course Program 2020ComarzzoNo ratings yet
- Cosmetic Dentistry CSD 2013Document3 pagesCosmetic Dentistry CSD 2013Rodrigo Daniel Vela RiveraNo ratings yet
- Vertical Ridge Augmentation and Soft Tissue Reconstruction of The Anterior Atrophic Maxillae - Urban2017Document12 pagesVertical Ridge Augmentation and Soft Tissue Reconstruction of The Anterior Atrophic Maxillae - Urban2017Claudio GuzmanNo ratings yet
- Dental ImplantsDocument9 pagesDental ImplantsPati Villalobos AntibiloNo ratings yet
- All Ceramic 5p PDFDocument6 pagesAll Ceramic 5p PDFWiwin Nuril FalahNo ratings yet
- Bulk Fill Composites For Class II Restorations by DentistryDocument12 pagesBulk Fill Composites For Class II Restorations by Dentistryddmorar486No ratings yet
- MagnificationDocument52 pagesMagnificationSiva KumarNo ratings yet
- Mclaren Smile AnalysisDocument15 pagesMclaren Smile AnalysisXavier Vargas PerezNo ratings yet
- The Endocrown - A Different Type of All-Ceramic Reconstruction For Molars - JcdaDocument10 pagesThe Endocrown - A Different Type of All-Ceramic Reconstruction For Molars - Jcdaabcder1234No ratings yet
- The International Journal of Periodontics & Restorative DentistryDocument10 pagesThe International Journal of Periodontics & Restorative Dentistrykevin1678No ratings yet
- Develop Lingual OrtoDocument68 pagesDevelop Lingual OrtoOrtodonti UnhasNo ratings yet
- Biologic Interfaces in Esthetic Dentistry Part IIDocument27 pagesBiologic Interfaces in Esthetic Dentistry Part IINoelia MadrizNo ratings yet
- Enrico Cassai The WORKING LENGTHDocument9 pagesEnrico Cassai The WORKING LENGTHAnca MartinoviciNo ratings yet
- 547792129c17bec4c106ead404e0c4ddDocument52 pages547792129c17bec4c106ead404e0c4ddHugoRoCkstarNo ratings yet
- Deliperi S - PPAD - 2005 PDFDocument9 pagesDeliperi S - PPAD - 2005 PDFAlfredo PortocarreroNo ratings yet
- Afraccion PDFDocument9 pagesAfraccion PDFzayraNo ratings yet
- AnyRidge EngwebDocument128 pagesAnyRidge EngwebPinky Tolani100% (1)
- HTTP WWW - Styleitaliano.org Esthetic Dentistry in PaediatricsDocument9 pagesHTTP WWW - Styleitaliano.org Esthetic Dentistry in PaediatricsAmee PatelNo ratings yet
- Course 2 Jordi Anna 2018 Brochure 1Document6 pagesCourse 2 Jordi Anna 2018 Brochure 1mhd ssaghNo ratings yet
- Telescopic Dentures: An Overlooked TechnologyDocument3 pagesTelescopic Dentures: An Overlooked TechnologyarchanglsNo ratings yet
- Noncarious Cervical Lesions As Abfraction Etiology Diagnosis and Treatmentmodalities of Lesions A Review Article 2161 1122 1000438 PDFDocument6 pagesNoncarious Cervical Lesions As Abfraction Etiology Diagnosis and Treatmentmodalities of Lesions A Review Article 2161 1122 1000438 PDFFaniaNo ratings yet
- Ultimate Ceramic Veneers A Laboratory-Guided Ultraconservative PreparationDocument15 pagesUltimate Ceramic Veneers A Laboratory-Guided Ultraconservative PreparationEvelina HaddadienNo ratings yet
- Zirconia in Dentistry Part 2. Evidence-BDocument33 pagesZirconia in Dentistry Part 2. Evidence-Bt723849No ratings yet
- EJED2 Dietschi 329Document18 pagesEJED2 Dietschi 329Alexis Alberto Rodríguez Jiménez100% (1)
- Posterior Indirect AdhesiveDocument34 pagesPosterior Indirect AdhesiveAlondra CevallosNo ratings yet
- Digital Smile Design: A Tool For Treatment Planning and Communication in Esthetic DentistryDocument10 pagesDigital Smile Design: A Tool For Treatment Planning and Communication in Esthetic Dentistrygilberto69No ratings yet
- 3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFDocument10 pages3c. The Effect of A Fiber Reinforced Cavity Configuration On Load Bearing Capacity and Failure Mode of Endodontically Treated Molars Restored With CAD-CAM Resin Composite Overlay Restorations PDFAnisha AnilNo ratings yet
- Aesthetic Evolution - 7 Lessons of Indirect RestorationDocument10 pagesAesthetic Evolution - 7 Lessons of Indirect RestorationAndreea StaicuNo ratings yet
- Casebook IconVE 07022019 enDocument45 pagesCasebook IconVE 07022019 envanity fairNo ratings yet
- Criteria For The Selection of Restoration Materials PDFDocument8 pagesCriteria For The Selection of Restoration Materials PDFSofia BoteroNo ratings yet
- 2 - Evaluation of Bond Strength and Thickness of Adhesive Layer According To The Techniques of Applying Adhesives in Composite Resin RestorationsDocument7 pages2 - Evaluation of Bond Strength and Thickness of Adhesive Layer According To The Techniques of Applying Adhesives in Composite Resin RestorationskochikaghochiNo ratings yet
- Orhan 2021 (Book) - Ultrasonography in Dentomaxillofacial Diagnostics - SpringerDocument372 pagesOrhan 2021 (Book) - Ultrasonography in Dentomaxillofacial Diagnostics - SpringerlagianggenNo ratings yet
- Nanofilled Resin Composite Properties and Clinical Performance - A ReviewDocument18 pagesNanofilled Resin Composite Properties and Clinical Performance - A ReviewInside Dentistry educationNo ratings yet
- Digital Smile Design - Predictable Results (#741934) - 1117267Document6 pagesDigital Smile Design - Predictable Results (#741934) - 1117267yuumiNo ratings yet
- Clinical Tips: 25 For General PracticeDocument6 pagesClinical Tips: 25 For General PracticethiatuslNo ratings yet
- CDA June 2021 Journal - ISSUU - 060121Document56 pagesCDA June 2021 Journal - ISSUU - 060121abdulaziz alzaidNo ratings yet
- Advantages of Adhesive in DentistryDocument29 pagesAdvantages of Adhesive in DentistryAnonymous CY62A9No ratings yet
- Microsurgery in EndodonticsFrom EverandMicrosurgery in EndodonticsSyngcuk KimNo ratings yet
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionFrom EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNo ratings yet
- Analysis of Opaque, Peel-Off and Flex Rejects in the Electro Plating Process Using the Six Sigma Dmaic MethodDocument18 pagesAnalysis of Opaque, Peel-Off and Flex Rejects in the Electro Plating Process Using the Six Sigma Dmaic MethodInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Study to Effect of Reminiscence Therapy on Psychological Well-Being among Elderly Residing in Selected Old Age HomeDocument5 pagesA Study to Effect of Reminiscence Therapy on Psychological Well-Being among Elderly Residing in Selected Old Age HomeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Application of Project Management using CPM (Critical Path Method) and Pert (Project Evaluation and Review Technique) in the Nava House Bekasi Cluster Housing Development ProjectDocument12 pagesApplication of Project Management using CPM (Critical Path Method) and Pert (Project Evaluation and Review Technique) in the Nava House Bekasi Cluster Housing Development ProjectInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Comprehensive Review on the Therapeutic Potential of PectinDocument6 pagesA Comprehensive Review on the Therapeutic Potential of PectinInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Application of the Economic Order Quantity (EOQ) Method on the Supply of Chemical Materials in the Laboratory of PT. Fajar Surya Wisesa TbkDocument15 pagesApplication of the Economic Order Quantity (EOQ) Method on the Supply of Chemical Materials in the Laboratory of PT. Fajar Surya Wisesa TbkInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Rare Complication: Cardiac Arrest and Pulmonary Embolism in Polyarteritis NodosaDocument5 pagesA Rare Complication: Cardiac Arrest and Pulmonary Embolism in Polyarteritis NodosaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Integrated Border Security System on Human Trafficking in Bangladesh: The Mediating Effect of the Use of Advanced TechnologyDocument12 pagesThe Impact of Integrated Border Security System on Human Trafficking in Bangladesh: The Mediating Effect of the Use of Advanced TechnologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Quality Control to Reduce Appearance Defects at PT. Musical InstrumentDocument11 pagesQuality Control to Reduce Appearance Defects at PT. Musical InstrumentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Forecasting PM10 Concentrations Using Artificial Neural Network in Imphal CityDocument10 pagesForecasting PM10 Concentrations Using Artificial Neural Network in Imphal CityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analysis of Carton Packaging Quality Control Using Statistical Quality Control Methods at PT XYZDocument10 pagesAnalysis of Carton Packaging Quality Control Using Statistical Quality Control Methods at PT XYZInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Quizlet's Usefulness for Vocabulary Learning: Perceptions of High-Level and Low-Level Chinese College EFL LearnersDocument5 pagesQuizlet's Usefulness for Vocabulary Learning: Perceptions of High-Level and Low-Level Chinese College EFL LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Enhancing Estimating the Charge Level in Electric Vehicles: Leveraging Force Fluctuation and Regenerative Braking DataDocument6 pagesEnhancing Estimating the Charge Level in Electric Vehicles: Leveraging Force Fluctuation and Regenerative Braking DataInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Entrepreneurial Adult Education as a Catalyst for Youth Employability in Disadvantaged AreasDocument9 pagesEntrepreneurial Adult Education as a Catalyst for Youth Employability in Disadvantaged AreasInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Role of Leadership Training in Developing Effective Police SupervisorsDocument17 pagesThe Role of Leadership Training in Developing Effective Police SupervisorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Health Care - An Android Application Implementation and Analyzing user Experience Using PythonDocument7 pagesHealth Care - An Android Application Implementation and Analyzing user Experience Using PythonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Intrusion Detection System with Ensemble Machine Learning Approaches using VotingClassifierDocument4 pagesIntrusion Detection System with Ensemble Machine Learning Approaches using VotingClassifierInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Synthetic and Natural Vitamin C Modulation of Leaded Paint-Induced Nephrotoxicity of Automobile Painters in Ile-Ife, Nigeria.Document21 pagesSynthetic and Natural Vitamin C Modulation of Leaded Paint-Induced Nephrotoxicity of Automobile Painters in Ile-Ife, Nigeria.International Journal of Innovative Science and Research TechnologyNo ratings yet
- Visitor Perception Related to the Quality of Service in Todo Tourism VillageDocument10 pagesVisitor Perception Related to the Quality of Service in Todo Tourism VillageInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Gravity Investigations Applied to the Geological Framework Study of the Mambasa Territory in Democratic Republic of CongoDocument9 pagesGravity Investigations Applied to the Geological Framework Study of the Mambasa Territory in Democratic Republic of CongoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Developing Digital Fluency in Early Education: Narratives of Elementary School TeachersDocument11 pagesDeveloping Digital Fluency in Early Education: Narratives of Elementary School TeachersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A New Model of Rating to Evaluate Start-ups in Emerging Indian MarketDocument7 pagesA New Model of Rating to Evaluate Start-ups in Emerging Indian MarketInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Proof of Concept Using BLE to Optimize Patients Turnaround Time (PTAT) in Health CareDocument14 pagesA Proof of Concept Using BLE to Optimize Patients Turnaround Time (PTAT) in Health CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Financial Prudence as Determinant of Employees’ Interest in Graduate StudyDocument13 pagesFinancial Prudence as Determinant of Employees’ Interest in Graduate StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design and Implementation of Software-Defined ReceiverDocument8 pagesDesign and Implementation of Software-Defined ReceiverInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Optimizing Bio-Implant Materials for Femur Bone Replacement:A Multi-Criteria Analysis and Finite Element StudyDocument5 pagesOptimizing Bio-Implant Materials for Femur Bone Replacement:A Multi-Criteria Analysis and Finite Element StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Crop Monitoring System with Water Moisture Levels Using ControllerDocument8 pagesCrop Monitoring System with Water Moisture Levels Using ControllerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Inclusive Leadership in the South African Police Service (SAPS)Document26 pagesInclusive Leadership in the South African Police Service (SAPS)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Naturopathic Approaches to Relieving Constipation: Effective Natural Treatments and TherapiesDocument9 pagesNaturopathic Approaches to Relieving Constipation: Effective Natural Treatments and TherapiesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fahfi/Mochaina Illegal Gambling Activities and its Average Turnover within Limpopo ProvinceDocument8 pagesFahfi/Mochaina Illegal Gambling Activities and its Average Turnover within Limpopo ProvinceInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Year Wise Analysis and Prediction of Gold RatesDocument8 pagesYear Wise Analysis and Prediction of Gold RatesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Vegan LifeDocument116 pagesVegan Lifepelouse23100% (12)
- Female GenitaliaDocument96 pagesFemale GenitaliaJopaii TanakaNo ratings yet
- Materia Medica For Students Part I Ritu Kinra.00247 2introductionDocument5 pagesMateria Medica For Students Part I Ritu Kinra.00247 2introductionRohini Chaudhari33% (3)
- Revision Test 4 - Class 12D1 2021-2022Document7 pagesRevision Test 4 - Class 12D1 2021-2022Tenebrae LuxNo ratings yet
- HIRARC On Fertilisation - SI - 2022Document6 pagesHIRARC On Fertilisation - SI - 2022noor khairaniNo ratings yet
- Mark Keterangan: Acuan Perencanaan Alat Kesehatan Kode Rs 3216441 Form f3Document18 pagesMark Keterangan: Acuan Perencanaan Alat Kesehatan Kode Rs 3216441 Form f3igdNo ratings yet
- Kenya Basic Education Covid - 19 Emergency Response PlanDocument53 pagesKenya Basic Education Covid - 19 Emergency Response Planh3493061No ratings yet
- 1340701015binder2Document39 pages1340701015binder2CoolerAdsNo ratings yet
- List of Subject CodesDocument1 pageList of Subject CodesAnonymous YooNo ratings yet
- En Manu RVDocument90 pagesEn Manu RVMurat CanNo ratings yet
- New Wordpad DocumentDocument41 pagesNew Wordpad DocumentSherwin TuckerNo ratings yet
- PopipDocument2 pagesPopipRaj Kumar KNo ratings yet
- 1 RT08 Occupational Exposure WEBDocument87 pages1 RT08 Occupational Exposure WEBRichar Pinedo CadilloNo ratings yet
- Level 12 Analogies 2 PDFDocument3 pagesLevel 12 Analogies 2 PDFCarlson AberinNo ratings yet
- Ies RDocument3 pagesIes RNikoleta HirleaNo ratings yet
- Brief Introduction To HospitalDocument11 pagesBrief Introduction To Hospitalkanika jainNo ratings yet
- 2 Risk Identification FormDocument6 pages2 Risk Identification FormkamranNo ratings yet
- Predisposing Factor of Fungal InfectionDocument13 pagesPredisposing Factor of Fungal InfectionDitha RizkyNo ratings yet
- Medicaid Edit CodesDocument79 pagesMedicaid Edit CodesNeil GilstrapNo ratings yet
- August 7, 2015 Strathmore Times PDFDocument28 pagesAugust 7, 2015 Strathmore Times PDFStrathmore TimesNo ratings yet
- Medical Passport - Enteral NutritionDocument4 pagesMedical Passport - Enteral NutritionDovlet AmanovNo ratings yet
- Unilateral Neglect: Assessment and Rehabilitation: Richard P. Conti, Jacqueline M. ArnoneDocument10 pagesUnilateral Neglect: Assessment and Rehabilitation: Richard P. Conti, Jacqueline M. Arnonejerrin jacobNo ratings yet
- Case Report 2Document2 pagesCase Report 2respikNo ratings yet
- Safety Alert - Grinder WheelDocument3 pagesSafety Alert - Grinder WheelsarojNo ratings yet
- CGSM Form No. 1 Community SurveyDocument3 pagesCGSM Form No. 1 Community SurveyJulia PicoNo ratings yet
- Latent Autoimmune Diabetes in Adults TDDocument3 pagesLatent Autoimmune Diabetes in Adults TDapi-648595816No ratings yet
- Nursing Responsibilities For METRONIDAZOLEDocument1 pageNursing Responsibilities For METRONIDAZOLEIsrael Soria Espero63% (8)
- Lesson Plan in Health IV JonaDocument8 pagesLesson Plan in Health IV JonaJenelyn Limen100% (1)