Download as docx, pdf, or txt
You might also like
- Drug Study On Emergency DrugsDocument14 pagesDrug Study On Emergency DrugsRene John FranciscoNo ratings yet
- Drug Study TramadolDocument14 pagesDrug Study TramadolBianca Freya Porral85% (13)
- Analytical Method Validation PDFDocument19 pagesAnalytical Method Validation PDFroxaniqu100% (1)
- Pharmacology - Chapter 29Document5 pagesPharmacology - Chapter 29Ashley-Michelle LewisNo ratings yet
- Nursing Responsibilities For METRONIDAZOLEDocument1 pageNursing Responsibilities For METRONIDAZOLEIsrael Soria Espero63% (8)
- Metoclopromide Drug StudyDocument4 pagesMetoclopromide Drug Studymarklesterdeguzman087No ratings yet
- Dextroamphetamine: Brand Name: DexedrineDocument23 pagesDextroamphetamine: Brand Name: DexedrineSharry Fe OasayNo ratings yet
- Dextroamphetamine: Brand Name: DexedrineDocument23 pagesDextroamphetamine: Brand Name: DexedrineSharry Fe OasayNo ratings yet
- ImipramineDocument6 pagesImipramineMuhammed Faruk JambazNo ratings yet
- Drug Study 1Document10 pagesDrug Study 1neeraj chauhanNo ratings yet
- Drugs For EmergencyDocument25 pagesDrugs For EmergencyJunathan L. DelgadoNo ratings yet
- Drug Study CardinalDocument21 pagesDrug Study CardinalDrei LanuzoNo ratings yet
- DRUGSTUDY TramadolDocument3 pagesDRUGSTUDY TramadolMicaela Andrea CieloNo ratings yet
- Paracetamol Use GuideDocument13 pagesParacetamol Use GuideShashiprakash KshatriyaNo ratings yet
- Fluvoxamine MaleateDocument3 pagesFluvoxamine MaleateHilman Fitriaji Suganda PrawiraNo ratings yet
- Prescribing InformationDocument9 pagesPrescribing InformationasdwasdNo ratings yet
- 01-Tramadol Guidelines PDFDocument1 page01-Tramadol Guidelines PDFDina Aulia FakhrinaNo ratings yet
- Drug StudyDocument7 pagesDrug Studykristen_ramos_3No ratings yet
- TramadolDocument1 pageTramadolBbhie AntiguaNo ratings yet
- ZOMORPH Capsules 10mgDocument6 pagesZOMORPH Capsules 10mgFlorexan Malanday PasonNo ratings yet
- Symph A To Mimetic SDocument27 pagesSymph A To Mimetic Sjl frusaNo ratings yet
- Lyks - Part 7 Drug StudyDocument6 pagesLyks - Part 7 Drug StudyLuige AvilaNo ratings yet
- Calpol Tablets Oral Suspension and Paediatric DropsDocument13 pagesCalpol Tablets Oral Suspension and Paediatric DropsMiscrit ManNo ratings yet
- Citalopramhydrobromide CelexaDocument3 pagesCitalopramhydrobromide CelexaKristi Wray100% (1)
- Drug Study 2Document8 pagesDrug Study 2rey_tengNo ratings yet
- TemazepamDocument1 pageTemazepamCris TanNo ratings yet
- Last PartDocument12 pagesLast PartAira Shane MargesNo ratings yet
- Drug Study Tramadol HydrochlorideDocument1 pageDrug Study Tramadol HydrochlorideSEAN PATRICK SILADANNo ratings yet
- The 10 Most Common Emergency DrugsDocument28 pagesThe 10 Most Common Emergency DrugsKrishna BalsarzaNo ratings yet
- Lisinopril PDFDocument3 pagesLisinopril PDFHannaNo ratings yet
- EMERGENCY DRUGS: A Drug StudyDocument39 pagesEMERGENCY DRUGS: A Drug StudyJenny Rose GriñoNo ratings yet
- Drug Study ArraDocument5 pagesDrug Study ArraPaul ManaloNo ratings yet
- DiarryDocument10 pagesDiarryVan Ryan CondenoNo ratings yet
- V. Norepinephrine &dopamine ReuptakeDocument2 pagesV. Norepinephrine &dopamine ReuptakeChristine Pialan SalimbagatNo ratings yet
- Ketamine Guidelines Feb 05Document3 pagesKetamine Guidelines Feb 05AdiAri RosiuNo ratings yet
- V. Atypical AntipsychoticsDocument2 pagesV. Atypical AntipsychoticsChristine Pialan SalimbagatNo ratings yet
- Drug StudyDocument10 pagesDrug Studytamtam_antonioNo ratings yet
- Psych DrugsDocument6 pagesPsych DrugsdianneingusanNo ratings yet
- Adult: IV: Bradycardia PoisoningDocument28 pagesAdult: IV: Bradycardia PoisoningArthur William Tell BarbaNo ratings yet
- Amiodarone Hydro ChlorideDocument4 pagesAmiodarone Hydro Chlorideapi-3797941No ratings yet
- Clonazepam (Drug Study) - WWW - RNpediaDocument2 pagesClonazepam (Drug Study) - WWW - RNpediaFranz.thenurse6888100% (3)
- DiazepamDocument5 pagesDiazepamapi-3797941No ratings yet
- Antispastics Emtyaz FDocument57 pagesAntispastics Emtyaz FMuhammed MuhsinNo ratings yet
- DolcetDocument3 pagesDolcetConn_Casipe_8158100% (4)
- Drug Study On Emergency DrugsDocument14 pagesDrug Study On Emergency Drugsjcarysuitos100% (4)
- High Alert MedicationsDocument17 pagesHigh Alert MedicationsJoanna Marie Datahan EstomoNo ratings yet
- Actifed DM Cough SyrupDocument10 pagesActifed DM Cough SyrupAnjeliNo ratings yet
- Ketorolac TromethamineDocument4 pagesKetorolac TromethamineSebastian CruzNo ratings yet
- Pil - Ma032 06401Document7 pagesPil - Ma032 06401ntecbd1No ratings yet
- Nortriptyline Tablets Prescribing InformationDocument10 pagesNortriptyline Tablets Prescribing InformationMirza MarufNo ratings yet
- Lovastatin PDFDocument3 pagesLovastatin PDFHannaNo ratings yet
- ANALSIKDocument4 pagesANALSIKDianpratiwi22No ratings yet
- Psychopharmacology in PsychiatryDocument94 pagesPsychopharmacology in PsychiatryOslo Saputra100% (1)
- Drugs Used in The Management of Pain: Non Opioid AnalgesicsDocument6 pagesDrugs Used in The Management of Pain: Non Opioid Analgesicstesfamichael mengistuNo ratings yet
- WEEK2 Course Task (ALFEREZ, DINIELA)Document4 pagesWEEK2 Course Task (ALFEREZ, DINIELA)DINIELA ALLAINE ALFEREZNo ratings yet
- TRAMADOLDocument2 pagesTRAMADOLzimmerstyle09No ratings yet
- Medical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcFrom EverandMedical Encyclopedia XXL: Prof. J.P. Schadé, M.D., Ph.D. D.Sc.hcNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Psychotropic Medications Questions You Should Ask Your 37th Psychiatric Consultation William R. Yee M.D., J.D., Copyright Applied for October 16th, 2022: 3rd editionFrom EverandPsychotropic Medications Questions You Should Ask Your 37th Psychiatric Consultation William R. Yee M.D., J.D., Copyright Applied for October 16th, 2022: 3rd editionNo ratings yet
- Fast Facts: Ottimizzazione del trattamento delle fluttuazioni motorie nella malattia di ParkinsonFrom EverandFast Facts: Ottimizzazione del trattamento delle fluttuazioni motorie nella malattia di ParkinsonNo ratings yet
- Introduction and Evaluation of Pharmacovigilance For BeginnersDocument8 pagesIntroduction and Evaluation of Pharmacovigilance For BeginnersShaun MerchantNo ratings yet
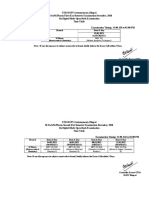
- UTD-RGPV (Autonomous), Bhopal M.Tech/M.Pharm First (Ex) Semester Examination December, 2020 On Digital Mode Open Book Examination Time Table Examination Timing: 11:00 AM To 02:00 PMDocument3 pagesUTD-RGPV (Autonomous), Bhopal M.Tech/M.Pharm First (Ex) Semester Examination December, 2020 On Digital Mode Open Book Examination Time Table Examination Timing: 11:00 AM To 02:00 PMkarishi mehraNo ratings yet
- Ebook How The FDA Trains and Prepares InvestigatorsDocument46 pagesEbook How The FDA Trains and Prepares InvestigatorsNitin JainNo ratings yet
- Con 475306Document24 pagesCon 475306Jagdish ChanderNo ratings yet
- Kelapa Kopyor InternDocument7 pagesKelapa Kopyor InternPutri Amalia IsnainiNo ratings yet
- PharmacistDocument3 pagesPharmacistasakura95No ratings yet
- ECA Annex11 CompSysDocument6 pagesECA Annex11 CompSysNitin KashyapNo ratings yet
- 藥理表格Document26 pages藥理表格林盈孜No ratings yet
- 2017 - The Impact of Halloysite On The Thermo-Mechanical Properties of Polymer CompositesDocument20 pages2017 - The Impact of Halloysite On The Thermo-Mechanical Properties of Polymer CompositesSubramani PichandiNo ratings yet
- Kevin M O'saugnesi: Tavi 24 Arteriuli Hipertenzia, Stenokardia, Miokardiumis Infarqti Da Gulis UkmarisobaDocument47 pagesKevin M O'saugnesi: Tavi 24 Arteriuli Hipertenzia, Stenokardia, Miokardiumis Infarqti Da Gulis UkmarisobaTamari AbesadzeNo ratings yet
- 7: Calculation of Doses: General Considerations: Practice ProblemsDocument9 pages7: Calculation of Doses: General Considerations: Practice ProblemsAashna LambaNo ratings yet
- Participating Vendor ListDocument119 pagesParticipating Vendor ListWWaahhiidd KhanNo ratings yet
- Insulin Infusion Protocol LaborDocument4 pagesInsulin Infusion Protocol LaborJohb CaballeroNo ratings yet
- Enrofloxacin: Therapeutic ReviewDocument4 pagesEnrofloxacin: Therapeutic ReviewAndi Dytha Pramitha SamNo ratings yet
- Organization of Hospital PharmacyDocument27 pagesOrganization of Hospital PharmacyMisty CheifNo ratings yet
- Prometric Questions: Reviewed By:dr - Mohamed Soliman Call: +201016640110Document215 pagesPrometric Questions: Reviewed By:dr - Mohamed Soliman Call: +201016640110Mallu StreamerNo ratings yet
- Medicinal Benefits of Tamarindus Indica by Pharm Safiya A ShehuDocument14 pagesMedicinal Benefits of Tamarindus Indica by Pharm Safiya A ShehuYPS NetworkNo ratings yet
- GEA Niro Mixing and Granulation TechnologyDocument16 pagesGEA Niro Mixing and Granulation Technologychien_yu_leeNo ratings yet
- Vestibular Causes of DizzinessDocument5 pagesVestibular Causes of DizzinessEcaterina ChiriacNo ratings yet
- Session 1: Introduction To Pharmaceutical Dosage Forms: by NTENGO, Venance Wilfred Bpharm K's Royal CollegeDocument27 pagesSession 1: Introduction To Pharmaceutical Dosage Forms: by NTENGO, Venance Wilfred Bpharm K's Royal CollegeVenance NtengoNo ratings yet
- Mission and PrefaceDocument6 pagesMission and Prefacemehrdarou.qaNo ratings yet
- Antibiotic IDocument9 pagesAntibiotic Iglorija71No ratings yet
- Alternative Microbiological Sampling Methods For Nonsterile Inhaled and Nasal ProductsDocument2 pagesAlternative Microbiological Sampling Methods For Nonsterile Inhaled and Nasal ProductsThomas Niccolo Filamor ReyesNo ratings yet
- PsychDocument6 pagesPsychNooneNo ratings yet
- Pharmaceutical MarketingDocument5 pagesPharmaceutical MarketingRahel StormNo ratings yet
- Concept of CRDDSDocument13 pagesConcept of CRDDSNirali DongaNo ratings yet
- OB Drug Study - CephalexinDocument2 pagesOB Drug Study - CephalexinJustin AncogNo ratings yet
- IV Manual 7th Edition July 2020Document175 pagesIV Manual 7th Edition July 2020Deena AlJawamisNo ratings yet