Download as pdf or txt
You might also like
- How To Unlearn Your Pain - PositiveHealth PDFDocument5 pagesHow To Unlearn Your Pain - PositiveHealth PDFEloy Vargas100% (1)
- DR Henry G Bieler Lines of Defense Against DiseaseDocument6 pagesDR Henry G Bieler Lines of Defense Against DiseasebonifacesilveiraNo ratings yet
- Lpca Professional Disclosure Statement - J JonesDocument2 pagesLpca Professional Disclosure Statement - J Jonesapi-316369725100% (1)
- Metastatic Renal Cell Carcinoma in A Child: 11-Year Disease-Free Survival Following SurgeryDocument4 pagesMetastatic Renal Cell Carcinoma in A Child: 11-Year Disease-Free Survival Following SurgerySarly FebrianaNo ratings yet
- Mixed Malignant Germ Cell Tumour of The Lateral Ventricle in An 8-Month-Old Girl: Case Report and Review of The LiteratureDocument4 pagesMixed Malignant Germ Cell Tumour of The Lateral Ventricle in An 8-Month-Old Girl: Case Report and Review of The LiteratureEslam KandilNo ratings yet
- Unknown Primary Cancer of The Head and Neck - A MultidisciplinaryDocument10 pagesUnknown Primary Cancer of The Head and Neck - A MultidisciplinaryFreddy Eduardo Navarro BautistaNo ratings yet
- 2012 Renal Cell Carcinoma Metastasizing To Larynx A Case ReportDocument5 pages2012 Renal Cell Carcinoma Metastasizing To Larynx A Case ReportAlfonsoSánchezNo ratings yet
- Dacheng Jin 2020Document5 pagesDacheng Jin 2020Nehemias MD GuevaraNo ratings yet
- Adenoid Cystic Carcinoma of The Head and NeckDocument4 pagesAdenoid Cystic Carcinoma of The Head and Neckcleric25No ratings yet
- Publications 011Document4 pagesPublications 011utamiNo ratings yet
- F0605yDocument6 pagesF0605ySetiaty PandiaNo ratings yet
- Updates and Management Algorithm For Neuroendocrine Tumors of The Uterine CervixDocument10 pagesUpdates and Management Algorithm For Neuroendocrine Tumors of The Uterine CervixdosiNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument22 pagesInternational Journal of Pediatric OtorhinolaryngologyDear Farah SielmaNo ratings yet
- Carcinoma ParatiroideoDocument10 pagesCarcinoma Paratiroideodavid villamilNo ratings yet
- Follicular Dendritic Cell Sarcoma of The Tonssilar About A CaseDocument4 pagesFollicular Dendritic Cell Sarcoma of The Tonssilar About A CaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Updates and Management Algorithm For Neuroendocrine Tumors of The Uterine CervixDocument10 pagesUpdates and Management Algorithm For Neuroendocrine Tumors of The Uterine Cervixa20320700No ratings yet
- Article Oesophage CorrectionDocument11 pagesArticle Oesophage CorrectionKhalilSemlaliNo ratings yet
- 1752 1947 2 309 PDFDocument5 pages1752 1947 2 309 PDFHelen EngelinaNo ratings yet
- Small Cell Neuroendocrine Carcinoma of Bartholin's Gland: A Case ReportDocument4 pagesSmall Cell Neuroendocrine Carcinoma of Bartholin's Gland: A Case ReportAfrican Journal of Medicine and Pharma ResearchNo ratings yet
- Metastatic Behavior of Breast Cancer Subtypes: Ournal of Linical NcologyDocument7 pagesMetastatic Behavior of Breast Cancer Subtypes: Ournal of Linical NcologyJafet Gonzalez EstradaNo ratings yet
- LakhdarDocument5 pagesLakhdarPGY 6No ratings yet
- Metastasis of Differentiated Thyroid Carcinoma A Descriptive Study of 75 PatientsDocument10 pagesMetastasis of Differentiated Thyroid Carcinoma A Descriptive Study of 75 PatientsAthenaeum Scientific PublishersNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofCristhian del CidNo ratings yet
- Jurnal Patologi AnatomiDocument5 pagesJurnal Patologi Anatomiafiqzakieilhami11No ratings yet
- Mediastinal Mass in A 25-Year-Old Man: Chest Imaging and Pathology For CliniciansDocument5 pagesMediastinal Mass in A 25-Year-Old Man: Chest Imaging and Pathology For CliniciansWahyu RianiNo ratings yet
- CASE REPORT NewwwDocument11 pagesCASE REPORT NewwwkrisnaNo ratings yet
- Carcinossarcoma TireoideDocument6 pagesCarcinossarcoma TireoidevetcancerbrasilNo ratings yet
- Malignant Giant Pheochromocytoma: A Case Report and Review of The LiteratureDocument8 pagesMalignant Giant Pheochromocytoma: A Case Report and Review of The LiteratureannesasoumyanNo ratings yet
- Cervical Cancer With Brain MetastasesDocument7 pagesCervical Cancer With Brain MetastasesTataru RaduNo ratings yet
- Radiotherapy of Oligometastatic Prostate Cancer Experience of The Mohamed VI Center For Cancer Treatment in Casablanca, MoroccoDocument7 pagesRadiotherapy of Oligometastatic Prostate Cancer Experience of The Mohamed VI Center For Cancer Treatment in Casablanca, MoroccoInternational Journal of Innovative Science and Research Technology100% (1)
- A Rare Huge Myxofibrosarcoma of Chest WallDocument3 pagesA Rare Huge Myxofibrosarcoma of Chest WallIOSRjournalNo ratings yet
- MainDocument8 pagesMainIoana CucuNo ratings yet
- Mucinouscystadenoma of The Pancreas:diagnosis and Surgicaltreatmentwith or Withoutsplenectomy of 2 CasesDocument9 pagesMucinouscystadenoma of The Pancreas:diagnosis and Surgicaltreatmentwith or Withoutsplenectomy of 2 CasesIJAR JOURNALNo ratings yet
- Mucoepidermoid Carcinomaof The External Auditory Canal (Eac)Document4 pagesMucoepidermoid Carcinomaof The External Auditory Canal (Eac)IJAR JOURNALNo ratings yet
- Alveolar Rhabdomyosarcoma of The Vulva in An Adult: A Case Report and Literature ReviewDocument7 pagesAlveolar Rhabdomyosarcoma of The Vulva in An Adult: A Case Report and Literature Reviewdesthalia cyatraningtyasNo ratings yet
- TangDocument8 pagesTangPatricia BezneaNo ratings yet
- Non Small-Cell Lung Cancer in A 15-Year-Old NonsmokerDocument2 pagesNon Small-Cell Lung Cancer in A 15-Year-Old Nonsmokertonirian99No ratings yet
- HodgkinDisease FRenPro3739Document0 pagesHodgkinDisease FRenPro3739Jemmy SusatiaNo ratings yet
- A Young Child With Recurrent Pneumonia and HemoptyDocument4 pagesA Young Child With Recurrent Pneumonia and Hemoptylincolnbasilio1No ratings yet
- Annals of Medicine and SurgeryDocument5 pagesAnnals of Medicine and SurgeryUsee TvNo ratings yet
- Pathologic Quiz Case: Ovarian Mass in A 2-Year-Old Girl Presenting With Pleural EffusionsDocument4 pagesPathologic Quiz Case: Ovarian Mass in A 2-Year-Old Girl Presenting With Pleural EffusionsMateen ShukriNo ratings yet
- 2017 Diagnostic Relevance of Metastatic Renal Cell Carcinoma in The Head and Neck An Evaluation of 22 Cases in 671 PatientsDocument7 pages2017 Diagnostic Relevance of Metastatic Renal Cell Carcinoma in The Head and Neck An Evaluation of 22 Cases in 671 PatientsAlfonsoSánchezNo ratings yet
- 10.1186@1748 717X 1 17.pdfMUNTER PDFDocument6 pages10.1186@1748 717X 1 17.pdfMUNTER PDFpaolaNo ratings yet
- Testicular CancerDocument12 pagesTesticular Cancerghost_724No ratings yet
- E17 FullDocument5 pagesE17 FullSajit RawatNo ratings yet
- Malignant Phyllodes Tumor of The BreastDocument16 pagesMalignant Phyllodes Tumor of The BreastunknownNo ratings yet
- Classification of Biopsy-Confirmed Brain Tumors Using Single-Voxel MR SpectrosDocument7 pagesClassification of Biopsy-Confirmed Brain Tumors Using Single-Voxel MR SpectrosPandu DiputraNo ratings yet
- Multiple Synchronous Breast and Lung CarcinomaDocument14 pagesMultiple Synchronous Breast and Lung CarcinomaAnitei GabrielaNo ratings yet
- Case Study 2Document7 pagesCase Study 2ash kingNo ratings yet
- A Case Report of Chest Wall Desmoplastic Sma - 2024 - International Journal of SDocument4 pagesA Case Report of Chest Wall Desmoplastic Sma - 2024 - International Journal of SRonald QuezadaNo ratings yet
- Esophageal Composite Tumor With Neuroendocrine Component: A Rare EntityDocument4 pagesEsophageal Composite Tumor With Neuroendocrine Component: A Rare EntityIJAR JOURNALNo ratings yet
- Single Institution Study On The Management of Childhood Bladder and Prostate RhabdomyosarcomaDocument5 pagesSingle Institution Study On The Management of Childhood Bladder and Prostate RhabdomyosarcomaIJAR JOURNALNo ratings yet
- Pe09055 PDFDocument5 pagesPe09055 PDFMed MedNo ratings yet
- Cancer de Cervix y EndometrioDocument24 pagesCancer de Cervix y EndometriomaritaradNo ratings yet
- Reporte de Caso Cancer MamaDocument5 pagesReporte de Caso Cancer MamaCRISTHIAN CASTILLO JIBAJANo ratings yet
- Growth Patterns of Craniopharyngiomas: Clinical Analysis of 226 PatientsDocument16 pagesGrowth Patterns of Craniopharyngiomas: Clinical Analysis of 226 PatientsAmina GoharyNo ratings yet
- 650-Article Text-2348-1-10-20230510Document4 pages650-Article Text-2348-1-10-20230510Tresor KabambaNo ratings yet
- A Rare Case of Paediatric Lung Tumor: Pleuropulmonary Blastoma (Type-1 PPB)Document1 pageA Rare Case of Paediatric Lung Tumor: Pleuropulmonary Blastoma (Type-1 PPB)Javed AliNo ratings yet
- Current Diagnosis and Management of Retroperitoneal SarcomaDocument11 pagesCurrent Diagnosis and Management of Retroperitoneal SarcomaMaximiliano TorresNo ratings yet
- Rebel Lo 2021Document27 pagesRebel Lo 2021cydolusNo ratings yet
- 2021 Metastasis of Clear Cell Renal Cell Carcinoma To The Larynx A Short Literature Review and Presentation of A Rare Case of Prolonged SurvivalDocument3 pages2021 Metastasis of Clear Cell Renal Cell Carcinoma To The Larynx A Short Literature Review and Presentation of A Rare Case of Prolonged SurvivalAlfonsoSánchezNo ratings yet
- Prognostic Factors For Recurrence in Patients With Papillary Thyroid CarcinomaDocument8 pagesPrognostic Factors For Recurrence in Patients With Papillary Thyroid CarcinomaLeonardo LeónNo ratings yet
- Basal Cell Carcinoma: Advances in Treatment and ResearchFrom EverandBasal Cell Carcinoma: Advances in Treatment and ResearchMichael R. MigdenNo ratings yet
- Monogastric Digestive SystemDocument25 pagesMonogastric Digestive SystemMae Sntg OraNo ratings yet
- Daftar Pustaka ReferatDocument2 pagesDaftar Pustaka ReferatBetharlitha PurLikaNo ratings yet
- Dental Anxiety PDFDocument12 pagesDental Anxiety PDFKhalydia NafishaNo ratings yet
- Chapter 12 Survey LinesDocument7 pagesChapter 12 Survey Linessamir_patel_20No ratings yet
- Stabilisation and Safe Transport of The Critically Ill ChildDocument9 pagesStabilisation and Safe Transport of The Critically Ill ChildAdrian CraciunNo ratings yet
- Knowledge and Accessibility of Cervical Cancer Screening Services Among Women of Reproductive Age in Rural Communities of Ekiti StateDocument7 pagesKnowledge and Accessibility of Cervical Cancer Screening Services Among Women of Reproductive Age in Rural Communities of Ekiti StateInternational Journal of Innovative Science and Research TechnologyNo ratings yet
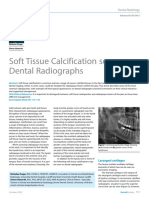
- Soft Tissue Calcification Seen On Dental RadiographsDocument4 pagesSoft Tissue Calcification Seen On Dental RadiographsMohammad Abdulmon’emNo ratings yet
- Luluk Handayani - PPTDocument14 pagesLuluk Handayani - PPTLuluk handayaniNo ratings yet
- FRACTURE PDF FixDocument47 pagesFRACTURE PDF FixselviNo ratings yet
- How To Stop Macular DegenerationDocument66 pagesHow To Stop Macular DegenerationJenny Bhatt100% (1)
- Interpersonal Model: Harry Stack Sullivan Development Occurs in Stages With Changing RelationshipsDocument38 pagesInterpersonal Model: Harry Stack Sullivan Development Occurs in Stages With Changing RelationshipsDhen MarcNo ratings yet
- Malaysian Endodontics Journal Volume 21Document53 pagesMalaysian Endodontics Journal Volume 21Devin Kwan100% (1)
- Cop-5-Policy On Uniform Use of CPRDocument23 pagesCop-5-Policy On Uniform Use of CPRanithaNo ratings yet
- Andabuen National High School: Benito Soliven South DistrictDocument3 pagesAndabuen National High School: Benito Soliven South DistrictRonalyn ColladoNo ratings yet
- Daftar Singkatan RSUP PDocument32 pagesDaftar Singkatan RSUP Pmaria ulfaNo ratings yet
- Journal-Appraisal - Pgmi Del Prado, RockyDocument14 pagesJournal-Appraisal - Pgmi Del Prado, Rockyrockson del PradoNo ratings yet
- School Health ServicesDocument2 pagesSchool Health ServicesCrystal Ann Monsale TadiamonNo ratings yet
- Cardiac PanelDocument6 pagesCardiac Panellinjinxian444No ratings yet
- Interpret HbA2 With Caution Per DR Barbara BainDocument50 pagesInterpret HbA2 With Caution Per DR Barbara Baindamadol100% (1)
- Cabo H. Color Atlas of Dermoscopy 2018Document354 pagesCabo H. Color Atlas of Dermoscopy 2018Esther ParvuNo ratings yet
- Empty Sella SyndromeDocument2 pagesEmpty Sella Syndromewawan_291289100% (1)
- Stress SurveyDocument2 pagesStress Surveydoctork2No ratings yet
- NCP BleedingDocument3 pagesNCP Bleedingapi-316491996No ratings yet
- Resonium - Info o LekuDocument3 pagesResonium - Info o LekuЂорђе ИнђићNo ratings yet
- Gender Report March - June 2020Document8 pagesGender Report March - June 2020Revy HamaNo ratings yet
- Cot DLL Health 8 Q3Document8 pagesCot DLL Health 8 Q3Jarnel Cabalsa100% (1)
- NKF Kidney Transplant Application Form B1Document8 pagesNKF Kidney Transplant Application Form B1Ainaa FarhanaNo ratings yet