Download as pdf or txt
You might also like
- Ebook American Corrections 13Th Edition Todd R Clear Online PDF All ChapterDocument69 pagesEbook American Corrections 13Th Edition Todd R Clear Online PDF All Chaptersonya.martinez866100% (11)
- EPA07 Maxxforce 11, 13 Diagnostic Manual-1Document190 pagesEPA07 Maxxforce 11, 13 Diagnostic Manual-1Manuel Alejandro Velez NavaNo ratings yet
- Exoskeleton SCIDocument11 pagesExoskeleton SCIsana siddiqueNo ratings yet
- Effects of A Supported Speed Treadmill Training Exercise Program On Impairment and Function For Children With Cerebral PalsyDocument9 pagesEffects of A Supported Speed Treadmill Training Exercise Program On Impairment and Function For Children With Cerebral PalsyKimum KimúmNo ratings yet
- Effectiveness of Treadmill Training On Gait Function in Children With Cerebral Palsy: Meta-AnalysisDocument10 pagesEffectiveness of Treadmill Training On Gait Function in Children With Cerebral Palsy: Meta-AnalysisNovie AstiniNo ratings yet
- Willoughby Et Al. (2010)Document7 pagesWilloughby Et Al. (2010)ع الNo ratings yet
- ProQuestDocuments 2017 11 11 PDFDocument13 pagesProQuestDocuments 2017 11 11 PDFDonny HendrawanNo ratings yet
- Sports: Backward Running: Acute E Performance in Preadolescent BoysDocument11 pagesSports: Backward Running: Acute E Performance in Preadolescent BoysYeison UrregoNo ratings yet
- Correlation of Balance Tests Scores With Modified Physical Performance Test in Indian Community-Dwelling Older AdultsDocument19 pagesCorrelation of Balance Tests Scores With Modified Physical Performance Test in Indian Community-Dwelling Older AdultsDr. Krishna N. SharmaNo ratings yet
- OTAGO On FrailtyDocument5 pagesOTAGO On FrailtyNura Eky VNo ratings yet
- Gates Et Al. (2012)Document35 pagesGates Et Al. (2012)ع الNo ratings yet
- Effects of Exergame Training On The Health Promotion of Young AdultsDocument10 pagesEffects of Exergame Training On The Health Promotion of Young AdultsCarlosNo ratings yet
- Ymj 55 1736Document7 pagesYmj 55 1736Cristian HanganNo ratings yet
- Ortega 2014Document23 pagesOrtega 2014Visnja DjordjicNo ratings yet
- 1 s2.0 S1013702515000615 MainDocument9 pages1 s2.0 S1013702515000615 MainLalala Safitri2000No ratings yet
- Effects of Integrative Core Stability Training OnDocument15 pagesEffects of Integrative Core Stability Training OnMari PaoNo ratings yet
- Brazilian Journal of Physical TherapyDocument11 pagesBrazilian Journal of Physical TherapyshodhgangaNo ratings yet
- DownloadDocument9 pagesDownloadcesar8319No ratings yet
- Yonsei Med J2014 ParkDocument8 pagesYonsei Med J2014 ParkCristian HanganNo ratings yet
- Kassim 2022Document12 pagesKassim 2022ع الNo ratings yet
- Ijerph 18 10709Document13 pagesIjerph 18 10709Pablo Orellana StevensNo ratings yet
- JUrnal Tumbang, 023Document9 pagesJUrnal Tumbang, 023Rafli Jody PratamaNo ratings yet
- Aras Et Al. (2019)Document10 pagesAras Et Al. (2019)ع الNo ratings yet
- International Journal of Current Advanced Research International Journal of Current Advanced ResearchDocument5 pagesInternational Journal of Current Advanced Research International Journal of Current Advanced ResearchI Made Dhita PriantharaNo ratings yet
- Develop Med Child Neuro - 2014 - Curtis - The Central Role of Trunk Control in The Gross Motor Function of Children WithDocument7 pagesDevelop Med Child Neuro - 2014 - Curtis - The Central Role of Trunk Control in The Gross Motor Function of Children WithAmr Mohamed GalalNo ratings yet
- Investigeting The Effects of Standing Training On Body Functions and Activity For Nonambulatory Children With MyelomeningoceleDocument6 pagesInvestigeting The Effects of Standing Training On Body Functions and Activity For Nonambulatory Children With MyelomeningoceleMutiarahmiNo ratings yet
- 2019 Article AbstractsFromThe5thInternation PDFDocument41 pages2019 Article AbstractsFromThe5thInternation PDFStephano NgangiNo ratings yet
- 5-4-26 1 IjyppeDocument7 pages5-4-26 1 IjyppeMansi ParmarNo ratings yet
- 3 GIAGAZOGLOU - pp39 49Document11 pages3 GIAGAZOGLOU - pp39 49Mara CarbajoNo ratings yet
- Sensors 22 02668 v2Document14 pagesSensors 22 02668 v2RUBEN DARIO AQUIZE PALACIOSNo ratings yet
- Ijerph 19 08212 v3Document16 pagesIjerph 19 08212 v3SAMARIA RAQUEL ESQUIVEL RINCONNo ratings yet
- Fragala Pinkham2013Document10 pagesFragala Pinkham2013Beatriz Garcia-PoggioNo ratings yet
- Yang Et Al. 2022 Otago Exercise Programme - Systematic ReviewDocument14 pagesYang Et Al. 2022 Otago Exercise Programme - Systematic ReviewClarissa LimNo ratings yet
- פרקינסוןDocument15 pagesפרקינסוןHadas LippnerNo ratings yet
- 5 - Yadav Sunita. Correlation of Balance Tests Scores With Modified Physical Performance Test in Indian Community-Dwelling Older AdultsDocument19 pages5 - Yadav Sunita. Correlation of Balance Tests Scores With Modified Physical Performance Test in Indian Community-Dwelling Older AdultsDr. Krishna N. SharmaNo ratings yet
- Plyometric Training Effectiveness and Optimal.3Document11 pagesPlyometric Training Effectiveness and Optimal.3LeonardoValenzuelaNo ratings yet
- Agmr 22 0073Document7 pagesAgmr 22 0073rizki kaiNo ratings yet
- 2019 - Flexibility and Jump Performance - JPESDocument6 pages2019 - Flexibility and Jump Performance - JPESMaiaraNo ratings yet
- Effects of Resistance Training On The.3Document5 pagesEffects of Resistance Training On The.3cc polyuNo ratings yet
- 1 s2.0 S0197457223002094 MainDocument11 pages1 s2.0 S0197457223002094 Maintamara arenasNo ratings yet
- Tong 2006Document7 pagesTong 2006Amanda BarrosNo ratings yet
- Effects of Interactive Video-Game-Based Exercise On Balance in Older AdultsDocument10 pagesEffects of Interactive Video-Game-Based Exercise On Balance in Older AdultsYamato HotsuinNo ratings yet
- Ozaki 2013Document8 pagesOzaki 2013PierinaNo ratings yet
- Jump Rope Training For Health and Fitness in SchooDocument15 pagesJump Rope Training For Health and Fitness in Schoodani yusupNo ratings yet
- Cherng Et Al. (2007)Document8 pagesCherng Et Al. (2007)ع الNo ratings yet
- Otago 1 PDFDocument3 pagesOtago 1 PDFAde Maghvira PutriNo ratings yet
- Exercise and Progressive Supranuclear Palsy: The Need For Explicit Exercise ReportingDocument9 pagesExercise and Progressive Supranuclear Palsy: The Need For Explicit Exercise ReportingNathaly CantorNo ratings yet
- 10.1093 PTJ Pzac153Document13 pages10.1093 PTJ Pzac153evelyn.minichNo ratings yet
- 01 - Is Device-Measured Vigorous Physical Activity Associated With Health-Related Outcomes in Children and Adolescents A Systematic Review and Meta-AnalysisDocument12 pages01 - Is Device-Measured Vigorous Physical Activity Associated With Health-Related Outcomes in Children and Adolescents A Systematic Review and Meta-AnalysisJosé Antonio MárquezNo ratings yet
- Develop Med Child Neuro - 2021 - Chaovalit - Sit To Stand Training For Self Care and Mobility in Children With CerebralDocument7 pagesDevelop Med Child Neuro - 2021 - Chaovalit - Sit To Stand Training For Self Care and Mobility in Children With Cerebralzizee61No ratings yet
- Projeto ASSO 2020Document35 pagesProjeto ASSO 2020Vanessa ViveirosNo ratings yet
- RetrieveDocument14 pagesRetrieveshamel robinsonNo ratings yet
- Robot-Assisted Gait Training (Lokomat) Improves Walking Function and Activity in People With Spinal Cord Injury: A Systematic ReviewDocument13 pagesRobot-Assisted Gait Training (Lokomat) Improves Walking Function and Activity in People With Spinal Cord Injury: A Systematic ReviewSAMUEL ENRIQUE ASTUDILLO VARGASNo ratings yet
- 1 s2.0 S1836955317301467 MainDocument12 pages1 s2.0 S1836955317301467 MainNeyfer Henao RiveroNo ratings yet
- Geriatrics 07 00088Document10 pagesGeriatrics 07 0008834. Putu Mariska Abdi CahyaniNo ratings yet
- Características Asociadas Con La Actividad Física Entre Niños y Adolescentes Con Parálisis Cerebral Unilateral Que Caminan de Forma IndependienteDocument8 pagesCaracterísticas Asociadas Con La Actividad Física Entre Niños y Adolescentes Con Parálisis Cerebral Unilateral Que Caminan de Forma IndependienteKimum KimúmNo ratings yet
- Effect of Circuit Training On Selected Health-Related Physical Fitness Components: The Case of Sport Science StudentsDocument7 pagesEffect of Circuit Training On Selected Health-Related Physical Fitness Components: The Case of Sport Science StudentsCoolveticaNo ratings yet
- Artritis Idiopatica JuvenilDocument12 pagesArtritis Idiopatica JuvenilJhos_Leon15No ratings yet
- Senthilarticlein JCDRDocument4 pagesSenthilarticlein JCDRAnnisa KusumaNo ratings yet
- Jhse Vol 12 N 1 219-235Document17 pagesJhse Vol 12 N 1 219-235Maybelle E. EraNo ratings yet
- Experimental Gerontology: Contents Lists Available atDocument9 pagesExperimental Gerontology: Contents Lists Available atGorkaBuesaNo ratings yet
- Strengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesFrom EverandStrengthening Versus Stabilisation Exercise Programmes for Preventing and Reducing Low Back Pain in FemalesNo ratings yet
- 3 Mode Exc OADocument7 pages3 Mode Exc OANura Eky VNo ratings yet
- Bloom's Taxonomy - WikipediaDocument11 pagesBloom's Taxonomy - WikipediaNura Eky VNo ratings yet
- Overview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionDocument4 pagesOverview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionNura Eky VNo ratings yet
- S0003999321002963Document10 pagesS0003999321002963Nura Eky VNo ratings yet
- 1 s2.0 S0531556520305611 MainDocument8 pages1 s2.0 S0531556520305611 MainNura Eky VNo ratings yet
- 1 s2.0 S0003999321001404Document10 pages1 s2.0 S0003999321001404Nura Eky VNo ratings yet
- OTAGO On FrailtyDocument5 pagesOTAGO On FrailtyNura Eky VNo ratings yet
- 1 s2.0 S0966636212000811 MainDocument5 pages1 s2.0 S0966636212000811 MainNura Eky VNo ratings yet
- Effect of Different Types of Exercises On Psychological and Cognitive Features in People With Parkinson's Disease: A Randomized Controlled TrialDocument10 pagesEffect of Different Types of Exercises On Psychological and Cognitive Features in People With Parkinson's Disease: A Randomized Controlled TrialNura Eky VNo ratings yet
- 16646-Article Text-14610-1-10-20070123Document2 pages16646-Article Text-14610-1-10-20070123Nura Eky VNo ratings yet
- 1 s2.0 S1877065719301794 MainDocument8 pages1 s2.0 S1877065719301794 MainNura Eky VNo ratings yet
- CP Spastic, Diskinetik, AtaxicDocument4 pagesCP Spastic, Diskinetik, AtaxicNura Eky VNo ratings yet
- Design CPMDocument5 pagesDesign CPMNura Eky VNo ratings yet
- Anterior Cruciate Ligament Injury-Who Succeeds WitDocument9 pagesAnterior Cruciate Ligament Injury-Who Succeeds WitNura Eky VNo ratings yet
- Polifarmasi and Fall in ElderlyDocument5 pagesPolifarmasi and Fall in ElderlyNura Eky VNo ratings yet
- Hof Condition For Dynamic StabilityDocument8 pagesHof Condition For Dynamic StabilityNura Eky VNo ratings yet
- CASP RCT Checklist PDF Fillable FormDocument4 pagesCASP RCT Checklist PDF Fillable FormNura Eky VNo ratings yet
- Pai Patton97PostPrintDocument7 pagesPai Patton97PostPrintNura Eky VNo ratings yet
- Impact of Covid Patient RecoveryDocument15 pagesImpact of Covid Patient RecoveryNura Eky VNo ratings yet
- Spleen: - Site of Lymphocyte Proliferation - Immune Surveillance and Response - Cleanses The BloodDocument13 pagesSpleen: - Site of Lymphocyte Proliferation - Immune Surveillance and Response - Cleanses The BloodNura Eky VNo ratings yet
- Obesity Review MelaninDocument12 pagesObesity Review MelaninNura Eky VNo ratings yet
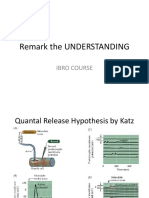
- Remark The UNDERSTANDING: Ibro CourseDocument4 pagesRemark The UNDERSTANDING: Ibro CourseNura Eky VNo ratings yet
- Leonard, 2002Document18 pagesLeonard, 2002Nura Eky VNo ratings yet
- Acharya LifeDocument19 pagesAcharya LifeAnand SwamiNo ratings yet
- Genesys Inbound VoiceDocument6 pagesGenesys Inbound VoiceparidimalNo ratings yet
- Communication Processes, Principles, and Ethics (Reviewer)Document4 pagesCommunication Processes, Principles, and Ethics (Reviewer)Jessie TindoyNo ratings yet
- MGMT1000 Fundamentals of Management Semester 2 2019 Curtin Mauritius INT PDFDocument13 pagesMGMT1000 Fundamentals of Management Semester 2 2019 Curtin Mauritius INT PDFkimNo ratings yet
- Chapter 1: Managers, Profits, and Markets: Multiple ChoiceDocument10 pagesChapter 1: Managers, Profits, and Markets: Multiple ChoiceMarwa Al RiyamiNo ratings yet
- Chapter 1 Toxins - Kill The Primates, Rule The World. Or: Don't Turn Your Back On A Fungus!Document9 pagesChapter 1 Toxins - Kill The Primates, Rule The World. Or: Don't Turn Your Back On A Fungus!Eved1981 superrito.comNo ratings yet
- Document 3Document2 pagesDocument 3ANKIT KUMAR DUBEYNo ratings yet
- Current Technology in Genetic EngineeringDocument2 pagesCurrent Technology in Genetic EngineeringAnne Clarisse BarrientosNo ratings yet
- Macys Inc Store ListingDocument57 pagesMacys Inc Store ListingSurya NarayananNo ratings yet
- AR-Raheeq Al-Makhtum (The Seald Nectar)Document297 pagesAR-Raheeq Al-Makhtum (The Seald Nectar)rabtay100% (1)
- Al., G.R. No. 209271, December 8, 2015Document116 pagesAl., G.R. No. 209271, December 8, 2015Martin SNo ratings yet
- 08 - Chapter 2 PDFDocument48 pages08 - Chapter 2 PDFpradeep bandaru0% (1)
- Why Literature by Mario Vargas LlosaDocument7 pagesWhy Literature by Mario Vargas Llosaadriel mendoza33% (3)
- Terri Stegmiller Art and Design - Art For SaleDocument1 pageTerri Stegmiller Art and Design - Art For Salemeethi_andreaNo ratings yet
- NorMar 250-350 TI Manual CompletoDocument20 pagesNorMar 250-350 TI Manual CompletomarlinyareNo ratings yet
- Lost and Found SpellDocument9 pagesLost and Found SpellKarthikNo ratings yet
- Co vs. CADocument3 pagesCo vs. CAJaysonNo ratings yet
- Heroes Are Made Not BornDocument2 pagesHeroes Are Made Not BornYoong iiNo ratings yet
- Saint James Academy: The Problem and Its BackgroundDocument78 pagesSaint James Academy: The Problem and Its BackgroundYna Marie GutierrezNo ratings yet
- The Best Casinos Perform Slots in VegasvzyijDocument2 pagesThe Best Casinos Perform Slots in Vegasvzyijpumaorchid83No ratings yet
- Year 3 Civic Lesson Plan (February-Mutual Respect) : By:MissashDocument1 pageYear 3 Civic Lesson Plan (February-Mutual Respect) : By:MissashJensen ChangNo ratings yet
- Cargo Handling 5Document21 pagesCargo Handling 5LilCent MmanuelNo ratings yet
- China Banking Corp vs. CA - GR No.140687Document13 pagesChina Banking Corp vs. CA - GR No.140687Leizl A. VillapandoNo ratings yet
- Value Chain AnalysisDocument76 pagesValue Chain AnalysisA B M Rafiqul Hasan Khan67% (3)
- Lesson Plan-Elm 375Document3 pagesLesson Plan-Elm 375api-582006278No ratings yet
- Inset OutputDocument2 pagesInset OutputJackielou Biala-Guba Mosada RebualosNo ratings yet
- Fetal Skull: Badeea Seliem Soliman Assistant Prof. of Gynecology and Obstetrics Zagazig UniversityDocument107 pagesFetal Skull: Badeea Seliem Soliman Assistant Prof. of Gynecology and Obstetrics Zagazig UniversityBharat Thapa50% (2)
- Indifference, Again Author(s) : Michael Meredith Source: Log, Winter 2017, No. 39 (Winter 2017), Pp. 75-79 Published By: Anyone CorporationDocument6 pagesIndifference, Again Author(s) : Michael Meredith Source: Log, Winter 2017, No. 39 (Winter 2017), Pp. 75-79 Published By: Anyone CorporationSepideh KordmirNo ratings yet