Download as pdf or txt
You might also like
- Unit IG2: Risk Assessment: Declaration: by Submitting This Assessment (Parts 1Document18 pagesUnit IG2: Risk Assessment: Declaration: by Submitting This Assessment (Parts 1Mohammad Awees Sanadi83% (6)
- Kioti NS4710, NS6010, NS4710H, NS5310H, NS6010H Tractor Operator's ManualDocument15 pagesKioti NS4710, NS6010, NS4710H, NS5310H, NS6010H Tractor Operator's ManualLisakolyNo ratings yet
- Kioti NX4510, NX5010, NX5510, NX6010 Tractor Operator's ManualDocument15 pagesKioti NX4510, NX5010, NX5510, NX6010 Tractor Operator's ManualLisakolyNo ratings yet
- Shivshrishti Co-Operative Housing Society LTDDocument6 pagesShivshrishti Co-Operative Housing Society LTDMohammad Awees Sanadi67% (3)
- GasCal 1100 Dilution CalibratorDocument83 pagesGasCal 1100 Dilution Calibratorhacguest8485No ratings yet
- Secrets of Hypnosis Revealed!Document39 pagesSecrets of Hypnosis Revealed!Angel Fulton100% (1)
- 8 Extraordinary Vessels Maciocia OnlineDocument129 pages8 Extraordinary Vessels Maciocia OnlineRudolph Antony Thomas100% (3)
- Prodelin 1385Document33 pagesProdelin 1385bebebrenda100% (1)
- Form ODocument2 pagesForm ORavi Krishnan75% (4)
- Act Medical Certificate FormatDocument2 pagesAct Medical Certificate Formats anithaNo ratings yet
- Form O New FormatDocument3 pagesForm O New FormatGaurav Jangid100% (2)
- Geoelectric Strike and Its Application in MagnetotelluricsDocument40 pagesGeoelectric Strike and Its Application in MagnetotelluricsamiruddinNo ratings yet
- Manual CFS-830 PDFDocument184 pagesManual CFS-830 PDFLuisRocha50% (2)
- Installation GuideDocument128 pagesInstallation GuidetimeNo ratings yet
- Series 2000 Instruments Wireline Anchor Applications: Part Number 90-03 Revision CDocument166 pagesSeries 2000 Instruments Wireline Anchor Applications: Part Number 90-03 Revision CLuis Eduardo Albarracin RugelesNo ratings yet
- HP DM and Relief Manual, 2012Document115 pagesHP DM and Relief Manual, 2012VIJAY KUMAR HEER100% (1)
- KrisEnergy LTD - Appendix D - Volume2Document194 pagesKrisEnergy LTD - Appendix D - Volume2Invest StockNo ratings yet
- Indonesia Baroid VPE Structure - 1811 PDFDocument13 pagesIndonesia Baroid VPE Structure - 1811 PDFfebry_rfNo ratings yet
- CPF GPF FormsDocument10 pagesCPF GPF FormsTaresh MittalNo ratings yet
- MWD PresentationDocument13 pagesMWD PresentationBabi LakhdariNo ratings yet
- SS6800 - Line Management System Manual Second RevDocument62 pagesSS6800 - Line Management System Manual Second RevGonza Pf0% (1)
- Part Number 60-20 Revision C: Installation, Operation, and Maintenance With Illustrated Parts BreakdownDocument134 pagesPart Number 60-20 Revision C: Installation, Operation, and Maintenance With Illustrated Parts BreakdownLuis Eduardo Albarracin RugelesNo ratings yet
- MSC.97 (73) HSC Code 2000Document239 pagesMSC.97 (73) HSC Code 2000Rajnish KumarNo ratings yet
- Accident Register - CRM - Wound Certificate: OriginalDocument2 pagesAccident Register - CRM - Wound Certificate: OriginalUrmi royNo ratings yet
- Peso Tipo 40Document118 pagesPeso Tipo 40Miguel angel leon bautistaNo ratings yet
- Advt 06Document3 pagesAdvt 06Hari Krishna ChaurasiaNo ratings yet
- Specific Gravity@ 60 ° FDocument9 pagesSpecific Gravity@ 60 ° FindahNo ratings yet
- NaviTrak Short Radius Manual 750-500-029Document110 pagesNaviTrak Short Radius Manual 750-500-029MaximNo ratings yet
- Drilling EssayDocument4 pagesDrilling EssayngdthgyyttrNo ratings yet
- MSS Software User's Guide 77719UG100Document488 pagesMSS Software User's Guide 77719UG100MaximNo ratings yet
- TotcoDocument13 pagesTotcoObdulioNo ratings yet
- Part Number 28-31 Revision C: Installation & OperationDocument148 pagesPart Number 28-31 Revision C: Installation & OperationLuis AlbarracinNo ratings yet
- 20 21 PDFDocument56 pages20 21 PDFMauricio GarciaNo ratings yet
- FSLDocument38 pagesFSLsiolagNo ratings yet
- Logiq-A, B: Kittisak S. Grit DDocument15 pagesLogiq-A, B: Kittisak S. Grit DSuryak1997No ratings yet
- Installation Manual InventorDocument156 pagesInstallation Manual InventorGeopas GreeceNo ratings yet
- Preparation of Glass Beads and Powder Pills For XRF Analysis of Silicic and Calcareous RocksDocument18 pagesPreparation of Glass Beads and Powder Pills For XRF Analysis of Silicic and Calcareous RocksJOSE ABADNo ratings yet
- JPT 2024-01Document102 pagesJPT 2024-01FarresForrzaNo ratings yet
- TM 11 6130 413 12Document34 pagesTM 11 6130 413 12David Bentley100% (1)
- Part Number 27-58: Installation, Operation, and Maintenance With Illustrated Parts BreakdownDocument26 pagesPart Number 27-58: Installation, Operation, and Maintenance With Illustrated Parts BreakdownLuis Eduardo Albarracin RugelesNo ratings yet
- Part Number 28-31 Revision C: Installation & OperationDocument148 pagesPart Number 28-31 Revision C: Installation & OperationLuis Eduardo Albarracin RugelesNo ratings yet
- Part Number 30-03: Installation, Operation and MaintenanceDocument30 pagesPart Number 30-03: Installation, Operation and MaintenanceLuis AlbarracinNo ratings yet
- NKY-C15Ex Torque Manual EnglishDocument28 pagesNKY-C15Ex Torque Manual Englishกัญญารัตน์ พูลทองNo ratings yet
- Technical Manual: Rig Air Filter P/N 270240 Air Filter/Regulator P/N 270244Document24 pagesTechnical Manual: Rig Air Filter P/N 270240 Air Filter/Regulator P/N 270244Andres NavarroNo ratings yet
- Birech Amine MWD-LWD Field Engineer IIDocument2 pagesBirech Amine MWD-LWD Field Engineer IINewLife WillcomeNo ratings yet
- 118914-HDS-NT Mecha Ope Us-E04-201108Document198 pages118914-HDS-NT Mecha Ope Us-E04-201108jturnerNo ratings yet
- Triple ComboDocument2 pagesTriple ComboilkerkozturkNo ratings yet
- STM6 LM PDFDocument20 pagesSTM6 LM PDFRepresentaciones y Distribuciones FALNo ratings yet
- Mou 2004Document3 pagesMou 2004Ankur DuttaNo ratings yet
- Part Number 60-43 Revision A: Installation, Operation, Maintenance AND Illustrated Parts BreakdownDocument55 pagesPart Number 60-43 Revision A: Installation, Operation, Maintenance AND Illustrated Parts BreakdownLuis Eduardo Albarracin RugelesNo ratings yet
- Characterisation of The Egyptian Pliocene Bentonite From The Sohag Region For Pharmaceutical UseDocument12 pagesCharacterisation of The Egyptian Pliocene Bentonite From The Sohag Region For Pharmaceutical UseNguyễn Thị Hải YếnNo ratings yet
- IWCF Surface Vertical Kill Sheet - API Field Units - Revised July 2010Document4 pagesIWCF Surface Vertical Kill Sheet - API Field Units - Revised July 2010rverretNo ratings yet
- Part Number 60-40 Revision B: Start-Up, Operation, and MaintenanceDocument257 pagesPart Number 60-40 Revision B: Start-Up, Operation, and MaintenanceLuis Eduardo Albarracin RugelesNo ratings yet
- NIE Chennai 27-12-2020 PDFDocument14 pagesNIE Chennai 27-12-2020 PDFkarunaharan 1964No ratings yet
- Part Number 80-01 Revision A: Installation, Operation, Maintenance and Illustrated Parts BreakdownDocument64 pagesPart Number 80-01 Revision A: Installation, Operation, Maintenance and Illustrated Parts BreakdownLuis Eduardo Albarracin RugelesNo ratings yet
- Single Output Current Sensor Assembly: Service ManualDocument40 pagesSingle Output Current Sensor Assembly: Service ManualAbdallah ElhendyNo ratings yet
- Hydro-Mast Weight Indicator System: Service ManualDocument64 pagesHydro-Mast Weight Indicator System: Service ManualAbdallah Elhendy100% (1)
- Membrane Filter Tester Instruction Manual: Part No. 396460 Rev. BDocument23 pagesMembrane Filter Tester Instruction Manual: Part No. 396460 Rev. BWajid NizamiNo ratings yet
- Experimentos Johnson Cook PDFDocument125 pagesExperimentos Johnson Cook PDFwircexdjNo ratings yet
- FYP 1 ReportDocument75 pagesFYP 1 ReportWWZNo ratings yet
- Drilling and Well Completion Edited 2022Document60 pagesDrilling and Well Completion Edited 2022ossama farghlyNo ratings yet
- AR860 English ManualDocument10 pagesAR860 English ManualMARIO SALVATORE SANDOVAL PAIPAYNo ratings yet
- Form oDocument2 pagesForm oPrateek BaruahNo ratings yet
- SaftyDocument3 pagesSaftyAnonymous ABLtDDvKuiNo ratings yet
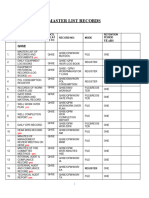
- Final Master List of Records - 2023Document5 pagesFinal Master List of Records - 2023Mohammad Awees SanadiNo ratings yet
- 00628068, Faizan Abdul Aziz, 1446-Gulf Academy of SafetyDocument21 pages00628068, Faizan Abdul Aziz, 1446-Gulf Academy of SafetyMohammad Awees SanadiNo ratings yet
- 10th History Revision TestDocument8 pages10th History Revision TestMohammad Awees SanadiNo ratings yet
- Computer Practical Filee-Term 1Document8 pagesComputer Practical Filee-Term 1Mohammad Awees SanadiNo ratings yet
- Nebosh International Technical Certificate in Oil and Gas Operational SafetyDocument2 pagesNebosh International Technical Certificate in Oil and Gas Operational SafetyMohammad Awees Sanadi100% (1)
- Shaikh, Arsalan, Ayub, 00626820,1446 GulfacademyDocument24 pagesShaikh, Arsalan, Ayub, 00626820,1446 GulfacademyMohammad Awees Sanadi100% (1)
- Unani System of MedicineDocument18 pagesUnani System of MedicineManika RaiNo ratings yet
- BTK Quick Hits Final PDFDocument24 pagesBTK Quick Hits Final PDFcusom34No ratings yet
- Final ProposalDocument46 pagesFinal ProposalPantaleon EdilNo ratings yet
- General Education ReviewerDocument15 pagesGeneral Education ReviewerMat Seigfried SaguiboNo ratings yet
- Smoking Is DangerousDocument3 pagesSmoking Is DangerousAbdulmalkNo ratings yet
- Feeding and Swallowing Disorders in Pediatric Neuromuscular DiseasesDocument13 pagesFeeding and Swallowing Disorders in Pediatric Neuromuscular DiseasesNádia MarquesNo ratings yet
- Clasificacion Rapin y AllenDocument3 pagesClasificacion Rapin y AllenEranko Victor Mol RubilarNo ratings yet
- Group 3 Diabetes MellitusDocument9 pagesGroup 3 Diabetes MellitusMary0% (1)
- Cardiorespiratory Assessment: Medical Chart ReadingDocument7 pagesCardiorespiratory Assessment: Medical Chart ReadingPrasath SelvarajNo ratings yet
- NCCN Guideline RC v3 2022Document20 pagesNCCN Guideline RC v3 2022dony hendrawanNo ratings yet
- Child Developmental ChecklistDocument10 pagesChild Developmental ChecklistfirstmomsclubNo ratings yet
- Survival of Pediatric Patients After CPRDocument11 pagesSurvival of Pediatric Patients After CPRMaria Regina CamargoNo ratings yet
- An Intensive Swallowing Exercise Protocol For Improving Swallowing Physiology in Older Adults With Radiographically Confirmed DysphagiaDocument7 pagesAn Intensive Swallowing Exercise Protocol For Improving Swallowing Physiology in Older Adults With Radiographically Confirmed DysphagiaMaria DemetriouNo ratings yet
- Exercise 1. Complete The Text Using The Words From The BoxDocument5 pagesExercise 1. Complete The Text Using The Words From The BoxВлада ВоеводинаNo ratings yet
- Feyer 2020 WvngoshawkDocument13 pagesFeyer 2020 WvngoshawkAgnieszka CzujkowskaNo ratings yet
- Daftar Pasien Neurologi RABU 22 APRIL 2020: Lontara 3 Saraf Kamar 1Document4 pagesDaftar Pasien Neurologi RABU 22 APRIL 2020: Lontara 3 Saraf Kamar 1Ilham Habib DjarkoniNo ratings yet
- Organoid ArticleDocument4 pagesOrganoid ArticleAnonimo AnonimoNo ratings yet
- Essay About Your CommunityDocument6 pagesEssay About Your Communitynhbtoxwhd100% (2)
- Nursing Clinical QuestionsDocument8 pagesNursing Clinical QuestionsMrinalini BakshiNo ratings yet
- 840 B2 Fire Rated Pu FoamDocument10 pages840 B2 Fire Rated Pu FoamJonathan Alexis Abarzua TorresNo ratings yet
- Arteriovenous MalformationsDocument22 pagesArteriovenous MalformationsJunus EufrataNo ratings yet
- Annotated BibliographyDocument8 pagesAnnotated BibliographyEunice AppiahNo ratings yet
- Hypertensive DietDocument6 pagesHypertensive DietCarlos NiñoNo ratings yet
- Case Pres - Imperforate AnusDocument26 pagesCase Pres - Imperforate AnusMerlash MerlaNo ratings yet
- Antiplasmodial and Toxicological Properties of Cnidoscolus AconitifoliusDocument14 pagesAntiplasmodial and Toxicological Properties of Cnidoscolus AconitifoliusRuthNo ratings yet
- Normal Variants Are Commonly Overread As Interictal EpileptiformDocument14 pagesNormal Variants Are Commonly Overread As Interictal EpileptiformRizka_aprilNo ratings yet
- MM 1 - Grammar Test Unit 10Document12 pagesMM 1 - Grammar Test Unit 10Jose Antonio Mattaz AsturizagaNo ratings yet
- Flyer PIT IDI Bandung LINKDocument1 pageFlyer PIT IDI Bandung LINKBabo SanNo ratings yet