
Hospitalization Due To Adverse Drug Reactions and Drug Interactions Before and After Haart
Hospitalization Due To Adverse Drug Reactions and Drug Interactions Before and After Haart
You might also like
- Production of Tablets and CapsulesDocument32 pagesProduction of Tablets and Capsulesraviteja79173% (15)
- The Importance of AdherenceDocument28 pagesThe Importance of AdherenceVijay LaptopNo ratings yet
- Tetanus: A Case ReportDocument2 pagesTetanus: A Case ReportrkotichaNo ratings yet
- Antibiotic and Oral Contraceptive Drug Interactions: Is There A Need For Concern?Document6 pagesAntibiotic and Oral Contraceptive Drug Interactions: Is There A Need For Concern?Eva SefianaNo ratings yet
- The Impact of COVID-19 On The Quality of Admission Clerkings On An Old Age Psychiatry Ward - An AuditDocument3 pagesThe Impact of COVID-19 On The Quality of Admission Clerkings On An Old Age Psychiatry Ward - An Auditkuda69790No ratings yet
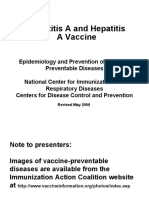
- Hepatitis A and Hepatitis A VaccineDocument31 pagesHepatitis A and Hepatitis A VaccinedydinNo ratings yet
- Kenya Health Sector Strategic Investment Plan 2013 To 2017Document100 pagesKenya Health Sector Strategic Investment Plan 2013 To 2017GEOFFREY KAMBUNINo ratings yet
- 11 AdherenceDocument33 pages11 AdherenceCalvin ChisangoNo ratings yet
- A Critical Review Evaluation of The Efficacy of Covid19 Vaccines in EnglandDocument14 pagesA Critical Review Evaluation of The Efficacy of Covid19 Vaccines in EnglandvalgurNo ratings yet
- CCO Cytokine TX in MM ExpressPointsDocument18 pagesCCO Cytokine TX in MM ExpressPointsveaceslav coscodanNo ratings yet
- Prevention Strategy of Infectious Diseases For Health Care WorkersDocument31 pagesPrevention Strategy of Infectious Diseases For Health Care WorkersarinNo ratings yet
- VIH Diagnóstico Reciente in The Clinic PDFDocument16 pagesVIH Diagnóstico Reciente in The Clinic PDFFernando ArancibiaNo ratings yet
- Phase II Study of Vicriviroc Versus Efavirenz (Both With Zidovudine/Lamivudine) in Treatment-Naive Subjects With HIV-1 InfectionDocument10 pagesPhase II Study of Vicriviroc Versus Efavirenz (Both With Zidovudine/Lamivudine) in Treatment-Naive Subjects With HIV-1 Infectionverra sitanggangNo ratings yet
- Antibody PDFDocument2 pagesAntibody PDFStef DygaNo ratings yet
- Management of MRSA NP: Slide ReferenceDocument29 pagesManagement of MRSA NP: Slide ReferenceDermawan SolehNo ratings yet
- A Prospective Study On The Practice of Conversion of Antibiotics From IV To Oral Route and The Barriers Affecting ItDocument3 pagesA Prospective Study On The Practice of Conversion of Antibiotics From IV To Oral Route and The Barriers Affecting ItInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Immunodeficiency: Abdul Ghaffar, Ph.D. E-Mail: Ghaffar@med - Sc.eduDocument10 pagesImmunodeficiency: Abdul Ghaffar, Ph.D. E-Mail: Ghaffar@med - Sc.eduAhmed Goma'aNo ratings yet
- Bone Marrow Transplant Recent Advances and Nursing ImplicationsDocument18 pagesBone Marrow Transplant Recent Advances and Nursing ImplicationsRob BordenNo ratings yet
- Ruxolitinib Cream For Treatment of Vitiligo: A Randomised, Controlled, Phase 2 TrialDocument11 pagesRuxolitinib Cream For Treatment of Vitiligo: A Randomised, Controlled, Phase 2 TrialDORIS Z.No ratings yet
- HHS Public Access: HIV-1 Drug Resistance and Resistance TestingDocument42 pagesHHS Public Access: HIV-1 Drug Resistance and Resistance TestingAlfiraNo ratings yet
- Clinical Policy: Donor Lymphocyte Infusion: Coding Implications Revision Log Important ReminderDocument7 pagesClinical Policy: Donor Lymphocyte Infusion: Coding Implications Revision Log Important ReminderAlfajriekaputraNo ratings yet
- DFDFDFDFDocument10 pagesDFDFDFDFkclaportNo ratings yet
- Nac Leve Puntos Finales Diseño de Estudios Cid 2008Document5 pagesNac Leve Puntos Finales Diseño de Estudios Cid 2008Gustavo GomezNo ratings yet
- Day 1 5 MMC BootcampDocument40 pagesDay 1 5 MMC BootcampDianne Erika MeguinesNo ratings yet
- Shifts in Healthcare Demand, Delivery and Care During The COVID-19 EraDocument33 pagesShifts in Healthcare Demand, Delivery and Care During The COVID-19 EraMassimo RiserboNo ratings yet
- Mallik Questions ReplyDocument9 pagesMallik Questions ReplysanthoshNo ratings yet
- BIDMC HIV Manual 2019Document97 pagesBIDMC HIV Manual 2019oluNo ratings yet
- RevChilInfectol2015 VIHUPCDocument11 pagesRevChilInfectol2015 VIHUPCPaola GalarzaNo ratings yet
- Pharmacotherapeutic Group: Antivirals For Treatment of HIV Infections, CombinationsDocument30 pagesPharmacotherapeutic Group: Antivirals For Treatment of HIV Infections, CombinationspathuriNo ratings yet
- Integrated Disease Management: Basic ConceptDocument8 pagesIntegrated Disease Management: Basic ConceptNidhi SinghNo ratings yet
- Association of Low Serum 25-Hydroxyvitamin D Levels and Mortality in The Critically IllDocument7 pagesAssociation of Low Serum 25-Hydroxyvitamin D Levels and Mortality in The Critically Illdarius2311No ratings yet
- Pneumonia Trat 2012Document8 pagesPneumonia Trat 2012tcroscaNo ratings yet
- Antiviral Activity in Vitro: in Vitro Against HIV-2, With Similar Potency As Observed Against HIV-1Document30 pagesAntiviral Activity in Vitro: in Vitro Against HIV-2, With Similar Potency As Observed Against HIV-1pathuriNo ratings yet
- Vaccine and Basic Concepts of AEFIDocument35 pagesVaccine and Basic Concepts of AEFIFoyye MergaNo ratings yet
- Analysis Plan Final1Document9 pagesAnalysis Plan Final1Humphrey MisiriNo ratings yet
- Imunisasi Pada Kesehatan Masyarakat Di Indonesia Dan Pelaksanaan Safe InjectionDocument90 pagesImunisasi Pada Kesehatan Masyarakat Di Indonesia Dan Pelaksanaan Safe InjectionPuji Arifianti RamadhanyNo ratings yet
- NW PepDocument71 pagesNW PepRupali MukhijaNo ratings yet
- HBV, HCV, and HIV in The Dental Office Prevention and Recommendations For Post Exposure Prophylaxis (PEP)Document71 pagesHBV, HCV, and HIV in The Dental Office Prevention and Recommendations For Post Exposure Prophylaxis (PEP)Rajneesh JindalNo ratings yet
- GEMINI 1 y 2Document9 pagesGEMINI 1 y 2nacxit6No ratings yet
- Risk Factors For Severe Anaphylaxis in Patients Receiving Anaphylaxis Treatment in US Emergency Departments and HospitalsDocument6 pagesRisk Factors For Severe Anaphylaxis in Patients Receiving Anaphylaxis Treatment in US Emergency Departments and HospitalsAngga Aryo LukmantoNo ratings yet
- Polycythemia Vera and Essential ThrombocythemiaDocument10 pagesPolycythemia Vera and Essential ThrombocythemiaNichole BrownNo ratings yet
- Vaccine HIVDocument7 pagesVaccine HIVAbramo Abrahams FratusNo ratings yet
- Delirium ProphylaxisDocument7 pagesDelirium Prophylaxismohammed isam al hajNo ratings yet
- Pfizer/BiontechDocument1 pagePfizer/BiontechVIẾT HÀNo ratings yet
- DECAL LNH Refrac JCO 2001Document7 pagesDECAL LNH Refrac JCO 2001sunrasta23No ratings yet
- 2009-10-16 Current Antiviral Recommendations For Influenza TreatmentDocument2 pages2009-10-16 Current Antiviral Recommendations For Influenza Treatmenttamiprior5294No ratings yet
- Delirium: in The ClinicDocument16 pagesDelirium: in The Clinicmedal6No ratings yet
- Hemophila 190121092014Document46 pagesHemophila 190121092014interna MANADONo ratings yet
- Hivss2019 Paredes R. Intro To Pathophysiology of HivDocument65 pagesHivss2019 Paredes R. Intro To Pathophysiology of Hivjhonny12321No ratings yet
- Hiv 09 58Document13 pagesHiv 09 58dewiNo ratings yet
- Adr PDFDocument71 pagesAdr PDFVaibhav ThoratNo ratings yet
- PharmacovigillanceDocument36 pagesPharmacovigillanceSiti Hajar Nur SafitaNo ratings yet
- REITHINGERCID2055Document8 pagesREITHINGERCID2055Wulan YuwitaNo ratings yet
- VZV Clinical Slideset Jul2010Document57 pagesVZV Clinical Slideset Jul2010rtoroblesNo ratings yet
- J Jfms 2011 03 010Document14 pagesJ Jfms 2011 03 010Muhammad Fernanda DanuartaNo ratings yet
- Communicating The Benefits and Risks of VaccinesDocument8 pagesCommunicating The Benefits and Risks of VaccinesBrandeice BarrettNo ratings yet
- Fluvoxamine For COVID-19Document66 pagesFluvoxamine For COVID-19Vijay GauravNo ratings yet
- Journal of Research and Practice: SurgeryDocument22 pagesJournal of Research and Practice: SurgeryAthenaeum Scientific PublishersNo ratings yet
- Modified Morisky ScaleDocument7 pagesModified Morisky ScaleLeong YungNo ratings yet
- 31 5 1155Document9 pages31 5 1155operation_cloudburstNo ratings yet
- Virologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementFrom EverandVirologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementNo ratings yet
- Soft Copy of Activity Manual Supply Chain Management MedicineDocument40 pagesSoft Copy of Activity Manual Supply Chain Management MedicineRyanNo ratings yet
- Grapefruit MonographDocument4 pagesGrapefruit Monographjn007jnNo ratings yet
- NO Kodebarang Satuan Pakai Stock Awal Masuk Keluar Stock Akhir Harga KeteranganDocument4 pagesNO Kodebarang Satuan Pakai Stock Awal Masuk Keluar Stock Akhir Harga Keteranganruang belajar farmasiNo ratings yet
- Pharmacologically Active Constituents in PlantsDocument2 pagesPharmacologically Active Constituents in Plantsdarshan baskarNo ratings yet
- Pharmaco-Analytical Study and Phytochemical Profile of Hydroethanolic Extract of Algerian Prickly Pear (Opuntia Ficus-Indica.l)Document12 pagesPharmaco-Analytical Study and Phytochemical Profile of Hydroethanolic Extract of Algerian Prickly Pear (Opuntia Ficus-Indica.l)lotfi9No ratings yet
- IV Drugs CalculationDocument87 pagesIV Drugs CalculationAtiq KhanNo ratings yet
- Pharmacology Ms. Meenu Bhati (Asst. Prof. at CBS) ParasympathomimeticsDocument4 pagesPharmacology Ms. Meenu Bhati (Asst. Prof. at CBS) ParasympathomimeticsDAMBALENo ratings yet
- Technical Information On METHOCELDocument14 pagesTechnical Information On METHOCELPhạm ViệtNo ratings yet
- Company Profile Incepta PharmaDocument9 pagesCompany Profile Incepta PharmaNobo AhmedNo ratings yet
- Principles of Drug AdministrationDocument6 pagesPrinciples of Drug AdministrationEmman NuelleNo ratings yet
- Instructions For Filling Out Form Fda 356H - Application To Market A New or Abbreviated New Drug or Biologic For Human UseDocument3 pagesInstructions For Filling Out Form Fda 356H - Application To Market A New or Abbreviated New Drug or Biologic For Human UseSiva PrasadNo ratings yet
- Stok 16 Juni 2023Document62 pagesStok 16 Juni 2023Icha FransiscaNo ratings yet
- Model Pharmacy in BangladeshDocument7 pagesModel Pharmacy in BangladeshMoinuddin Khan KafiNo ratings yet
- Medicinal Chemistry Unit 5Document98 pagesMedicinal Chemistry Unit 5Prasanna ReddyNo ratings yet
- Fentanyl NeomedDocument3 pagesFentanyl NeomedmuarifNo ratings yet
- GC Packaging Distribution Ec MTG Exec SummaryDocument2 pagesGC Packaging Distribution Ec MTG Exec SummarymeiNo ratings yet
- Celpure®: High Purity Diatomite Filter MediaDocument2 pagesCelpure®: High Purity Diatomite Filter MediaMeira FontalvoNo ratings yet
- Pharmaceutical Legislation & History: Philippine Pharmaceutical Regulatory Affairs, Laws & EthicsDocument79 pagesPharmaceutical Legislation & History: Philippine Pharmaceutical Regulatory Affairs, Laws & EthicsCristine ChubiboNo ratings yet
- 472-Article Text-3477-1-10-20220326Document8 pages472-Article Text-3477-1-10-20220326Rianne MoralesNo ratings yet
- Small Volume Parenterals by MVRR2Document37 pagesSmall Volume Parenterals by MVRR2mvrr9100% (3)
- 990 1958 2 PBDocument10 pages990 1958 2 PBHeristiana PratiwiNo ratings yet
- Nurdr Practice QuestionsDocument6 pagesNurdr Practice QuestionsSHEENA MAE DE LOS REYESNo ratings yet
- Pharmacology: Introduction To Nursing PharmacologyDocument10 pagesPharmacology: Introduction To Nursing PharmacologyMarianne Joyce ManzoNo ratings yet
- Mediplant PDFDocument58 pagesMediplant PDFDnyaneshwar Dattatraya Phadatare100% (1)
- Aurobindo Pharma - Group8 - Sec-CDocument12 pagesAurobindo Pharma - Group8 - Sec-CBharadwaja JoshiNo ratings yet
- Development and Validation of A RP-HPLC Method ForDocument5 pagesDevelopment and Validation of A RP-HPLC Method ForabasNo ratings yet
- Chapter 311 Laws of BelizeDocument37 pagesChapter 311 Laws of Belizeamber castilloNo ratings yet
- Tablet ProblemsDocument3 pagesTablet ProblemsamitrameshwardayalNo ratings yet






















































































Download as pdf or txt
You might also like
- Production of Tablets and CapsulesDocument32 pagesProduction of Tablets and Capsulesraviteja79173% (15)
- The Importance of AdherenceDocument28 pagesThe Importance of AdherenceVijay LaptopNo ratings yet
- Tetanus: A Case ReportDocument2 pagesTetanus: A Case ReportrkotichaNo ratings yet
- Antibiotic and Oral Contraceptive Drug Interactions: Is There A Need For Concern?Document6 pagesAntibiotic and Oral Contraceptive Drug Interactions: Is There A Need For Concern?Eva SefianaNo ratings yet
- The Impact of COVID-19 On The Quality of Admission Clerkings On An Old Age Psychiatry Ward - An AuditDocument3 pagesThe Impact of COVID-19 On The Quality of Admission Clerkings On An Old Age Psychiatry Ward - An Auditkuda69790No ratings yet
- Hepatitis A and Hepatitis A VaccineDocument31 pagesHepatitis A and Hepatitis A VaccinedydinNo ratings yet
- Kenya Health Sector Strategic Investment Plan 2013 To 2017Document100 pagesKenya Health Sector Strategic Investment Plan 2013 To 2017GEOFFREY KAMBUNINo ratings yet
- 11 AdherenceDocument33 pages11 AdherenceCalvin ChisangoNo ratings yet
- A Critical Review Evaluation of The Efficacy of Covid19 Vaccines in EnglandDocument14 pagesA Critical Review Evaluation of The Efficacy of Covid19 Vaccines in EnglandvalgurNo ratings yet
- CCO Cytokine TX in MM ExpressPointsDocument18 pagesCCO Cytokine TX in MM ExpressPointsveaceslav coscodanNo ratings yet
- Prevention Strategy of Infectious Diseases For Health Care WorkersDocument31 pagesPrevention Strategy of Infectious Diseases For Health Care WorkersarinNo ratings yet
- VIH Diagnóstico Reciente in The Clinic PDFDocument16 pagesVIH Diagnóstico Reciente in The Clinic PDFFernando ArancibiaNo ratings yet
- Phase II Study of Vicriviroc Versus Efavirenz (Both With Zidovudine/Lamivudine) in Treatment-Naive Subjects With HIV-1 InfectionDocument10 pagesPhase II Study of Vicriviroc Versus Efavirenz (Both With Zidovudine/Lamivudine) in Treatment-Naive Subjects With HIV-1 Infectionverra sitanggangNo ratings yet
- Antibody PDFDocument2 pagesAntibody PDFStef DygaNo ratings yet
- Management of MRSA NP: Slide ReferenceDocument29 pagesManagement of MRSA NP: Slide ReferenceDermawan SolehNo ratings yet
- A Prospective Study On The Practice of Conversion of Antibiotics From IV To Oral Route and The Barriers Affecting ItDocument3 pagesA Prospective Study On The Practice of Conversion of Antibiotics From IV To Oral Route and The Barriers Affecting ItInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Immunodeficiency: Abdul Ghaffar, Ph.D. E-Mail: Ghaffar@med - Sc.eduDocument10 pagesImmunodeficiency: Abdul Ghaffar, Ph.D. E-Mail: Ghaffar@med - Sc.eduAhmed Goma'aNo ratings yet
- Bone Marrow Transplant Recent Advances and Nursing ImplicationsDocument18 pagesBone Marrow Transplant Recent Advances and Nursing ImplicationsRob BordenNo ratings yet
- Ruxolitinib Cream For Treatment of Vitiligo: A Randomised, Controlled, Phase 2 TrialDocument11 pagesRuxolitinib Cream For Treatment of Vitiligo: A Randomised, Controlled, Phase 2 TrialDORIS Z.No ratings yet
- HHS Public Access: HIV-1 Drug Resistance and Resistance TestingDocument42 pagesHHS Public Access: HIV-1 Drug Resistance and Resistance TestingAlfiraNo ratings yet
- Clinical Policy: Donor Lymphocyte Infusion: Coding Implications Revision Log Important ReminderDocument7 pagesClinical Policy: Donor Lymphocyte Infusion: Coding Implications Revision Log Important ReminderAlfajriekaputraNo ratings yet
- DFDFDFDFDocument10 pagesDFDFDFDFkclaportNo ratings yet
- Nac Leve Puntos Finales Diseño de Estudios Cid 2008Document5 pagesNac Leve Puntos Finales Diseño de Estudios Cid 2008Gustavo GomezNo ratings yet
- Day 1 5 MMC BootcampDocument40 pagesDay 1 5 MMC BootcampDianne Erika MeguinesNo ratings yet
- Shifts in Healthcare Demand, Delivery and Care During The COVID-19 EraDocument33 pagesShifts in Healthcare Demand, Delivery and Care During The COVID-19 EraMassimo RiserboNo ratings yet
- Mallik Questions ReplyDocument9 pagesMallik Questions ReplysanthoshNo ratings yet
- BIDMC HIV Manual 2019Document97 pagesBIDMC HIV Manual 2019oluNo ratings yet
- RevChilInfectol2015 VIHUPCDocument11 pagesRevChilInfectol2015 VIHUPCPaola GalarzaNo ratings yet
- Pharmacotherapeutic Group: Antivirals For Treatment of HIV Infections, CombinationsDocument30 pagesPharmacotherapeutic Group: Antivirals For Treatment of HIV Infections, CombinationspathuriNo ratings yet
- Integrated Disease Management: Basic ConceptDocument8 pagesIntegrated Disease Management: Basic ConceptNidhi SinghNo ratings yet
- Association of Low Serum 25-Hydroxyvitamin D Levels and Mortality in The Critically IllDocument7 pagesAssociation of Low Serum 25-Hydroxyvitamin D Levels and Mortality in The Critically Illdarius2311No ratings yet
- Pneumonia Trat 2012Document8 pagesPneumonia Trat 2012tcroscaNo ratings yet
- Antiviral Activity in Vitro: in Vitro Against HIV-2, With Similar Potency As Observed Against HIV-1Document30 pagesAntiviral Activity in Vitro: in Vitro Against HIV-2, With Similar Potency As Observed Against HIV-1pathuriNo ratings yet
- Vaccine and Basic Concepts of AEFIDocument35 pagesVaccine and Basic Concepts of AEFIFoyye MergaNo ratings yet
- Analysis Plan Final1Document9 pagesAnalysis Plan Final1Humphrey MisiriNo ratings yet
- Imunisasi Pada Kesehatan Masyarakat Di Indonesia Dan Pelaksanaan Safe InjectionDocument90 pagesImunisasi Pada Kesehatan Masyarakat Di Indonesia Dan Pelaksanaan Safe InjectionPuji Arifianti RamadhanyNo ratings yet
- NW PepDocument71 pagesNW PepRupali MukhijaNo ratings yet
- HBV, HCV, and HIV in The Dental Office Prevention and Recommendations For Post Exposure Prophylaxis (PEP)Document71 pagesHBV, HCV, and HIV in The Dental Office Prevention and Recommendations For Post Exposure Prophylaxis (PEP)Rajneesh JindalNo ratings yet
- GEMINI 1 y 2Document9 pagesGEMINI 1 y 2nacxit6No ratings yet
- Risk Factors For Severe Anaphylaxis in Patients Receiving Anaphylaxis Treatment in US Emergency Departments and HospitalsDocument6 pagesRisk Factors For Severe Anaphylaxis in Patients Receiving Anaphylaxis Treatment in US Emergency Departments and HospitalsAngga Aryo LukmantoNo ratings yet
- Polycythemia Vera and Essential ThrombocythemiaDocument10 pagesPolycythemia Vera and Essential ThrombocythemiaNichole BrownNo ratings yet
- Vaccine HIVDocument7 pagesVaccine HIVAbramo Abrahams FratusNo ratings yet
- Delirium ProphylaxisDocument7 pagesDelirium Prophylaxismohammed isam al hajNo ratings yet
- Pfizer/BiontechDocument1 pagePfizer/BiontechVIẾT HÀNo ratings yet
- DECAL LNH Refrac JCO 2001Document7 pagesDECAL LNH Refrac JCO 2001sunrasta23No ratings yet
- 2009-10-16 Current Antiviral Recommendations For Influenza TreatmentDocument2 pages2009-10-16 Current Antiviral Recommendations For Influenza Treatmenttamiprior5294No ratings yet
- Delirium: in The ClinicDocument16 pagesDelirium: in The Clinicmedal6No ratings yet
- Hemophila 190121092014Document46 pagesHemophila 190121092014interna MANADONo ratings yet
- Hivss2019 Paredes R. Intro To Pathophysiology of HivDocument65 pagesHivss2019 Paredes R. Intro To Pathophysiology of Hivjhonny12321No ratings yet
- Hiv 09 58Document13 pagesHiv 09 58dewiNo ratings yet
- Adr PDFDocument71 pagesAdr PDFVaibhav ThoratNo ratings yet
- PharmacovigillanceDocument36 pagesPharmacovigillanceSiti Hajar Nur SafitaNo ratings yet
- REITHINGERCID2055Document8 pagesREITHINGERCID2055Wulan YuwitaNo ratings yet
- VZV Clinical Slideset Jul2010Document57 pagesVZV Clinical Slideset Jul2010rtoroblesNo ratings yet
- J Jfms 2011 03 010Document14 pagesJ Jfms 2011 03 010Muhammad Fernanda DanuartaNo ratings yet
- Communicating The Benefits and Risks of VaccinesDocument8 pagesCommunicating The Benefits and Risks of VaccinesBrandeice BarrettNo ratings yet
- Fluvoxamine For COVID-19Document66 pagesFluvoxamine For COVID-19Vijay GauravNo ratings yet
- Journal of Research and Practice: SurgeryDocument22 pagesJournal of Research and Practice: SurgeryAthenaeum Scientific PublishersNo ratings yet
- Modified Morisky ScaleDocument7 pagesModified Morisky ScaleLeong YungNo ratings yet
- 31 5 1155Document9 pages31 5 1155operation_cloudburstNo ratings yet
- Virologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementFrom EverandVirologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementNo ratings yet
- Soft Copy of Activity Manual Supply Chain Management MedicineDocument40 pagesSoft Copy of Activity Manual Supply Chain Management MedicineRyanNo ratings yet
- Grapefruit MonographDocument4 pagesGrapefruit Monographjn007jnNo ratings yet
- NO Kodebarang Satuan Pakai Stock Awal Masuk Keluar Stock Akhir Harga KeteranganDocument4 pagesNO Kodebarang Satuan Pakai Stock Awal Masuk Keluar Stock Akhir Harga Keteranganruang belajar farmasiNo ratings yet
- Pharmacologically Active Constituents in PlantsDocument2 pagesPharmacologically Active Constituents in Plantsdarshan baskarNo ratings yet
- Pharmaco-Analytical Study and Phytochemical Profile of Hydroethanolic Extract of Algerian Prickly Pear (Opuntia Ficus-Indica.l)Document12 pagesPharmaco-Analytical Study and Phytochemical Profile of Hydroethanolic Extract of Algerian Prickly Pear (Opuntia Ficus-Indica.l)lotfi9No ratings yet
- IV Drugs CalculationDocument87 pagesIV Drugs CalculationAtiq KhanNo ratings yet
- Pharmacology Ms. Meenu Bhati (Asst. Prof. at CBS) ParasympathomimeticsDocument4 pagesPharmacology Ms. Meenu Bhati (Asst. Prof. at CBS) ParasympathomimeticsDAMBALENo ratings yet
- Technical Information On METHOCELDocument14 pagesTechnical Information On METHOCELPhạm ViệtNo ratings yet
- Company Profile Incepta PharmaDocument9 pagesCompany Profile Incepta PharmaNobo AhmedNo ratings yet
- Principles of Drug AdministrationDocument6 pagesPrinciples of Drug AdministrationEmman NuelleNo ratings yet
- Instructions For Filling Out Form Fda 356H - Application To Market A New or Abbreviated New Drug or Biologic For Human UseDocument3 pagesInstructions For Filling Out Form Fda 356H - Application To Market A New or Abbreviated New Drug or Biologic For Human UseSiva PrasadNo ratings yet
- Stok 16 Juni 2023Document62 pagesStok 16 Juni 2023Icha FransiscaNo ratings yet
- Model Pharmacy in BangladeshDocument7 pagesModel Pharmacy in BangladeshMoinuddin Khan KafiNo ratings yet
- Medicinal Chemistry Unit 5Document98 pagesMedicinal Chemistry Unit 5Prasanna ReddyNo ratings yet
- Fentanyl NeomedDocument3 pagesFentanyl NeomedmuarifNo ratings yet
- GC Packaging Distribution Ec MTG Exec SummaryDocument2 pagesGC Packaging Distribution Ec MTG Exec SummarymeiNo ratings yet
- Celpure®: High Purity Diatomite Filter MediaDocument2 pagesCelpure®: High Purity Diatomite Filter MediaMeira FontalvoNo ratings yet
- Pharmaceutical Legislation & History: Philippine Pharmaceutical Regulatory Affairs, Laws & EthicsDocument79 pagesPharmaceutical Legislation & History: Philippine Pharmaceutical Regulatory Affairs, Laws & EthicsCristine ChubiboNo ratings yet
- 472-Article Text-3477-1-10-20220326Document8 pages472-Article Text-3477-1-10-20220326Rianne MoralesNo ratings yet
- Small Volume Parenterals by MVRR2Document37 pagesSmall Volume Parenterals by MVRR2mvrr9100% (3)
- 990 1958 2 PBDocument10 pages990 1958 2 PBHeristiana PratiwiNo ratings yet
- Nurdr Practice QuestionsDocument6 pagesNurdr Practice QuestionsSHEENA MAE DE LOS REYESNo ratings yet
- Pharmacology: Introduction To Nursing PharmacologyDocument10 pagesPharmacology: Introduction To Nursing PharmacologyMarianne Joyce ManzoNo ratings yet
- Mediplant PDFDocument58 pagesMediplant PDFDnyaneshwar Dattatraya Phadatare100% (1)
- Aurobindo Pharma - Group8 - Sec-CDocument12 pagesAurobindo Pharma - Group8 - Sec-CBharadwaja JoshiNo ratings yet
- Development and Validation of A RP-HPLC Method ForDocument5 pagesDevelopment and Validation of A RP-HPLC Method ForabasNo ratings yet
- Chapter 311 Laws of BelizeDocument37 pagesChapter 311 Laws of Belizeamber castilloNo ratings yet
- Tablet ProblemsDocument3 pagesTablet ProblemsamitrameshwardayalNo ratings yet