Download as pdf or txt
You might also like
- Blood TransfusionDocument59 pagesBlood Transfusionpranalika .................76% (17)
- Herbs and Healing PDFDocument14 pagesHerbs and Healing PDFDavid SeraciniNo ratings yet
- Student Feedback VT CorrectionsDocument6 pagesStudent Feedback VT Correctionsapi-300353332No ratings yet
- Requirements For OVP Medical AssistanceDocument1 pageRequirements For OVP Medical AssistanceOVP Media67% (6)
- Gonadal Hormones and InhibitorsDocument14 pagesGonadal Hormones and InhibitorsbluesumNo ratings yet
- Sex Hormones PDFDocument54 pagesSex Hormones PDFmohsen mirdamadiNo ratings yet
- Contraception Lec 1Document38 pagesContraception Lec 1fh2785519No ratings yet
- Drugs Affecting The FemaleDocument32 pagesDrugs Affecting The FemaleLule Allan PhillipNo ratings yet
- ContraceptionDocument39 pagesContraceptionapi-3705046100% (3)
- Hormonal Contraception: Oral, Parenteral and Implanted ContraceptivesDocument14 pagesHormonal Contraception: Oral, Parenteral and Implanted ContraceptivesFrancia ToledanoNo ratings yet
- Contraception: Fertility Control Which Ideally Should Be Reliable, Inexpensive, Safe and Easy To UseDocument39 pagesContraception: Fertility Control Which Ideally Should Be Reliable, Inexpensive, Safe and Easy To UseJan Jamison ZuluetaNo ratings yet
- Unit 8 Drugs Acting On The Endocrine SystemDocument26 pagesUnit 8 Drugs Acting On The Endocrine SystemTherese Margarette SantiagoNo ratings yet
- Sex Hormones - 2023 PDFDocument49 pagesSex Hormones - 2023 PDFmohsen mirdamadiNo ratings yet
- Female Reproductive System DrugsDocument84 pagesFemale Reproductive System DrugsPrincess C. SultanNo ratings yet
- EstorgenDocument34 pagesEstorgenAbubakar JallohNo ratings yet
- Pharma Report Reproductive SystemDocument18 pagesPharma Report Reproductive SystemDolly Jane JavierNo ratings yet
- 07 Miscellaneous Drugs Group ADocument64 pages07 Miscellaneous Drugs Group AKamal GhimireNo ratings yet
- ContraceptionDocument44 pagesContraceptionmustafa atayaNo ratings yet
- Drugs Used in Reproductive Health: Estrogen and ProgestinDocument41 pagesDrugs Used in Reproductive Health: Estrogen and ProgestindrfatimarizNo ratings yet
- Oestrogen, Progesterone, AndrogensDocument58 pagesOestrogen, Progesterone, AndrogensTandin Sonam100% (1)
- SajanDocument28 pagesSajanSajan ChoudharyNo ratings yet
- Metabolic and Endocrine Pharmacology: Gonadol DrugsDocument38 pagesMetabolic and Endocrine Pharmacology: Gonadol Drugstheintrov100% (1)
- Family Planning MethodsDocument130 pagesFamily Planning MethodsDIPENDRA KUMAR KUSHAWAHANo ratings yet
- Endocrine and GI Pharmacology 2020Document19 pagesEndocrine and GI Pharmacology 2020JanelleNo ratings yet
- New Estrogen and ProgesteroneDocument56 pagesNew Estrogen and ProgesteroneHBr100% (1)
- Family Planning: By: Khalid Jemal (MD, Assistant Prof. of Obstetrics & Gynecology)Document73 pagesFamily Planning: By: Khalid Jemal (MD, Assistant Prof. of Obstetrics & Gynecology)Degefaw BikoyNo ratings yet
- Dwi Indria Anggraini Faculty of Medicine Lampung UniversityDocument16 pagesDwi Indria Anggraini Faculty of Medicine Lampung UniversitysyiefarenandaNo ratings yet
- Hormone Replacement TherapyDocument24 pagesHormone Replacement TherapyZai Akma100% (2)
- Progestins AND AntiprogestinsDocument41 pagesProgestins AND Antiprogestinsdrfatimariz100% (1)
- Gonadal Hormones 62594Document98 pagesGonadal Hormones 62594TES SENNo ratings yet
- Drugs Acting On Genitourinary System of AnimalsDocument44 pagesDrugs Acting On Genitourinary System of AnimalsSunilNo ratings yet
- Tamoxifen CitrateDocument3 pagesTamoxifen Citrateapi-3797941No ratings yet
- MED 4 CAS 2 Pharm ChartDocument7 pagesMED 4 CAS 2 Pharm Chartnaazaninrahat76No ratings yet
- Management of Infertile CoupleDocument29 pagesManagement of Infertile CoupleSaneem AnwerNo ratings yet
- Presentation 1Document58 pagesPresentation 1Kuch Bhi50% (2)
- Sex HarmoneDocument22 pagesSex Harmonesuyash jainNo ratings yet
- Drugs Affecting The Female Reproductive SystemDocument27 pagesDrugs Affecting The Female Reproductive Systemadrianleet18No ratings yet
- Progestins: DR Suyash Bharat MD Pharmacology GMC HaldwaniDocument27 pagesProgestins: DR Suyash Bharat MD Pharmacology GMC HaldwanidrfatimarizNo ratings yet
- Drug Study #3Document4 pagesDrug Study #3Sarah Kaye BañoNo ratings yet
- Severe Cramps or Pelvic Pain, Pain During Intercourse, Extreme Dizziness, Lightheadedness, Severe Migraine HeadacheDocument2 pagesSevere Cramps or Pelvic Pain, Pain During Intercourse, Extreme Dizziness, Lightheadedness, Severe Migraine HeadacheChristian LancelotNo ratings yet
- AndrogensDocument63 pagesAndrogensSantu Prashu50% (2)
- Steroids JenniferKettelDocument25 pagesSteroids JenniferKettelvinay0717No ratings yet
- Progesterone in PregnancyDocument59 pagesProgesterone in PregnancyKaruna Indoliya100% (2)
- Oestrogens & Phytoestrogens ProgestrogensDocument127 pagesOestrogens & Phytoestrogens ProgestrogensSheerazNo ratings yet
- K16 - Pharmacology of Hormonal ContraceptionDocument51 pagesK16 - Pharmacology of Hormonal Contraceptiondhiyas100% (1)
- Contraception Family PlaningDocument74 pagesContraception Family PlaningEyob MizanNo ratings yet
- AndrogenDocument19 pagesAndrogenTamam JauharNo ratings yet
- Drugs Affecting Reproduction: DR - R - PrameelaDocument76 pagesDrugs Affecting Reproduction: DR - R - PrameelaRamadi PrameelaNo ratings yet
- The Use of Hormones in Gynaecological PracticeDocument24 pagesThe Use of Hormones in Gynaecological PracticeMuhammad AmeenNo ratings yet
- Contraception: Oral ContraceptivesDocument24 pagesContraception: Oral Contraceptivesnasir_ali7846No ratings yet
- The IVF Problem Patient: Pre-Existing Diseases in Infertile PatientsDocument14 pagesThe IVF Problem Patient: Pre-Existing Diseases in Infertile PatientsRyan Bianet CosicolNo ratings yet
- Infertility NirwenDocument55 pagesInfertility Nirwenpok yeahNo ratings yet
- Female Hormonal TherapyDocument38 pagesFemale Hormonal TherapySA NodeNo ratings yet
- Pharmacology of Sex SteroidsDocument40 pagesPharmacology of Sex Steroidsmus zaharaNo ratings yet
- Classification of Drug Name of Drug Pharmacokinetics Toxicity/Side EffectsDocument23 pagesClassification of Drug Name of Drug Pharmacokinetics Toxicity/Side EffectsDestiny Church ZamboangaNo ratings yet
- Menopause and HRTDocument35 pagesMenopause and HRTMelNo ratings yet
- Contraceptive Pharmacology Katz Com 2010Document41 pagesContraceptive Pharmacology Katz Com 2010Michael KatzNo ratings yet
- Parathyroid AgentsDocument36 pagesParathyroid AgentsGlaiza Joves EncarnacionNo ratings yet
- DR - Shameem R.AlaasamDocument31 pagesDR - Shameem R.Alaasamhacker ammerNo ratings yet
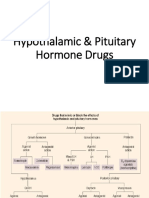
- Hypothalamic & Pituitary Hormone DrugsDocument29 pagesHypothalamic & Pituitary Hormone DrugsDylan MansillaNo ratings yet
- 10-Gonadal HormonesDocument9 pages10-Gonadal Hormonesmedical.student.messiNo ratings yet
- 5 ProgestogensDocument33 pages5 Progestogensmhmtrgnn67No ratings yet
- Anterior Pituitary AgentsDocument4 pagesAnterior Pituitary AgentsGab SanchezNo ratings yet
- My Mifespristone and Misoprostol Story: How I used mifepristone and misoprostol for a successful medical abortion and all you must know about these abortion pillsFrom EverandMy Mifespristone and Misoprostol Story: How I used mifepristone and misoprostol for a successful medical abortion and all you must know about these abortion pillsNo ratings yet
- Hypertensive Complications of PregnancyDocument37 pagesHypertensive Complications of PregnancyAlbert Francis BialaNo ratings yet
- Hepatic Biliary Tract and Pancreatic DisordersDocument26 pagesHepatic Biliary Tract and Pancreatic DisordersAlbert Francis BialaNo ratings yet
- Estrogen, Progestin and AndrogenDocument11 pagesEstrogen, Progestin and AndrogenAlbert Francis BialaNo ratings yet
- Primary Secondary DysmenorrheaDocument20 pagesPrimary Secondary DysmenorrheaAlbert Francis BialaNo ratings yet
- American College of Rheumatology Subcommittee On Osteoarthritis GuidelinesDocument17 pagesAmerican College of Rheumatology Subcommittee On Osteoarthritis GuidelinesAdrian MorosanNo ratings yet
- The Health Effect of Wood Smoke0Document2 pagesThe Health Effect of Wood Smoke0jhonrmdNo ratings yet
- Research Article: Kasturba Gandhi Nursing CollegeDocument5 pagesResearch Article: Kasturba Gandhi Nursing CollegesanthiyasandyNo ratings yet
- The Mahima of The Humble Tulsi in Our CourtyardDocument11 pagesThe Mahima of The Humble Tulsi in Our Courtyardsudhakardevarapalli100% (1)
- Baroudi Seroma - How To Avoid It and How To Treat ItDocument3 pagesBaroudi Seroma - How To Avoid It and How To Treat ItLuisCRNo ratings yet
- WISC IV Cross Culture ComparisonDocument21 pagesWISC IV Cross Culture ComparisongwzglNo ratings yet
- Antibody Identification: Part 1: The Basics A Blood Bank Guy Video PodcastDocument18 pagesAntibody Identification: Part 1: The Basics A Blood Bank Guy Video PodcastNguyen Thi Phuong NhiNo ratings yet
- ATI Flash Cards 03, Medications Affecting Immune SystemDocument40 pagesATI Flash Cards 03, Medications Affecting Immune Systemensoooooooooo0% (1)
- REMEDIAL EXAM Answer KeyDocument18 pagesREMEDIAL EXAM Answer KeyMark MasbadNo ratings yet
- Letter of Applicatin FinalDocument3 pagesLetter of Applicatin Finalapi-483670443No ratings yet
- Common Health Problems of Infancy PowptDocument78 pagesCommon Health Problems of Infancy PowptCiella Dela CruzNo ratings yet
- Hanuman Badabanala StotramDocument4 pagesHanuman Badabanala Stotrampramod yelagonda0% (1)
- Animal DentistryDocument10 pagesAnimal DentistryFei Fei LoNo ratings yet
- Olanzapine Drug StudyDocument5 pagesOlanzapine Drug Studyjohnlester_jlfNo ratings yet
- Healthy Michigan AssessmentDocument5 pagesHealthy Michigan AssessmentDevi PratiwiNo ratings yet
- Circulatory System Grades 5 To 7Document5 pagesCirculatory System Grades 5 To 7Jeff HagwonNo ratings yet
- 1 BellsPalsy PDFDocument14 pages1 BellsPalsy PDFSimbakutty VenkataramananNo ratings yet
- Mic Eales A Visual Enquiry Into SuicideDocument4 pagesMic Eales A Visual Enquiry Into Suicidemaribolla8015No ratings yet
- Microbiology Product Catalog EU enDocument94 pagesMicrobiology Product Catalog EU enArifin R HidayatNo ratings yet
- Dynamic Warm-Up Day 1 PDFDocument11 pagesDynamic Warm-Up Day 1 PDFtriflingNo ratings yet
- DGFHJKDocument3 pagesDGFHJKRavish MalhotraNo ratings yet
- Biglan, A. & Glenn, S. S. (2013) - Toward Prosocial Behavior and EnvironmentsDocument21 pagesBiglan, A. & Glenn, S. S. (2013) - Toward Prosocial Behavior and Environmentsregulus_caelum551No ratings yet
- Lista de Medicamentos Esenciales para Emergencias Radiológicas y NuclearesDocument66 pagesLista de Medicamentos Esenciales para Emergencias Radiológicas y NuclearesMartin GonzalezNo ratings yet
- Bougouin2022 Article EpinephrineVersusNorepinephrinDocument11 pagesBougouin2022 Article EpinephrineVersusNorepinephrinSaul RuizNo ratings yet
- Momcology 101: AnniversariesDocument2 pagesMomcology 101: AnniversariesEmily DeyoungNo ratings yet
- EpilepsyDocument11 pagesEpilepsyStella WatkinsNo ratings yet