Download as pdf or txt
You might also like
- Obesity and Asthma: E. Rand Sutherland, MD, MPHDocument14 pagesObesity and Asthma: E. Rand Sutherland, MD, MPHAsep HrNo ratings yet
- Gastro Oesophageal RefluxDocument7 pagesGastro Oesophageal Refluxjustifieda13No ratings yet
- Medical Hazards of Obesity: Ann Intern Med. 1993 119 (7 PT 2) :655-660Document6 pagesMedical Hazards of Obesity: Ann Intern Med. 1993 119 (7 PT 2) :655-660David WheelerNo ratings yet
- Obesity and AsthmaDocument26 pagesObesity and AsthmaDumitru BiniucNo ratings yet
- Taylor P 2016 IMC y HT NeonatoDocument9 pagesTaylor P 2016 IMC y HT NeonatoYHOISS SMIHT MUNOZ CERONNo ratings yet
- The Influence of Low Birth Weight On The Development of Asthma in ChildreDocument7 pagesThe Influence of Low Birth Weight On The Development of Asthma in ChildreLalaNo ratings yet
- Obesity and OsteoarthritisDocument13 pagesObesity and OsteoarthritisHelgaNo ratings yet
- Asthma and Obesity: Common Early-Life Influences in The Inception of DiseaseDocument10 pagesAsthma and Obesity: Common Early-Life Influences in The Inception of Diseaseracut_khansatraNo ratings yet
- 1 s2.0 S2666506920300055 MainDocument10 pages1 s2.0 S2666506920300055 MainVanni FierputeriNo ratings yet
- 2 Overweight, Obesity, and Depression - Areli López AlvaradoDocument10 pages2 Overweight, Obesity, and Depression - Areli López Alvaradomtz.c.erikaNo ratings yet
- Artigo Base 4Document8 pagesArtigo Base 4Cleo AlvesNo ratings yet
- Effect of Low Birth Weight On Childhood Asthma: A Meta-AnalysisDocument8 pagesEffect of Low Birth Weight On Childhood Asthma: A Meta-Analysisnavali rahmaNo ratings yet
- Early Life Body Fatness and Risk of Colon CancerDocument17 pagesEarly Life Body Fatness and Risk of Colon CancerNilufar K.No ratings yet
- Aipm 15 82Document6 pagesAipm 15 82Isini sehansa amarathungaNo ratings yet
- Ethnic Comparisons of The Cross-Sectional Relationships Between Measures of Body Size With Diabetes and HypertensionDocument9 pagesEthnic Comparisons of The Cross-Sectional Relationships Between Measures of Body Size With Diabetes and HypertensionDeedee RenovaldiNo ratings yet
- Jurnal JkmsDocument8 pagesJurnal JkmsArif Kurniawan ListiantoNo ratings yet
- Relation Sleep Obes and BPDocument18 pagesRelation Sleep Obes and BPMumtaz MaulanaNo ratings yet
- Association Between Body-Mass Index and Risk of Death in More Than 1 Million AsiansDocument11 pagesAssociation Between Body-Mass Index and Risk of Death in More Than 1 Million AsiansRhinie AstriyanaNo ratings yet
- Hostility and The Metabolic Syndrome in Older Males: The Normative Aging StudyDocument10 pagesHostility and The Metabolic Syndrome in Older Males: The Normative Aging StudymrclpppNo ratings yet
- Peters 2014Document10 pagesPeters 2014Andrew E P SunardiNo ratings yet
- 2017 Article 405Document11 pages2017 Article 405Kornelis AribowoNo ratings yet
- Asthma Journal Printtt2Document2 pagesAsthma Journal Printtt2everytimewithyou123No ratings yet
- Obesity and The Risk of Newly Diagnosed Asthma in School-Age ChildrenDocument10 pagesObesity and The Risk of Newly Diagnosed Asthma in School-Age ChildrenMar LindaNo ratings yet
- Population-Wide Analysis of Differences in Disease Progression Patterns in Men and WomenDocument14 pagesPopulation-Wide Analysis of Differences in Disease Progression Patterns in Men and WomenSagar SononeNo ratings yet
- Am J Clin Nutr 2007 Larsson 556 65Document10 pagesAm J Clin Nutr 2007 Larsson 556 65Safira T LNo ratings yet
- Body Mass Index, Waist Circumference and Waist:hip Ratio As Predictors of Cardiovascular Risk-A Review of The LiteratureDocument7 pagesBody Mass Index, Waist Circumference and Waist:hip Ratio As Predictors of Cardiovascular Risk-A Review of The LiteratureBenedetta AgnelliNo ratings yet
- Combination of Measures For Obesity and New-Onset Gallstone Disease 20.16.02Document11 pagesCombination of Measures For Obesity and New-Onset Gallstone Disease 20.16.02hasri ainunNo ratings yet
- 2021 Relation of Body Fat Mass and Fat Free Mass To Total MortalityDocument8 pages2021 Relation of Body Fat Mass and Fat Free Mass To Total MortalityLina M GarciaNo ratings yet
- LC1 BMI and All-Cause Mortality in Older AdultsDocument16 pagesLC1 BMI and All-Cause Mortality in Older AdultsMariNo ratings yet
- Body Mass Index ObesityDocument8 pagesBody Mass Index ObesityReyes Falcon D. ÁngelNo ratings yet
- Body Mass Index GERDDocument10 pagesBody Mass Index GERDlalalalaNo ratings yet
- Ijc 22717Document7 pagesIjc 22717Tony DávilaNo ratings yet
- Oby 21181Document13 pagesOby 21181Mayra de CáceresNo ratings yet
- I. Epidemiology and Genetics of AsthmaDocument7 pagesI. Epidemiology and Genetics of AsthmaVasincuAlexandruNo ratings yet
- Perceived Weight Discrimination Mediates The Prospective Relation Between Obesity and Depressive Symptoms in U.S. and U.K. AdultsDocument10 pagesPerceived Weight Discrimination Mediates The Prospective Relation Between Obesity and Depressive Symptoms in U.S. and U.K. AdultsRebeka meloNo ratings yet
- Obesity and Asthma: An Association Modified by Age of Asthma OnsetDocument10 pagesObesity and Asthma: An Association Modified by Age of Asthma OnsetSteve aokiNo ratings yet
- Association of Underweight Status With The Risk of Tuberculosis: A Nationwide Population Based Cohort StudyDocument8 pagesAssociation of Underweight Status With The Risk of Tuberculosis: A Nationwide Population Based Cohort StudygregoriusbudisetiawaNo ratings yet
- Obesidad y AsmaDocument8 pagesObesidad y AsmaLuis FelipeNo ratings yet
- Overweight and Obesity Associated With Higher Depression Prevalence in Adults: A Systematic Review and Meta-AnalysisDocument12 pagesOverweight and Obesity Associated With Higher Depression Prevalence in Adults: A Systematic Review and Meta-AnalysisLev FyodorNo ratings yet
- Anthropometrical Parameters Are Not Related With Lipid Profile in Mild To Moderate AsthmaDocument5 pagesAnthropometrical Parameters Are Not Related With Lipid Profile in Mild To Moderate AsthmaOpenaccess Research paperNo ratings yet
- Thừa cân, béo phì liên quan đến nhiều loại bệnh tật nguy hiểm-wed HarvardDocument24 pagesThừa cân, béo phì liên quan đến nhiều loại bệnh tật nguy hiểm-wed HarvardNam NguyenHoangNo ratings yet
- Jurnal Etiologi (EBM)Document9 pagesJurnal Etiologi (EBM)Dewi LarasatiNo ratings yet
- BBL, Imt, AsmaDocument7 pagesBBL, Imt, AsmaYenny Adelia 黃梅珠No ratings yet
- Ioi80217 764 7730Document7 pagesIoi80217 764 7730kern tranhNo ratings yet
- Epidemiology of Asthma and in Uence of EthnicityDocument9 pagesEpidemiology of Asthma and in Uence of EthnicitySyahrialNo ratings yet
- Insight On Pathogenesis of Lifelong Premature Ejaculation: Inverse Relationship Between Lifelong Premature Ejaculation and ObesityDocument4 pagesInsight On Pathogenesis of Lifelong Premature Ejaculation: Inverse Relationship Between Lifelong Premature Ejaculation and ObesitymaithamNo ratings yet
- Relationshipbetween RBSandobesityDocument2 pagesRelationshipbetween RBSandobesityasdNo ratings yet
- Public Health and The EyeDocument16 pagesPublic Health and The EyeAngkat Prasetya Abdi NegaraNo ratings yet
- A Prospective Study of Obesity and Incidence and Progession of Lower Urinary Tract SymptomsDocument13 pagesA Prospective Study of Obesity and Incidence and Progession of Lower Urinary Tract SymptomssusanaNo ratings yet
- Artigo 12Document17 pagesArtigo 12daisyscholliersNo ratings yet
- Eating Behaviors: Ricarda Ohlmer, Corinna Jacobi, Eike FittigDocument4 pagesEating Behaviors: Ricarda Ohlmer, Corinna Jacobi, Eike FittigAna PasoleaNo ratings yet
- 5 DAVID L. STREINER, PHD, GEOFFREY R. NORMAN, PHD - PDQ Epidemiology-People's Medical Publishing House (2009)Document14 pages5 DAVID L. STREINER, PHD, GEOFFREY R. NORMAN, PHD - PDQ Epidemiology-People's Medical Publishing House (2009)Germán Eduardo Lagos SepúlvedaNo ratings yet
- Childhood Body Mass Index and Risk of Inflammatory Bowel Disease in Adulthood - A Population-Based Cohort StudyDocument8 pagesChildhood Body Mass Index and Risk of Inflammatory Bowel Disease in Adulthood - A Population-Based Cohort StudyWarren SeowNo ratings yet
- Obesity and DepressionDocument5 pagesObesity and DepressionTunde WilliamsNo ratings yet
- LAGACE Et Al. 2022 Increased Odds of Having The Metabolic Syndrome With Greater Fat Free MassDocument9 pagesLAGACE Et Al. 2022 Increased Odds of Having The Metabolic Syndrome With Greater Fat Free MassFrancisco MenezesNo ratings yet
- Body Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisDocument7 pagesBody Mass Index and Susceptibility To Knee Osteoarthritis: A Systematic Review and Meta-AnalysisAmalia RosaNo ratings yet
- Journal Pone 0248856Document15 pagesJournal Pone 0248856raihannah othmanNo ratings yet
- Migraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesDocument14 pagesMigraine and Body Mass Index Categories: A Systematic Review and Meta-Analysis of Observational StudiesRetno ManggalihNo ratings yet
- Obesity and The Risk of Cryptogenic Ischemic Stroke in Young AdultsDocument25 pagesObesity and The Risk of Cryptogenic Ischemic Stroke in Young AdultsKhalilullah ArsyiNo ratings yet
- 649 FullDocument6 pages649 FullDumitru BiniucNo ratings yet
- Patophysiology of Lungs ObesityDocument6 pagesPatophysiology of Lungs ObesityDumitru BiniucNo ratings yet
- EU Baffi2016 - MetabDocument33 pagesEU Baffi2016 - MetabDumitru BiniucNo ratings yet
- Obesity Lung COPDDocument8 pagesObesity Lung COPDDumitru BiniucNo ratings yet
- 717 FullDocument11 pages717 FullDumitru BiniucNo ratings yet
- 1089 FullDocument9 pages1089 FullDumitru BiniucNo ratings yet
- Adipose Tissue in LungsDocument31 pagesAdipose Tissue in LungsDumitru BiniucNo ratings yet
- EU King2005Document6 pagesEU King2005Dumitru BiniucNo ratings yet
- EU 4.fullDocument5 pagesEU 4.fullDumitru BiniucNo ratings yet
- The Technology Boom: A New Era in Obesity ManagementDocument13 pagesThe Technology Boom: A New Era in Obesity ManagementDumitru BiniucNo ratings yet
- WHO Health Workforce Support and Safeguards ListDocument7 pagesWHO Health Workforce Support and Safeguards ListDumitru BiniucNo ratings yet
- Results of New Policies For Inpatient Rehabilitation Coverage in JapanDocument8 pagesResults of New Policies For Inpatient Rehabilitation Coverage in JapanDumitru BiniucNo ratings yet
- Rehabilitation - A New Approach. Overview and Part One: The ProblemsDocument10 pagesRehabilitation - A New Approach. Overview and Part One: The ProblemsDumitru BiniucNo ratings yet
- Evolutia in Abordarea Calitatii Serviciilor MedicaleDocument6 pagesEvolutia in Abordarea Calitatii Serviciilor MedicaleDumitru BiniucNo ratings yet
- Wylie 2007Document7 pagesWylie 2007Dumitru BiniucNo ratings yet
- Rehabilitation in The United Kingdom: Research, Policy, and PracticeDocument7 pagesRehabilitation in The United Kingdom: Research, Policy, and PracticeDumitru BiniucNo ratings yet
- Cornette 2011Document8 pagesCornette 2011Dumitru BiniucNo ratings yet
- JCM 09 03762Document9 pagesJCM 09 03762Dumitru BiniucNo ratings yet
- Cameron 2008Document11 pagesCameron 2008Dumitru BiniucNo ratings yet
- Eng PDFDocument52 pagesEng PDFDumitru BiniucNo ratings yet
- 2Document14 pages2Dumitru BiniucNo ratings yet
- 2Document14 pages2Dumitru BiniucNo ratings yet
- WRCC PTDocument2 pagesWRCC PTCHELSEA MAE SAULONo ratings yet
- The Benefits of Drug Education Reassessment and Policy ReformDocument7 pagesThe Benefits of Drug Education Reassessment and Policy Reformapi-316884204No ratings yet
- (Peter Ferrara) The Obamacare DisasterDocument78 pages(Peter Ferrara) The Obamacare DisasterYusuf KaripekNo ratings yet
- Serkom 2 Nov 2022Document25 pagesSerkom 2 Nov 2022donat mantulNo ratings yet
- Enhanced Recovery After SurgeryDocument47 pagesEnhanced Recovery After SurgeryPeri HidayatNo ratings yet
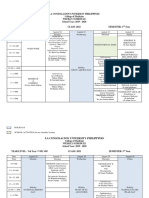
- Final3rd Year Schedule 1st Semester A.Y 2019-2020 As of August 21, 2019Document19 pagesFinal3rd Year Schedule 1st Semester A.Y 2019-2020 As of August 21, 2019Shannen Christelle AndradeNo ratings yet
- Variable List in ExcelDocument375 pagesVariable List in ExcelManhar HemantNo ratings yet
- Policy and Procedure Manual: Diagnostic Services - Department of Radiology - Diagnostic DivisionDocument5 pagesPolicy and Procedure Manual: Diagnostic Services - Department of Radiology - Diagnostic DivisionFriends ForeverNo ratings yet
- PRESENTATION: Aging and Human Resource Development of Elderly Persons' Care in Singapore and The PhilippinesDocument34 pagesPRESENTATION: Aging and Human Resource Development of Elderly Persons' Care in Singapore and The PhilippinesADB Health Sector Group100% (1)
- Siemens Saudi Arabia Country Profile 2010Document2 pagesSiemens Saudi Arabia Country Profile 2010Abu Ammar YasirNo ratings yet
- BS BuzzDocument8 pagesBS BuzzBS Central, Inc. "The Buzz"No ratings yet
- Lucknow Hospital TPA List 2021Document1 pageLucknow Hospital TPA List 2021sunnyNo ratings yet
- Global Health InitiativesDocument2 pagesGlobal Health InitiativesLily LunaNo ratings yet
- 2nd Announcement PIT XXIIDocument12 pages2nd Announcement PIT XXIIdr sutjiNo ratings yet
- Resume of Mary - HuthDocument1 pageResume of Mary - Huthapi-27971644No ratings yet
- The Road To Free Insulin: Guyana Case StudyDocument5 pagesThe Road To Free Insulin: Guyana Case StudyarmanNo ratings yet
- Staffdevelopment For NursesDocument33 pagesStaffdevelopment For NursesJoYCe75% (4)
- Full Download Health Economics and Policy 5th Edition Henderson Test BankDocument35 pagesFull Download Health Economics and Policy 5th Edition Henderson Test Bankzoism.waygoose.3fuhqv100% (32)
- The Study of Challenges Faced by Pharmaceutical IndustryDocument72 pagesThe Study of Challenges Faced by Pharmaceutical IndustryUmar MalikNo ratings yet
- Internship Report HR AUDITDocument37 pagesInternship Report HR AUDITAshish Joseph TirkeyNo ratings yet
- Lesson Plans k6Document13 pagesLesson Plans k6Regine Delfin AclaracionNo ratings yet
- Manager Healthcare Billing Coding in Baltimore MD Resume Patricia HeldoornDocument2 pagesManager Healthcare Billing Coding in Baltimore MD Resume Patricia HeldoornPatriciaHeldoornNo ratings yet
- TQM Implementation Practices and Performance Outcome of Indian Hospitals: Exploratory FindingsDocument22 pagesTQM Implementation Practices and Performance Outcome of Indian Hospitals: Exploratory FindingsLejandra MNo ratings yet
- Hospital Admission Form-4Document1 pageHospital Admission Form-4cebogoofythaiNo ratings yet
- Internship Report: Shree Guruji Pvt. LTDDocument4 pagesInternship Report: Shree Guruji Pvt. LTDAnonymous wXj9gDwvNo ratings yet
- 19-Urological-Infections 2017 Web PDFDocument64 pages19-Urological-Infections 2017 Web PDFUchy Luph'milimiLyNo ratings yet
- Hambatan Dalam Komunikasi TerapeutikDocument12 pagesHambatan Dalam Komunikasi TerapeutikMaulida ArifiantiNo ratings yet
- Christina Curriculum VitaeDocument3 pagesChristina Curriculum VitaedesignetgrNo ratings yet
- The Relationship Between Heavy Menstrual Bleeding, Iron Deficiency and Iron Deficiency AnemiaDocument9 pagesThe Relationship Between Heavy Menstrual Bleeding, Iron Deficiency and Iron Deficiency AnemiaKevin Stanley HalimNo ratings yet
- Guidelines On Medical Documents Retention in NigeriaDocument12 pagesGuidelines On Medical Documents Retention in NigeriaOluwasegun OluwaletiNo ratings yet