Download as pdf or txt
You might also like
- Case Analysis - Rosemont Hill Health Center - V3Document8 pagesCase Analysis - Rosemont Hill Health Center - V3thearpan100% (2)
- Illustrated Chinese Moxibustion Techniques and Methods - NodrmDocument371 pagesIllustrated Chinese Moxibustion Techniques and Methods - NodrmOsmany Amador94% (53)
- Specialist Rehabilitation in The Trauma Pathway BSRM Core StandardsDocument22 pagesSpecialist Rehabilitation in The Trauma Pathway BSRM Core StandardsDynamic NeuropsychologyNo ratings yet
- ArticleDocument6 pagesArticlecarlostororeumatologoNo ratings yet
- Adherence of Physical TherapyDocument9 pagesAdherence of Physical TherapyJingle BellsNo ratings yet
- Artigo 10 Reabili.Document15 pagesArtigo 10 Reabili.Gabriela GhissardiNo ratings yet
- Physiotherapists' Recommendations For Examination and Treatment of Rotator Cuff Related Shoulder PainDocument9 pagesPhysiotherapists' Recommendations For Examination and Treatment of Rotator Cuff Related Shoulder PainNadina WawrzykNo ratings yet
- Artikel 2 LDocument6 pagesArtikel 2 L.No ratings yet
- Williamson 2020Document11 pagesWilliamson 2020Franz CalumpitNo ratings yet
- The Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisDocument21 pagesThe Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-Analysisilham Maulana ArifNo ratings yet
- Ijccm 17 15Document11 pagesIjccm 17 15lakshminivas PingaliNo ratings yet
- AttendDocument3 pagesAttendAliRifqiAlkaffNo ratings yet
- Concise Chronic Spinal Cord Injury GuidelinesDocument15 pagesConcise Chronic Spinal Cord Injury Guidelinesantonia buzilaNo ratings yet
- Can Physiotherapists Contribute To Care in The Emergency Department?Document3 pagesCan Physiotherapists Contribute To Care in The Emergency Department?J Roberto Meza OntiverosNo ratings yet
- Bateman 2019Document7 pagesBateman 2019physiodeepeshNo ratings yet
- Japanese Clinical Practice Guidelines For Rehabilitation in Critically Ill Patients 2023 (J-Recip 2023)Document23 pagesJapanese Clinical Practice Guidelines For Rehabilitation in Critically Ill Patients 2023 (J-Recip 2023)Rodrigo VelezNo ratings yet
- Multidisciplinary Exercise Based Oncology Rehabilitation Prog - 2021 - JournalDocument15 pagesMultidisciplinary Exercise Based Oncology Rehabilitation Prog - 2021 - JournalAbner HenriqueNo ratings yet
- 02 Reference For ElevationDocument8 pages02 Reference For ElevationFederico BristotNo ratings yet
- Descargar PDFDocument4 pagesDescargar PDFedraljNo ratings yet
- Mobilizatin MMDocument31 pagesMobilizatin MMAna Luiza ToldoNo ratings yet
- Lit Review of Nursing RoleDocument11 pagesLit Review of Nursing RoleSnowyNo ratings yet
- Imun 8Document14 pagesImun 8Helmi AdisafitriNo ratings yet
- International Journal of Gerontology: Original ArticleDocument5 pagesInternational Journal of Gerontology: Original ArticleTika MahelsaNo ratings yet
- Clinical Practice Guideline For Physical Therapist Management of People With Rheumatoid ArthritisDocument16 pagesClinical Practice Guideline For Physical Therapist Management of People With Rheumatoid Arthritis1541920001 LUIS GUILLERMO PAJARO FRANCO ESTUDIANTE ACTIVO ESPECIALIDAD MEDICINA INTERNANo ratings yet
- Spinal Cord Injury RehabilitationDocument9 pagesSpinal Cord Injury RehabilitationVaibhav BhatiaNo ratings yet
- PublishedversionDocument7 pagesPublishedversionAsvino SheejNo ratings yet
- Musculoskeletal Care - 2024 - Powell - Is Exercise Therapy The Right Treatment For Rotator Cuff Related Shoulder PainDocument12 pagesMusculoskeletal Care - 2024 - Powell - Is Exercise Therapy The Right Treatment For Rotator Cuff Related Shoulder PainxurraNo ratings yet
- Pzaa 180Document10 pagesPzaa 180Ajeeta KulkarniNo ratings yet
- Current Practice in The Rehabilitation of Complex Regional Pain Syndrome A Survey of PractitionersDocument8 pagesCurrent Practice in The Rehabilitation of Complex Regional Pain Syndrome A Survey of Practitionersgeschrich7No ratings yet
- Cardiac Rehabilitation Adherence: A Multifaceted ApproachDocument13 pagesCardiac Rehabilitation Adherence: A Multifaceted ApproachBOHR International Journal of Research on Cardiology and Cardiovascular DiseasesNo ratings yet
- Nutritional ManagmentDocument19 pagesNutritional ManagmentgianellaNo ratings yet
- A Systematic Review Protocol On The Effectiveness of Therapeutic Exercises Utilised by Physiotherapists To Improve Function in Patients With BurnsDocument7 pagesA Systematic Review Protocol On The Effectiveness of Therapeutic Exercises Utilised by Physiotherapists To Improve Function in Patients With BurnsSintia DeviNo ratings yet
- PIIS1440244018312702Document25 pagesPIIS1440244018312702Jesus Maturana YañezNo ratings yet
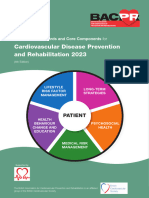
- BACPR Standards and Core Components 2023Document31 pagesBACPR Standards and Core Components 2023ganesh goreNo ratings yet
- Medi 100 00000Document7 pagesMedi 100 00000Dewi PutriNo ratings yet
- Cancers 14 05402 v2 PDFDocument43 pagesCancers 14 05402 v2 PDFPaulina Sobarzo VegaNo ratings yet
- ESPENpracticalpartiallyrevisedguideline Clinicalnutritionin ICUDocument20 pagesESPENpracticalpartiallyrevisedguideline Clinicalnutritionin ICUDANIELA MARTINEZ MELLADONo ratings yet
- Stem Cell Regenerative Medicine Scrma New Hope in Orthopedicsreview ArticleDocument6 pagesStem Cell Regenerative Medicine Scrma New Hope in Orthopedicsreview ArticleAtul DwivediNo ratings yet
- Role of Continuous Passive Motion of Elbow To Improve Feeding in Stroke A Comparative StudyDocument5 pagesRole of Continuous Passive Motion of Elbow To Improve Feeding in Stroke A Comparative StudyResearch ParkNo ratings yet
- Exercise and Diet For HFDocument8 pagesExercise and Diet For HFRobby Paguh TariganNo ratings yet
- Setting The Scene For The Second Stroke Recovery and Rehabilitation RoundtableDocument8 pagesSetting The Scene For The Second Stroke Recovery and Rehabilitation RoundtableMartín Rodrigo Lovera QuisbertNo ratings yet
- Fellowship in Sports RehabilitationDocument6 pagesFellowship in Sports Rehabilitationsendilcoumarv83No ratings yet
- Oswestry Low Back Disability QuestionnaireDocument3 pagesOswestry Low Back Disability QuestionnairechocklutdluxNo ratings yet
- Bernhardt 2019 - Setting The Scene For The Second Stroke Recovery and Rehabilitation RoundtableDocument7 pagesBernhardt 2019 - Setting The Scene For The Second Stroke Recovery and Rehabilitation RoundtableReagir ReagirNo ratings yet
- To Explore The Effect of Exergames For Increasing The Ranges of The Shoulder Joint in Incomplete Spinal Cord Injury Patients: A Case StudyDocument5 pagesTo Explore The Effect of Exergames For Increasing The Ranges of The Shoulder Joint in Incomplete Spinal Cord Injury Patients: A Case StudyIJAR JOURNALNo ratings yet
- Coronado-Zarco Et Al., 2019 PDFDocument9 pagesCoronado-Zarco Et Al., 2019 PDFadi pranotoNo ratings yet
- Physical Exercise Intervention For Children UndergDocument18 pagesPhysical Exercise Intervention For Children UndergIra AhrianaNo ratings yet
- Sundberg Et Al. BMC Musculoskeletal DisordersDocument10 pagesSundberg Et Al. BMC Musculoskeletal DisordersCrainlyNo ratings yet
- The Role of Physician Associate in Primary Care in England 1556Document15 pagesThe Role of Physician Associate in Primary Care in England 1556R. WadlowNo ratings yet
- Rehabilitación CardiacaDocument17 pagesRehabilitación Cardiacamsq.cv5919No ratings yet
- FIX JurnalDocument9 pagesFIX JurnalFitria Marina SandyNo ratings yet
- Eiu Health System Preparedness FinalDocument63 pagesEiu Health System Preparedness FinalFamilia En AcNo ratings yet
- Cost-Effectiveness of Individualized Nutrition and Exercise Therapy For Rehabilitation Following Hip FractureDocument8 pagesCost-Effectiveness of Individualized Nutrition and Exercise Therapy For Rehabilitation Following Hip FracturebellaNo ratings yet
- Ped 2Document48 pagesPed 2ericaluiza.henriques2002No ratings yet
- Experts Advise Against Arthroscopy For Almost All Patients With Degenerative Knee Damage - FullDocument9 pagesExperts Advise Against Arthroscopy For Almost All Patients With Degenerative Knee Damage - FullWillbourNo ratings yet
- Education, Self-Management, and Upper Extremity Exercise Training in People With Rheumatoid Arthritis: A Randomized Controlled TrialDocument11 pagesEducation, Self-Management, and Upper Extremity Exercise Training in People With Rheumatoid Arthritis: A Randomized Controlled TrialAnonymous vUl83IptiSNo ratings yet
- Exploring Patient Attitudes To Behaviour Change Beforesurgery To Reduce Peri-Operative RiskDocument9 pagesExploring Patient Attitudes To Behaviour Change Beforesurgery To Reduce Peri-Operative RiskFlavia VitalNo ratings yet
- Health Services and Delivery ResearchDocument152 pagesHealth Services and Delivery ResearchThierry UhawenimanaNo ratings yet
- Journal of Exercise Science & Fitness: Shi Zhou, Kade Davison, Fei Qin, Kuei-Fu Lin, Bik-Chu Chow, Jie-Xiu ZhaoDocument10 pagesJournal of Exercise Science & Fitness: Shi Zhou, Kade Davison, Fei Qin, Kuei-Fu Lin, Bik-Chu Chow, Jie-Xiu Zhaoapi-583367679No ratings yet
- Sensors 22 08069Document15 pagesSensors 22 08069Farhat SultanNo ratings yet
- Optimizing The Application of Surgery For Degenerative Cervical Myelopathy (AO Spine RECODE-DCM Research Priority Number 10)Document12 pagesOptimizing The Application of Surgery For Degenerative Cervical Myelopathy (AO Spine RECODE-DCM Research Priority Number 10)Dr Juan Carlos Ordóñez LegardaNo ratings yet
- Regenerative Injections in Sports Medicine: An Evidenced Based ApproachFrom EverandRegenerative Injections in Sports Medicine: An Evidenced Based ApproachNo ratings yet
- 1 s2.0 S0940960213000241 MainDocument7 pages1 s2.0 S0940960213000241 MainSgantzos MarkosNo ratings yet
- J S T A I (A) : Oint and Oft Issue Spiration and Njection RthrocentesisDocument19 pagesJ S T A I (A) : Oint and Oft Issue Spiration and Njection RthrocentesisSgantzos MarkosNo ratings yet
- Cupuncture: Victor S. SierpinaDocument6 pagesCupuncture: Victor S. SierpinaSgantzos MarkosNo ratings yet
- Case Series in Lifestyle Medicine: A Team Approach To Behavior ChangesDocument10 pagesCase Series in Lifestyle Medicine: A Team Approach To Behavior ChangesSgantzos MarkosNo ratings yet
- Femoral Neck FracturesDocument58 pagesFemoral Neck FracturesDibyendunarayan Bid100% (1)
- Muthu HT ReportDocument87 pagesMuthu HT ReportSridharan DNo ratings yet
- 1st Floor No 105 Above Raymonds Opp Medical College Koti: SHARMA Bpo SupportDocument4 pages1st Floor No 105 Above Raymonds Opp Medical College Koti: SHARMA Bpo SupportMK Musthafa GudalurNo ratings yet
- Writing Task 1 and 2Document4 pagesWriting Task 1 and 2Rumana Ali75% (4)
- Clinical Practice Guidelines: Chronic Suppurative Otitis Media in AdultsDocument28 pagesClinical Practice Guidelines: Chronic Suppurative Otitis Media in Adultsnanu-jenuNo ratings yet
- Cerebral Palsy AnatomyDocument5 pagesCerebral Palsy AnatomyIoana irimiaNo ratings yet
- Wrights Stain Diff Quick Manual MethDocument7 pagesWrights Stain Diff Quick Manual MethJose CisnerosNo ratings yet
- Es HG 2014 AbstractsDocument581 pagesEs HG 2014 Abstractsgengen100% (1)
- Abdomen Exam DetailsDocument5 pagesAbdomen Exam Detailsdidutza91No ratings yet
- Induction of Labour For Post MaturityDocument6 pagesInduction of Labour For Post MaturityYwagar YwagarNo ratings yet
- Exercise Prescription For Health & Fittness For Patients With ObesityDocument1 pageExercise Prescription For Health & Fittness For Patients With ObesityWasemBhatNo ratings yet
- Complete Denture Copy Technique-A Practical ApplicationDocument6 pagesComplete Denture Copy Technique-A Practical ApplicationDiana Ecaterina NechiforNo ratings yet
- Mock CodeDocument4 pagesMock CodeKrezielDulosEscobarNo ratings yet
- Clinmed 19 3 261bDocument2 pagesClinmed 19 3 261bgevowo3277No ratings yet
- BSA Creat Clearance Calculation OriginalDocument2 pagesBSA Creat Clearance Calculation Originalstrider_sdNo ratings yet
- Epilepsy in PregnancyDocument33 pagesEpilepsy in PregnancyxxdrivexxNo ratings yet
- Name: NIM: Class:: Medical InstrumentsDocument9 pagesName: NIM: Class:: Medical InstrumentsNessyaa SyahnaNo ratings yet
- 5-Minute Pediatric Consult, The: Make The Most Effective Diagnostic and Therapeutic Decisions Quickly and Efficiently!Document2 pages5-Minute Pediatric Consult, The: Make The Most Effective Diagnostic and Therapeutic Decisions Quickly and Efficiently!Antonio D'CostaNo ratings yet
- Daftar PustakaDocument5 pagesDaftar PustakaRizky Rachmat KurniawanNo ratings yet
- On SSTDocument14 pagesOn SSTsureesicNo ratings yet
- Paediatric Handbook - Amanda GweeDocument5 pagesPaediatric Handbook - Amanda GweezekijuraNo ratings yet
- April 24: Zein Mahgoub PACES Simplified Zein MahgoubDocument4 pagesApril 24: Zein Mahgoub PACES Simplified Zein Mahgoubmalik003No ratings yet
- Depression in Young People and The ElderlyDocument28 pagesDepression in Young People and The ElderlyJennyMae Ladica QueruelaNo ratings yet
- Peritoneal DialysisDocument37 pagesPeritoneal DialysisEm CastilloNo ratings yet
- Implant OcclusionDocument43 pagesImplant OcclusionMuaiyed Buzayan Akremy100% (3)
- Bemonc ChecklistDocument2 pagesBemonc Checklistkengyakkersss100% (1)
- Pa Tas Database (Conso)Document30 pagesPa Tas Database (Conso)AlbeldaArnaldoNo ratings yet
- 0medical Jurisprudence Summary Compilation PDFDocument85 pages0medical Jurisprudence Summary Compilation PDFFloyd balansagNo ratings yet