Download as pdf or txt
You might also like
- Physical Assessment PneumoniaDocument4 pagesPhysical Assessment PneumoniaMajkel Benche Custodio0% (1)
- Textbook of GB Madhuri For Cardio-Respiratory Cardiac Surgery and Thoracic Surgery ConditionsDocument340 pagesTextbook of GB Madhuri For Cardio-Respiratory Cardiac Surgery and Thoracic Surgery ConditionsBpt4 Kims100% (1)
- Medpox RecallsDocument8 pagesMedpox RecallsmedpoxNo ratings yet
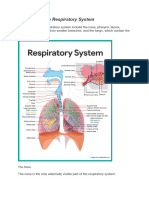
- Respiratory System (Anatomy)Document54 pagesRespiratory System (Anatomy)Juliet Ileto Villaruel - AlmonacidNo ratings yet
- Functions of The Respiratory SystemDocument10 pagesFunctions of The Respiratory SystemKrisha AvorqueNo ratings yet
- SEHH2234 2021 S2 Ch14 RespirationDocument56 pagesSEHH2234 2021 S2 Ch14 Respirationmiki leeNo ratings yet
- Respiratory SystemDocument8 pagesRespiratory SystemYoudonumeNo ratings yet
- Noor Respiratory 6Document43 pagesNoor Respiratory 6Hond HayNo ratings yet
- B5M2C1 REVIEWERDocument31 pagesB5M2C1 REVIEWERMariel AbatayoNo ratings yet
- Respiratory System PDFDocument16 pagesRespiratory System PDFMary Ann SacramentoNo ratings yet
- Assessment of Respiratory System: Submitted by Pankaj Singh Rana Nurse Practitioner in Critical Care, SrhuDocument80 pagesAssessment of Respiratory System: Submitted by Pankaj Singh Rana Nurse Practitioner in Critical Care, SrhuMary Christine Estrada CabactulanNo ratings yet
- Noor RespiratoryDocument45 pagesNoor RespiratoryHond HayNo ratings yet
- NCM 1234 - Thorax and LungsDocument150 pagesNCM 1234 - Thorax and LungsXerxes DejitoNo ratings yet
- Respiratory SystemDocument42 pagesRespiratory SystemSohailriazNo ratings yet
- Anatomi Pertemuan 4Document52 pagesAnatomi Pertemuan 4dimasNo ratings yet
- Anatomy and Physiology Chapter 8 Respiratory System PDFDocument58 pagesAnatomy and Physiology Chapter 8 Respiratory System PDFJobelleNerpiolAbaoNo ratings yet
- Respiratory SystemDocument61 pagesRespiratory SystemDenise Nicole PinedaNo ratings yet
- RTS1-K13-Anatomy of LungsDocument22 pagesRTS1-K13-Anatomy of LungsYohanna SinuhajiNo ratings yet
- Anatomy of LungsDocument22 pagesAnatomy of Lungsnadya0% (1)
- The Respiratory System: Raymund Christopher R. Dela Peña, RN, RM, MAN Clinical Faculty UNP-College of NursingDocument95 pagesThe Respiratory System: Raymund Christopher R. Dela Peña, RN, RM, MAN Clinical Faculty UNP-College of NursingrnrmmanphdNo ratings yet
- Respiratory System Anatomy, Assessment & Diagnostic TestsDocument24 pagesRespiratory System Anatomy, Assessment & Diagnostic TestsPrince Rener Velasco PeraNo ratings yet
- Kuliah 3 Respirasi + CardiovasculerDocument73 pagesKuliah 3 Respirasi + CardiovasculerNindya Alfa DichaNo ratings yet
- PAin and Oxygenation HandoutsPRELIMSDocument7 pagesPAin and Oxygenation HandoutsPRELIMSJhoanna de ChavezNo ratings yet
- Lec 4-The Respiratory System Biology Batch 6Document34 pagesLec 4-The Respiratory System Biology Batch 6Howra KiyasdeenNo ratings yet
- Chest and Lungs ExaminationDocument75 pagesChest and Lungs Examinationdhainey100% (10)
- Cardio Pulmonary LectureDocument55 pagesCardio Pulmonary Lectureahmedmohcen442No ratings yet
- Respiratory SystemDocument5 pagesRespiratory SystemJay QuilnetNo ratings yet
- Respi Anaphy Day 1Document128 pagesRespi Anaphy Day 1Tracy Megan RusillonNo ratings yet
- Anatomy of The Respiratory SystemDocument8 pagesAnatomy of The Respiratory Systemsuharti2365No ratings yet
- Approach To The Patient With Respiratory DiseaseDocument6 pagesApproach To The Patient With Respiratory DiseaseRem AlfelorNo ratings yet
- Trachea Presentation 1Document50 pagesTrachea Presentation 151-JASASWINI NAYAKNo ratings yet
- I. Review of Respiratory System A.ppt 2Document115 pagesI. Review of Respiratory System A.ppt 2arielleortuosteNo ratings yet
- Anatomy & PhysiologyDocument42 pagesAnatomy & PhysiologyArah Lyn ApiagNo ratings yet
- The Respiratory System or Pulmonary SystemDocument53 pagesThe Respiratory System or Pulmonary Systemfharidaismail47No ratings yet
- Respiratory LectureDocument17 pagesRespiratory Lecturemichellechapman0804No ratings yet
- Pulmo Management Week 1Document160 pagesPulmo Management Week 1Dharlyn MungcalNo ratings yet
- 24 - Respiratory SystemDocument18 pages24 - Respiratory SystemHarshil PatelNo ratings yet
- Dr. Sachin Kapur M.Phil, PHD: 20+ Years Teaching ExperienceDocument44 pagesDr. Sachin Kapur M.Phil, PHD: 20+ Years Teaching ExperienceVikas KumarNo ratings yet
- Respiratory GeriatricsDocument17 pagesRespiratory GeriatricsArvinjohn GacutanNo ratings yet
- Bio1 Respiratory System 1Document41 pagesBio1 Respiratory System 1Camela Kim Domider TenorioNo ratings yet
- Physio 1Document17 pagesPhysio 1NeviNo ratings yet
- Anatomy and Physiology of The Respiratory TractDocument49 pagesAnatomy and Physiology of The Respiratory TractshvnagaNo ratings yet
- Physical Examination in Respiratory SystemDocument84 pagesPhysical Examination in Respiratory SystemDr-i BarreNo ratings yet
- 4 RSDocument16 pages4 RSzabdullahstud1No ratings yet
- Respiratory SystemDocument33 pagesRespiratory SystemMusadiq Khan DurraniNo ratings yet
- Broncho PneumoniaDocument46 pagesBroncho PneumoniaAfrianzah Sevenfoldism100% (1)
- Respiratory SystemDocument8 pagesRespiratory SystemKhushi JainNo ratings yet
- Assessment of Patients With Respiratory Disorders Basic Respiratory Care ModalitiesDocument15 pagesAssessment of Patients With Respiratory Disorders Basic Respiratory Care ModalitiesJhosita Flora LarocoNo ratings yet
- 01 Respiratory SystemDocument15 pages01 Respiratory Systemnaseer alfahdNo ratings yet
- ANATOMYDocument53 pagesANATOMYJocel Mae OrtegaNo ratings yet
- Respiratory System Physiology.Document21 pagesRespiratory System Physiology.sandhiya.peetamberNo ratings yet
- CP4. Respiratory SystemDocument28 pagesCP4. Respiratory Systemdafabc50No ratings yet
- Group1 Review of Respiratory SystemDocument41 pagesGroup1 Review of Respiratory Systemjohn obinaNo ratings yet
- NCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsDocument7 pagesNCM 112 LEC Topic 2 Oxygenation Current Health History Physical Examination Normal Abnormal Breath Sounds Breathing PatternsViviene Faye FombuenaNo ratings yet
- Physiology of The Respiratory System-1Document155 pagesPhysiology of The Respiratory System-1Adil MusaddiqNo ratings yet
- 01 Respiratory SystemDocument43 pages01 Respiratory Systemhafaisolo37No ratings yet
- Assignment On Chest PhysiotherapyDocument15 pagesAssignment On Chest PhysiotherapyAxsa AlexNo ratings yet
- 22 Respiratory SystemDocument99 pages22 Respiratory SystemvanderphysNo ratings yet
- RespiratoryDocument62 pagesRespiratoryDerón Asbery HolmesNo ratings yet
- Respiratory SystemDocument71 pagesRespiratory SystemmarygracetamborlnhsNo ratings yet
- Respiratory SystemDocument12 pagesRespiratory Systemab4943409No ratings yet
- Breathe In, Breathe Out: Learning About Your LungsFrom EverandBreathe In, Breathe Out: Learning About Your LungsRating: 3.5 out of 5 stars3.5/5 (3)
- A Simple Guide to the Nose and Its Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to the Nose and Its Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- The Triple B: Breath andDocument12 pagesThe Triple B: Breath andChristian FarofaldaneNo ratings yet
- Group 4 - Nicu Case StudyDocument20 pagesGroup 4 - Nicu Case StudyMagdaraog Gabrielle A.No ratings yet
- Krok 1 Anatomy 6Document1 pageKrok 1 Anatomy 6Sandeep KumarNo ratings yet
- Question Bank Class Vii (Science) Chapter-1 Nutrition in PlantsDocument34 pagesQuestion Bank Class Vii (Science) Chapter-1 Nutrition in Plantssivsyadav50% (2)
- HSNS264 A1 COPDDocument2 pagesHSNS264 A1 COPDKC Nilam100% (1)
- Chest X-Ray Interpretation (Not Just Black and White) PDFDocument8 pagesChest X-Ray Interpretation (Not Just Black and White) PDFVincent WesleyNo ratings yet
- CASE-PRESENTATION-Bronchopulmonary DysplasiaDocument112 pagesCASE-PRESENTATION-Bronchopulmonary DysplasiaLouie MansaNo ratings yet
- 1.basic Final McqsDocument78 pages1.basic Final McqsPrabhat KcNo ratings yet
- 4th Q Module GEN BIO 2 Week 5 6Document19 pages4th Q Module GEN BIO 2 Week 5 6Hannah CastroNo ratings yet
- Human Respiratory System FunctionsDocument2 pagesHuman Respiratory System Functionsapi-169639475No ratings yet
- Sputum CollectionDocument14 pagesSputum CollectionAira AlaroNo ratings yet
- EmbryologyDocument29 pagesEmbryologySara Gblabi50% (2)
- Thoracic Cavity (Chapter 3)Document13 pagesThoracic Cavity (Chapter 3)Alenna BenitezNo ratings yet
- Anatomy MCQDocument9 pagesAnatomy MCQMido TooNo ratings yet
- ASDA Packet I-I (Part 1) PDFDocument46 pagesASDA Packet I-I (Part 1) PDFAbhi ThakkarNo ratings yet
- Feline Brochial DiseaseDocument7 pagesFeline Brochial DiseaseDimas SetiawanNo ratings yet
- C1 Respiratory System WorksheetDocument5 pagesC1 Respiratory System Worksheetlccjane8504No ratings yet
- ch19 Studyoutline Respiratory-SystemDocument16 pagesch19 Studyoutline Respiratory-SystemElvin MoletaNo ratings yet
- Anatomy and Physiology of Respiratory System Relevant To AnaesthesiaDocument10 pagesAnatomy and Physiology of Respiratory System Relevant To AnaesthesiaAnonymous h0DxuJTNo ratings yet
- Bot Med Final CHARTDocument33 pagesBot Med Final CHARTapi-26938624100% (3)
- Respiratory System: StructureDocument29 pagesRespiratory System: StructureDr. Abir Ishtiaq100% (1)
- Case Presentation in Geriatric Ward "Cancer of The Larynx"Document130 pagesCase Presentation in Geriatric Ward "Cancer of The Larynx"Christina GutierrezNo ratings yet
- Respiratory System: A) The Conducting Portion, Which Consists of The Nasal CavitiesDocument7 pagesRespiratory System: A) The Conducting Portion, Which Consists of The Nasal CavitiesSalmah Alimah FitriNo ratings yet
- An Update On Tracheal and Airway - 2020 - Veterinary Clinics of North AmericaDocument12 pagesAn Update On Tracheal and Airway - 2020 - Veterinary Clinics of North AmericaMariale OrdóñezNo ratings yet
- Science 9Document13 pagesScience 9Jho R NelNo ratings yet
- Grossing Templates (S)Document51 pagesGrossing Templates (S)Jack GuccioneNo ratings yet
- Tuberculosis and Lung Damage: From Epidemiology To PathophysiologyDocument20 pagesTuberculosis and Lung Damage: From Epidemiology To PathophysiologyDyan TonyNo ratings yet