Download as pdf or txt
You might also like
- 2010 Short-Duration Massage at The Hamstrings Musculotendinous Junction Induces Greater Range of MotionDocument8 pages2010 Short-Duration Massage at The Hamstrings Musculotendinous Junction Induces Greater Range of MotionFrancisco Antonó Castro WeithNo ratings yet
- Visual Mnemonics For Biochemistry PDFDocument162 pagesVisual Mnemonics For Biochemistry PDFMahin Rahman100% (2)
- Vitro MPC Pro-Liferation and DifferentiationDocument14 pagesVitro MPC Pro-Liferation and DifferentiationNev NnNo ratings yet
- Scapular Muscle Rehabilitation Exercises in Overhead Athletes With Impingement SymptomsDocument10 pagesScapular Muscle Rehabilitation Exercises in Overhead Athletes With Impingement SymptomsTheologos PardalidisNo ratings yet
- Therapeutic Effects of Massage and Electrotherapy On Muscle Tone, Stiffness and Muscle Contraction Following Gastrocnemius Muscle FatigueDocument4 pagesTherapeutic Effects of Massage and Electrotherapy On Muscle Tone, Stiffness and Muscle Contraction Following Gastrocnemius Muscle FatigueAina SarahNo ratings yet
- Dosagem Otima Musculo PDFDocument10 pagesDosagem Otima Musculo PDFJanaina PanizzaNo ratings yet
- Research ArticleDocument9 pagesResearch ArticleLISTIA NURBAETINo ratings yet
- The Impact of Whole Body Vibration Therapy On Spasticity and Disability of The Patients With Poststroke HemiplegiaDocument6 pagesThe Impact of Whole Body Vibration Therapy On Spasticity and Disability of The Patients With Poststroke HemiplegialabsoneducationNo ratings yet
- The Effect of Vibration Training On Delayed Muscle.33Document10 pagesThe Effect of Vibration Training On Delayed Muscle.33Alvaro RodriguezNo ratings yet
- Populasi 12Document4 pagesPopulasi 12Resky Ika Sah PutriNo ratings yet
- Buttner - JAP 07 - MicroarrayDocument12 pagesButtner - JAP 07 - Microarrayf1r3br4nd9427No ratings yet
- Pagé-Descarreaux2019 Article EffectsOfSpinalMDocument14 pagesPagé-Descarreaux2019 Article EffectsOfSpinalMdavid ioanaNo ratings yet
- Ansiedade e Treino Combinado PDFDocument8 pagesAnsiedade e Treino Combinado PDFPaulo AfonsoNo ratings yet
- Fatigue in Athlets Mox + Cupping PDFDocument6 pagesFatigue in Athlets Mox + Cupping PDFmedicina tradicionalNo ratings yet
- Effects of Massage On Delayed-Onset Muscle Soreness, Swelling, and Recovery of Muscle FunctionDocument7 pagesEffects of Massage On Delayed-Onset Muscle Soreness, Swelling, and Recovery of Muscle FunctionjaviNo ratings yet
- Effects of Kinesiotherapy, Ultrasound and Electrotherapy in Management of Bilateral Knee Osteoarthritis: Prospective Clinical TrialDocument10 pagesEffects of Kinesiotherapy, Ultrasound and Electrotherapy in Management of Bilateral Knee Osteoarthritis: Prospective Clinical TrialDavid Alejandro Cavieres AcuñaNo ratings yet
- Maat 08 I 3 P 234Document3 pagesMaat 08 I 3 P 234Felipe Andrés CabezasNo ratings yet
- Crioterapia Post EjercicioDocument22 pagesCrioterapia Post EjercicioRamsses Rubio SalasNo ratings yet
- Effects of Acute Endurance Exercise at 65 and 85 oDocument3 pagesEffects of Acute Endurance Exercise at 65 and 85 oaede747No ratings yet
- BR J Sports Med 1994 Smith 267 71Document6 pagesBR J Sports Med 1994 Smith 267 71Ricardo Pereira NevesNo ratings yet
- The Impact of Metabolic Stress On Hormonal Responses and Muscular AdaptationsDocument10 pagesThe Impact of Metabolic Stress On Hormonal Responses and Muscular AdaptationsJoão NunesNo ratings yet
- 7 Heggelund2012Document7 pages7 Heggelund2012Sergio Machado NeurocientistaNo ratings yet
- Efectos Del Ejercicio en Pacientes Mayores Con Diabetes ECADocument13 pagesEfectos Del Ejercicio en Pacientes Mayores Con Diabetes ECAAndrés Araneda VásquezNo ratings yet
- Stretching: Mechanisms and Benefits For Sport Performance and Injury PreventionDocument19 pagesStretching: Mechanisms and Benefits For Sport Performance and Injury PreventionGeorge M. PamborisNo ratings yet
- Effect of Manual Lymph Drainage On Removal of Blood Lactate After Submaximal ExerciseDocument5 pagesEffect of Manual Lymph Drainage On Removal of Blood Lactate After Submaximal ExerciseRatna Sulistya DewiNo ratings yet
- Effect of Task-Oriented Training and Neurodevelopmental Treatment On The Sitting Posture in Children With Cerebral PalsyDocument3 pagesEffect of Task-Oriented Training and Neurodevelopmental Treatment On The Sitting Posture in Children With Cerebral PalsyPhysio SauravNo ratings yet
- Brain Sciences: Exercise Strengthens Central Nervous System Modulation of Pain in FibromyalgiaDocument13 pagesBrain Sciences: Exercise Strengthens Central Nervous System Modulation of Pain in FibromyalgiaJavier Alejandro Rodriguez MelgozaNo ratings yet
- CipryanDocument10 pagesCipryan197Anzali CahyatiNo ratings yet
- Effects of Stretching On Passive Muscle Tension and Response To Eccentric ExerciseDocument8 pagesEffects of Stretching On Passive Muscle Tension and Response To Eccentric ExerciseRuben CapelaNo ratings yet
- The Effects of A Sensorimotor Training and A Strength Training On Postural Stabilisation, Maximum Isometric Contraction and Jump PerformanceDocument5 pagesThe Effects of A Sensorimotor Training and A Strength Training On Postural Stabilisation, Maximum Isometric Contraction and Jump PerformanceDiego LacerdaNo ratings yet
- Crystal 2013Document10 pagesCrystal 2013Jairo EspinosaNo ratings yet
- Chronic Ankle InstabilityDocument9 pagesChronic Ankle InstabilityJonathan Elias Barrientos OssesNo ratings yet
- 1 s2.0 S0965229923000833 MainDocument11 pages1 s2.0 S0965229923000833 MaintheophileflorentinNo ratings yet
- Effects of Low-Intensity Resistance Exercise With Vascular Occlusion On Physical Function in Healthy Elderly People.-2Document7 pagesEffects of Low-Intensity Resistance Exercise With Vascular Occlusion On Physical Function in Healthy Elderly People.-2Ingrid Ramirez PNo ratings yet
- Thematic Poster Bioenergetics and Training: (No Relationships Reported)Document2 pagesThematic Poster Bioenergetics and Training: (No Relationships Reported)pantufoNo ratings yet
- Journal ComparedDocument4 pagesJournal ComparedRisalah Al KhaerNo ratings yet
- The Effects of Myofascial Release With Foam Rolling On Performance PDFDocument8 pagesThe Effects of Myofascial Release With Foam Rolling On Performance PDFhenriqueNo ratings yet
- Acute Effect of Different Orders of Concurrent Training On GlycemiaDocument8 pagesAcute Effect of Different Orders of Concurrent Training On GlycemiaAlexandre VizzoniNo ratings yet
- Heavens 2014Document9 pagesHeavens 2014alexandremagnopersonalNo ratings yet
- Continued Sports Activity, Using A Pain - Monitoring Model, During Rehabilitation in Patients With Achilles TendinopathyDocument10 pagesContinued Sports Activity, Using A Pain - Monitoring Model, During Rehabilitation in Patients With Achilles TendinopathyMichele MarengoNo ratings yet
- Chronic Static Stretching Improves Exercise PerformanceDocument7 pagesChronic Static Stretching Improves Exercise Performanceyadex60201No ratings yet
- Suraj KanaseDocument4 pagesSuraj KanaseSURAJNo ratings yet
- Bmri2022 4133883Document8 pagesBmri2022 4133883aaNo ratings yet
- Efficacy Laser FatigueDocument10 pagesEfficacy Laser FatigueIana RusuNo ratings yet
- DeloadDocument27 pagesDeloadtatiNo ratings yet
- Stretching: Mechanisms and Benefits For Sport Performance and Injury PreventionDocument18 pagesStretching: Mechanisms and Benefits For Sport Performance and Injury PreventionBruno HenriqueNo ratings yet
- Nat Sci 2018 16 (7) :1-6) - ISSN 1545-0740 (Print) ISSN 2375-7167 (Online)Document6 pagesNat Sci 2018 16 (7) :1-6) - ISSN 1545-0740 (Print) ISSN 2375-7167 (Online)rizk86No ratings yet
- Deep Massage TendinopathyDocument7 pagesDeep Massage Tendinopathysilvaines06No ratings yet
- The Effects of Proprioceptive or Strength Training On The Neuromuscular Function of The ACL Reconstructed Knee - A Randomized Clinical TrialDocument9 pagesThe Effects of Proprioceptive or Strength Training On The Neuromuscular Function of The ACL Reconstructed Knee - A Randomized Clinical Trialsabilillah putri63No ratings yet
- European J App Phys - Effectiveness of Using Wearable Vibration Therapy T PDFDocument9 pagesEuropean J App Phys - Effectiveness of Using Wearable Vibration Therapy T PDFFrancisco Javier Medina CaballeroNo ratings yet
- Qu Et Al (2020) - Cryotherapy Models and Timing Sequence Recovery of Exercise Induced Muscle Damage in Middle and Long Distance RunnersDocument7 pagesQu Et Al (2020) - Cryotherapy Models and Timing Sequence Recovery of Exercise Induced Muscle Damage in Middle and Long Distance RunnersNg Hui HwaNo ratings yet
- Single Set Vs Multiple Sets 2004Document6 pagesSingle Set Vs Multiple Sets 2004turbobrikNo ratings yet
- Effects of Low-Volume High-Intensity Interval Training (HIT) On Fitness in Adults: A Meta-Analysis of Controlled and Non-Controlled TrialsDocument13 pagesEffects of Low-Volume High-Intensity Interval Training (HIT) On Fitness in Adults: A Meta-Analysis of Controlled and Non-Controlled TrialsPaulo PiresNo ratings yet
- Laroche 2006Document8 pagesLaroche 2006Ronan Varela de MeloNo ratings yet
- Ogborn y Schoenfeld 2017Document25 pagesOgborn y Schoenfeld 2017Alejandro Albert RequesNo ratings yet
- Effect of Isometric Quadriceps Exercise On Muscle StrengthDocument7 pagesEffect of Isometric Quadriceps Exercise On Muscle StrengthAyu RoseNo ratings yet
- FatehDocument9 pagesFatehVIVEKNo ratings yet
- Supplementation With A Mango Leaf Extract (Zynamite®) in Combination With Quercetin Attenuates Muscle Damage and Pain and Accelerates Recovery After Strenuous Damaging ExerciseDocument15 pagesSupplementation With A Mango Leaf Extract (Zynamite®) in Combination With Quercetin Attenuates Muscle Damage and Pain and Accelerates Recovery After Strenuous Damaging ExerciseRodas 108No ratings yet
- Exc PDFDocument9 pagesExc PDFHELGA MARÍLIA DA SILVA RAFAEL HENRIQUESNo ratings yet
- Neuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodFrom EverandNeuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodNo ratings yet
- Manual of Vibration Exercise and Vibration TherapyFrom EverandManual of Vibration Exercise and Vibration TherapyJörn RittwegerNo ratings yet
- 6439 7667 1 PBDocument12 pages6439 7667 1 PBZulfikar YuchaNo ratings yet
- 562 FullDocument11 pages562 FullZulfikar YuchaNo ratings yet
- Meyer 2014Document7 pagesMeyer 2014Zulfikar YuchaNo ratings yet
- OptimDocument110 pagesOptimZulfikar YuchaNo ratings yet
- 6566-Article Text-68051-2-10-20230818Document6 pages6566-Article Text-68051-2-10-20230818Zulfikar YuchaNo ratings yet
- ELS 22 Maret 2023Document16 pagesELS 22 Maret 2023Zulfikar YuchaNo ratings yet
- Tivoli: Golf With Class: D. North of The Santo MountainsDocument8 pagesTivoli: Golf With Class: D. North of The Santo MountainsZulfikar YuchaNo ratings yet
- Systemic Inflammatory Response SyndromeDocument28 pagesSystemic Inflammatory Response SyndromeRainickBrenhizarNavarro100% (1)
- FWA Prepayment Review Records Request: InstructionsDocument7 pagesFWA Prepayment Review Records Request: Instructionsabdulla.mho23No ratings yet
- Cerri Et Al. 2017Document7 pagesCerri Et Al. 2017JD SánchezNo ratings yet
- SSC - 2020-06-15 - THE VISION OF VILAZODONE AND VORTIOXETINE - CommentDocument27 pagesSSC - 2020-06-15 - THE VISION OF VILAZODONE AND VORTIOXETINE - CommentKaroline MarxNo ratings yet
- Emotions and Body ChemicalsDocument24 pagesEmotions and Body ChemicalsSiddharth chandan dasNo ratings yet
- 17 A1 ExcitotoxinsDocument41 pages17 A1 ExcitotoxinsholandecNo ratings yet
- Pharmacology NotesDocument9 pagesPharmacology NotesMayya FirdousNo ratings yet
- Molecular Pathophysiology of Congenital Long QT SyndromeDocument46 pagesMolecular Pathophysiology of Congenital Long QT SyndromeRareș MănucăNo ratings yet
- Cathecolamine, Sympathomimetic DrugsDocument24 pagesCathecolamine, Sympathomimetic DrugsEric AryantoNo ratings yet
- Opioid Analgesics & AntagonistsDocument13 pagesOpioid Analgesics & AntagonistsafiniherlyanaNo ratings yet
- CINVDocument23 pagesCINVHesham IbrahimNo ratings yet
- Chapter Sixteen Cell SignalingDocument96 pagesChapter Sixteen Cell SignalingRu LiliNo ratings yet
- Antidepressants and AntipsychoticsDocument8 pagesAntidepressants and AntipsychoticsWillNo ratings yet
- Activity in EAPP ObesityDocument1 pageActivity in EAPP ObesityIrrol RosNo ratings yet
- Organismal Physiology PDQ 3 - Cellular Communication Video Notes Part 3Document3 pagesOrganismal Physiology PDQ 3 - Cellular Communication Video Notes Part 3Sylvia Grace0% (1)
- Apoptosis: Proliferation, Differentiation and Apoptosis Are Crucial To DevelopmentDocument21 pagesApoptosis: Proliferation, Differentiation and Apoptosis Are Crucial To DevelopmentInsyirah JohariNo ratings yet
- 01 GRAT - ANS PharmDocument4 pages01 GRAT - ANS PharmjuanNo ratings yet
- Subject Forensic ScienceDocument12 pagesSubject Forensic SciencepartikNo ratings yet
- Biology - May 2017Document1 pageBiology - May 2017Rahique ShuaibNo ratings yet
- MCQ Sympatholytics 1Document8 pagesMCQ Sympatholytics 1Hossam MohamedNo ratings yet
- St. Paul University Philippines: /almarallag/v01/2020-21Document3 pagesSt. Paul University Philippines: /almarallag/v01/2020-21Suzete PagaduanNo ratings yet
- DR: Samah Gaafar Al-ShaygiDocument22 pagesDR: Samah Gaafar Al-Shaygiكسلان اكتب اسميNo ratings yet
- PDF Clinical Neuroendocrinology An Introduction Michael Wilkinson Ebook Full ChapterDocument53 pagesPDF Clinical Neuroendocrinology An Introduction Michael Wilkinson Ebook Full Chapternolan.gold619100% (3)
- Bio 473 Cardiac Activity Lab ReportDocument4 pagesBio 473 Cardiac Activity Lab Reportapi-253602935No ratings yet
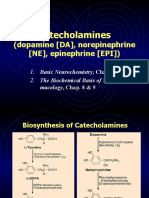
- Catecholamines: (Dopamine (DA), Norepinephrine (NE), Epinephrine (EPI) )Document30 pagesCatecholamines: (Dopamine (DA), Norepinephrine (NE), Epinephrine (EPI) )Imrana AamirNo ratings yet
- NSTP Drug and Substance AbuseDocument3 pagesNSTP Drug and Substance AbusemrwhoNo ratings yet
- NeurotransmittersDocument92 pagesNeurotransmittersClare DucutNo ratings yet
- General Pharmacology MCQ: 1. The Science Which Deals With The Drug and Their Action On Human Body Is CalledDocument274 pagesGeneral Pharmacology MCQ: 1. The Science Which Deals With The Drug and Their Action On Human Body Is CalledAmritesh singh thakurNo ratings yet
- DopamineDocument28 pagesDopamineNTA UGC-NETNo ratings yet