
s1013 70252970039 9
s1013 70252970039 9
You might also like
- Margaret McWilliams-Fundamentals of Meal ManagementDocument361 pagesMargaret McWilliams-Fundamentals of Meal ManagementSaher Yasin89% (9)
- Floor Cleaner Sunlight - NC Lau Sàn SunlightDocument3 pagesFloor Cleaner Sunlight - NC Lau Sàn Sunlightnhật minh nguyễnNo ratings yet
- Physiotherapy and Airway Clearance Techniques and Devices: Maggie McilwaineDocument3 pagesPhysiotherapy and Airway Clearance Techniques and Devices: Maggie Mcilwaineحسام الوجيهNo ratings yet
- Crit Care Med.: Krause@kkl200.ukl - Uni-Freiburg - de Back To TopDocument11 pagesCrit Care Med.: Krause@kkl200.ukl - Uni-Freiburg - de Back To TopTharshini_Indr_6713No ratings yet
- 09 T016 40473Document15 pages09 T016 40473Darmawan RizkyNo ratings yet
- Conventional Chest Physical Therapy For Obstructive Lung DiseaseDocument12 pagesConventional Chest Physical Therapy For Obstructive Lung DiseaseJulieta EvangelistaNo ratings yet
- Freid 2005Document14 pagesFreid 2005PaulHerreraNo ratings yet
- Autogenic DrainageDocument6 pagesAutogenic DrainagePhooi Yee LauNo ratings yet
- Japplphysiol 00119 2021Document12 pagesJapplphysiol 00119 2021Fernando Dinamarca SotoNo ratings yet
- 1 ChestDocument5 pages1 ChestZakiyah Nur HaqqiNo ratings yet
- Conventional Chest Physical Therapy For Obstructive Lung DiseaseDocument12 pagesConventional Chest Physical Therapy For Obstructive Lung DiseaseStelaA1No ratings yet
- Rclutamiento VAFO Pre Surfactante PTDocument7 pagesRclutamiento VAFO Pre Surfactante PTGustavo Carhuamaca RoblesNo ratings yet
- Ventilation During Lung Resection and Critical Care ComparativeDocument11 pagesVentilation During Lung Resection and Critical Care Comparativeema moralesNo ratings yet
- Airway Clearance Techniques and Hyperinflation Therapy Walsh Chapter 12Document25 pagesAirway Clearance Techniques and Hyperinflation Therapy Walsh Chapter 12Dennis Páez Torres100% (2)
- Jurnal 5Document7 pagesJurnal 5nskhldNo ratings yet
- 22 Effect of Incentive Spirometer Exercise On Pulmonary Functions in Children With Spastic Cerebral PalsyDocument6 pages22 Effect of Incentive Spirometer Exercise On Pulmonary Functions in Children With Spastic Cerebral PalsyDoaa TammamNo ratings yet
- Anaesthesia - 2016 - Song - Effects of An Alveolar Recruitment Manoeuvre Guided by Lung Ultrasound On Anaesthesia InducedDocument10 pagesAnaesthesia - 2016 - Song - Effects of An Alveolar Recruitment Manoeuvre Guided by Lung Ultrasound On Anaesthesia InducedAlexandra NemesNo ratings yet
- Driving Pressure Study OLVDocument13 pagesDriving Pressure Study OLVlucasNo ratings yet
- Influence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientsDocument6 pagesInfluence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientscamiladelgadomNo ratings yet
- Hfo 3Document8 pagesHfo 3markus_danusantosoNo ratings yet
- A Retrospective Study of Success, Failure, and Time Needed To Perform Awake IntubationDocument10 pagesA Retrospective Study of Success, Failure, and Time Needed To Perform Awake IntubationAinun RamadaniNo ratings yet
- Chest Physical Therapy For Patients in The Intensive Care Unit (APTA Journal)Document19 pagesChest Physical Therapy For Patients in The Intensive Care Unit (APTA Journal)Physio EbookNo ratings yet
- Hfo 2Document9 pagesHfo 2markus_danusantosoNo ratings yet
- Airway Clearance TherapiesDocument12 pagesAirway Clearance TherapiesMiguelandry PérezNo ratings yet
- Chest Physiotherapy in Mechanically Ventilated Children A ReviewDocument10 pagesChest Physiotherapy in Mechanically Ventilated Children A Reviewmrizki_1No ratings yet
- Role of PhysiotherapyDocument23 pagesRole of PhysiotherapyVikas ChaitanyaNo ratings yet
- Proforma For Registration of Subjects For DissertationDocument16 pagesProforma For Registration of Subjects For DissertationAldrich MabasaNo ratings yet
- The Physiologically Difficult Airway: Eview RticleDocument9 pagesThe Physiologically Difficult Airway: Eview RticleEdson Llerena SalvoNo ratings yet
- Chest Physiotherapy in Children With Acute Bacterial PneumoniaDocument10 pagesChest Physiotherapy in Children With Acute Bacterial PneumoniaEka BagaskaraNo ratings yet
- The ABC of Weaning Failure - A Structured ApproachDocument9 pagesThe ABC of Weaning Failure - A Structured ApproachArul ShanmugamNo ratings yet
- Autogenic 1 PDFDocument5 pagesAutogenic 1 PDFpermanaNo ratings yet
- Ajrcccm 2004Document9 pagesAjrcccm 2004kichilla1No ratings yet
- Journal of Anesthesia & Clinical ResearchDocument8 pagesJournal of Anesthesia & Clinical ResearchAyu Aprilisa D PutriNo ratings yet
- Care Unit Chest Physical Therapy For Patients in The IntensiveDocument19 pagesCare Unit Chest Physical Therapy For Patients in The IntensivezaqiyahNo ratings yet
- Como Optimizar La EntubaciónDocument4 pagesComo Optimizar La EntubaciónKaren Aline Gómez CruzNo ratings yet
- KTR Tecnica EvidenciaDocument12 pagesKTR Tecnica EvidenciacarlitrossotoNo ratings yet
- Esophageal and Transpulmonary Pressure in The Clinical Setting - Meaning, Usefulness and PerspectivesDocument14 pagesEsophageal and Transpulmonary Pressure in The Clinical Setting - Meaning, Usefulness and PerspectivesSüleyman YıldırımNo ratings yet
- Research Proposal: MPT (Cardio Respiratory Disorders)Document14 pagesResearch Proposal: MPT (Cardio Respiratory Disorders)permanaNo ratings yet
- Effectiveness of Airway ClearanceDocument7 pagesEffectiveness of Airway ClearanceNelly Lutfieta SariNo ratings yet
- Wa0042.Document4 pagesWa0042.ENFERMERIA EMERGENCIANo ratings yet
- An Evaluation of Chest Physiotherapy in The Management of Acute Bronchiolitis Changing Clinical Practice PDFDocument6 pagesAn Evaluation of Chest Physiotherapy in The Management of Acute Bronchiolitis Changing Clinical Practice PDFKopi143No ratings yet
- Lung and Diaphragm Protective Ventilation Guided by The EsophagealDocument3 pagesLung and Diaphragm Protective Ventilation Guided by The Esophagealema moralesNo ratings yet
- Fessler - 2010Document12 pagesFessler - 2010Cindy KarmilaNo ratings yet
- Chest Physical Therapy For Patients in Intensive Care Unit: Key WordsDocument17 pagesChest Physical Therapy For Patients in Intensive Care Unit: Key WordsNeil Francis VillagonzaloNo ratings yet
- Ventilación Del Pulmón Sano CC Current 20Document5 pagesVentilación Del Pulmón Sano CC Current 20Silvia Lorena Mireles GonzálezNo ratings yet
- 36 Update On Ventilatory Management of Extremely Preterm InfantsDocument9 pages36 Update On Ventilatory Management of Extremely Preterm Infantsema moralesNo ratings yet
- Rehabilitacion Pulmonar en La UciDocument19 pagesRehabilitacion Pulmonar en La UcimavhelllinaNo ratings yet
- Atelectasias en ObesosDocument6 pagesAtelectasias en ObesosHernan Dario GuerreroNo ratings yet
- Chatham 2004Document5 pagesChatham 2004raul huertaNo ratings yet
- Mauri 2017 - Optimum Support by High Flow Nasal Cannula in AHRFDocument11 pagesMauri 2017 - Optimum Support by High Flow Nasal Cannula in AHRFgiadungdanamallNo ratings yet
- Kim 2017 PDFDocument7 pagesKim 2017 PDFPablo IgnacioNo ratings yet
- ResuscitationDocument8 pagesResuscitation85tq5nhsqbNo ratings yet
- PEEP - Ventilação - Perfusão em Prona e Supino ArtigosDocument9 pagesPEEP - Ventilação - Perfusão em Prona e Supino Artigosle franchiNo ratings yet
- Effect of Volume-Oriented Versus Flow-Oriented Incentive Spirometry On Chest Wall Volumes, Inspiratory Muscle Activity, and Thoracoabdominal Synchrony in The ElderlyDocument7 pagesEffect of Volume-Oriented Versus Flow-Oriented Incentive Spirometry On Chest Wall Volumes, Inspiratory Muscle Activity, and Thoracoabdominal Synchrony in The ElderlyErina SeptianaNo ratings yet
- Paper MaryorieDocument9 pagesPaper MaryoriekakokineNo ratings yet
- Airway Management During Upper GI Endoscopic Procedures2016Document9 pagesAirway Management During Upper GI Endoscopic Procedures2016jcarl_20063003No ratings yet
- Rochat ...Document11 pagesRochat ...Vanessa SuazoNo ratings yet
- Chest Physical Therapy For Patients in Intensive Care Unit: Key WordsDocument17 pagesChest Physical Therapy For Patients in Intensive Care Unit: Key Wordsketrin maladaNo ratings yet
- PIIS1744165X23000677Document10 pagesPIIS1744165X23000677crislatorreferNo ratings yet
- RCCM 201902-0334ocDocument10 pagesRCCM 201902-0334ocrodolfo riosNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- J Physio 2006 09 004Document5 pagesJ Physio 2006 09 004ganesh goreNo ratings yet
- Chest Physiotherapy in Mechanically Ventilated Children: A ReviewDocument8 pagesChest Physiotherapy in Mechanically Ventilated Children: A Reviewganesh goreNo ratings yet
- Co 2Document5 pagesCo 2ganesh goreNo ratings yet
- Agneta 2Document13 pagesAgneta 2ganesh goreNo ratings yet
- Helicure - Google SearchDocument1 pageHelicure - Google Searchalijan deparNo ratings yet
- Sustainable Development Is To Make A World A Better Place For Everyone Now Without Destroying The Possibilities For The Next Generations.Document3 pagesSustainable Development Is To Make A World A Better Place For Everyone Now Without Destroying The Possibilities For The Next Generations.rico molNo ratings yet
- Roberto Padlan (Resume)Document5 pagesRoberto Padlan (Resume)Merian PadlanNo ratings yet
- Guide For Alternative Inhalers During Stock Shortages Related To Coronavirus (COVID-19)Document2 pagesGuide For Alternative Inhalers During Stock Shortages Related To Coronavirus (COVID-19)Devs AbdouNo ratings yet
- Essay GardeningDocument1 pageEssay Gardeningsharen310895660% (1)
- Hyperemesis Gravidarum ProtocolDocument6 pagesHyperemesis Gravidarum ProtocolArumDesiPratiwi0% (1)
- Kinerja Pusk Kalikajar I 2015Document32 pagesKinerja Pusk Kalikajar I 2015asabri yunisNo ratings yet
- Analysis of Breastfeeding Pattern With Early Childhood CariesDocument4 pagesAnalysis of Breastfeeding Pattern With Early Childhood CariesSusi susiNo ratings yet
- Cancer TypesDocument12 pagesCancer TypeskisNo ratings yet
- Comparison of High-Grade and Low-Grade Mobilization Techniques in The Management of Adhesive Capsulitis of The Shoulder: Randomized Controlled TrialDocument14 pagesComparison of High-Grade and Low-Grade Mobilization Techniques in The Management of Adhesive Capsulitis of The Shoulder: Randomized Controlled TrialLakshmi PrasannaNo ratings yet
- What Causes Iron-Deficiency Anemia?Document2 pagesWhat Causes Iron-Deficiency Anemia?AidaDesNo ratings yet
- Food Security and Vision 2025Document38 pagesFood Security and Vision 2025madihaNo ratings yet
- DiabeticRetPPP2014 SummaryBenchmarkPagesDocument2 pagesDiabeticRetPPP2014 SummaryBenchmarkPageskomite medikNo ratings yet
- The Evolution of Biotechnology and Its Impact On Health CareDocument10 pagesThe Evolution of Biotechnology and Its Impact On Health Carejose david obeso morenoNo ratings yet
- Concept Paper: Submitted By: John Paul T. Yu BSPA - 3A Submitted To: Ma'am Maha Dumama MidtimbangDocument3 pagesConcept Paper: Submitted By: John Paul T. Yu BSPA - 3A Submitted To: Ma'am Maha Dumama MidtimbangMark TayuanNo ratings yet
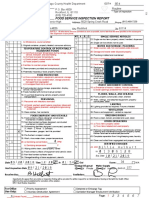
- Winnebago County Health Department, Food Service Inspection Report, Guilford High SchoolDocument7 pagesWinnebago County Health Department, Food Service Inspection Report, Guilford High Schoolcorina curryNo ratings yet
- NCM 114 Topic 4 Comprehensive Geriatric AssessmentDocument16 pagesNCM 114 Topic 4 Comprehensive Geriatric AssessmentCaitlynNo ratings yet
- Chapter 1Document52 pagesChapter 1marialourdes2489100% (15)
- Benefits of Aerobics, Zumba, Pilates, and Tae BoDocument3 pagesBenefits of Aerobics, Zumba, Pilates, and Tae BoTRIXIEJOY INIONNo ratings yet
- Career Technology Learners Resource Pack (Corrected)Document72 pagesCareer Technology Learners Resource Pack (Corrected)Tejasvini HummingwaveNo ratings yet
- Top 10 Herbs For Cancer in Ayurveda - Cancer TreatmentDocument8 pagesTop 10 Herbs For Cancer in Ayurveda - Cancer TreatmentSN WijesinheNo ratings yet
- Case Pres 317 - GADDocument25 pagesCase Pres 317 - GADPAOLA LUZ CRUZNo ratings yet
- Orchitis 160406115741Document28 pagesOrchitis 160406115741Right VentricleNo ratings yet
- Benelam 2009 Nutrition - BulletinDocument48 pagesBenelam 2009 Nutrition - BulletinCarlos Julio Fonseca SilvaNo ratings yet
- Theatre Operational PolicyDocument26 pagesTheatre Operational PolicyEmma Sunday OdyenyNo ratings yet
- HES 032 BSN - Lab Comprehensive ExamDocument40 pagesHES 032 BSN - Lab Comprehensive ExamDIAZ, GIANNA D.No ratings yet
- PharmacyDocument19 pagesPharmacyBotemi0% (1)




























































































Download as pdf or txt
You might also like
- Margaret McWilliams-Fundamentals of Meal ManagementDocument361 pagesMargaret McWilliams-Fundamentals of Meal ManagementSaher Yasin89% (9)
- Floor Cleaner Sunlight - NC Lau Sàn SunlightDocument3 pagesFloor Cleaner Sunlight - NC Lau Sàn Sunlightnhật minh nguyễnNo ratings yet
- Physiotherapy and Airway Clearance Techniques and Devices: Maggie McilwaineDocument3 pagesPhysiotherapy and Airway Clearance Techniques and Devices: Maggie Mcilwaineحسام الوجيهNo ratings yet
- Crit Care Med.: Krause@kkl200.ukl - Uni-Freiburg - de Back To TopDocument11 pagesCrit Care Med.: Krause@kkl200.ukl - Uni-Freiburg - de Back To TopTharshini_Indr_6713No ratings yet
- 09 T016 40473Document15 pages09 T016 40473Darmawan RizkyNo ratings yet
- Conventional Chest Physical Therapy For Obstructive Lung DiseaseDocument12 pagesConventional Chest Physical Therapy For Obstructive Lung DiseaseJulieta EvangelistaNo ratings yet
- Freid 2005Document14 pagesFreid 2005PaulHerreraNo ratings yet
- Autogenic DrainageDocument6 pagesAutogenic DrainagePhooi Yee LauNo ratings yet
- Japplphysiol 00119 2021Document12 pagesJapplphysiol 00119 2021Fernando Dinamarca SotoNo ratings yet
- 1 ChestDocument5 pages1 ChestZakiyah Nur HaqqiNo ratings yet
- Conventional Chest Physical Therapy For Obstructive Lung DiseaseDocument12 pagesConventional Chest Physical Therapy For Obstructive Lung DiseaseStelaA1No ratings yet
- Rclutamiento VAFO Pre Surfactante PTDocument7 pagesRclutamiento VAFO Pre Surfactante PTGustavo Carhuamaca RoblesNo ratings yet
- Ventilation During Lung Resection and Critical Care ComparativeDocument11 pagesVentilation During Lung Resection and Critical Care Comparativeema moralesNo ratings yet
- Airway Clearance Techniques and Hyperinflation Therapy Walsh Chapter 12Document25 pagesAirway Clearance Techniques and Hyperinflation Therapy Walsh Chapter 12Dennis Páez Torres100% (2)
- Jurnal 5Document7 pagesJurnal 5nskhldNo ratings yet
- 22 Effect of Incentive Spirometer Exercise On Pulmonary Functions in Children With Spastic Cerebral PalsyDocument6 pages22 Effect of Incentive Spirometer Exercise On Pulmonary Functions in Children With Spastic Cerebral PalsyDoaa TammamNo ratings yet
- Anaesthesia - 2016 - Song - Effects of An Alveolar Recruitment Manoeuvre Guided by Lung Ultrasound On Anaesthesia InducedDocument10 pagesAnaesthesia - 2016 - Song - Effects of An Alveolar Recruitment Manoeuvre Guided by Lung Ultrasound On Anaesthesia InducedAlexandra NemesNo ratings yet
- Driving Pressure Study OLVDocument13 pagesDriving Pressure Study OLVlucasNo ratings yet
- Influence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientsDocument6 pagesInfluence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientscamiladelgadomNo ratings yet
- Hfo 3Document8 pagesHfo 3markus_danusantosoNo ratings yet
- A Retrospective Study of Success, Failure, and Time Needed To Perform Awake IntubationDocument10 pagesA Retrospective Study of Success, Failure, and Time Needed To Perform Awake IntubationAinun RamadaniNo ratings yet
- Chest Physical Therapy For Patients in The Intensive Care Unit (APTA Journal)Document19 pagesChest Physical Therapy For Patients in The Intensive Care Unit (APTA Journal)Physio EbookNo ratings yet
- Hfo 2Document9 pagesHfo 2markus_danusantosoNo ratings yet
- Airway Clearance TherapiesDocument12 pagesAirway Clearance TherapiesMiguelandry PérezNo ratings yet
- Chest Physiotherapy in Mechanically Ventilated Children A ReviewDocument10 pagesChest Physiotherapy in Mechanically Ventilated Children A Reviewmrizki_1No ratings yet
- Role of PhysiotherapyDocument23 pagesRole of PhysiotherapyVikas ChaitanyaNo ratings yet
- Proforma For Registration of Subjects For DissertationDocument16 pagesProforma For Registration of Subjects For DissertationAldrich MabasaNo ratings yet
- The Physiologically Difficult Airway: Eview RticleDocument9 pagesThe Physiologically Difficult Airway: Eview RticleEdson Llerena SalvoNo ratings yet
- Chest Physiotherapy in Children With Acute Bacterial PneumoniaDocument10 pagesChest Physiotherapy in Children With Acute Bacterial PneumoniaEka BagaskaraNo ratings yet
- The ABC of Weaning Failure - A Structured ApproachDocument9 pagesThe ABC of Weaning Failure - A Structured ApproachArul ShanmugamNo ratings yet
- Autogenic 1 PDFDocument5 pagesAutogenic 1 PDFpermanaNo ratings yet
- Ajrcccm 2004Document9 pagesAjrcccm 2004kichilla1No ratings yet
- Journal of Anesthesia & Clinical ResearchDocument8 pagesJournal of Anesthesia & Clinical ResearchAyu Aprilisa D PutriNo ratings yet
- Care Unit Chest Physical Therapy For Patients in The IntensiveDocument19 pagesCare Unit Chest Physical Therapy For Patients in The IntensivezaqiyahNo ratings yet
- Como Optimizar La EntubaciónDocument4 pagesComo Optimizar La EntubaciónKaren Aline Gómez CruzNo ratings yet
- KTR Tecnica EvidenciaDocument12 pagesKTR Tecnica EvidenciacarlitrossotoNo ratings yet
- Esophageal and Transpulmonary Pressure in The Clinical Setting - Meaning, Usefulness and PerspectivesDocument14 pagesEsophageal and Transpulmonary Pressure in The Clinical Setting - Meaning, Usefulness and PerspectivesSüleyman YıldırımNo ratings yet
- Research Proposal: MPT (Cardio Respiratory Disorders)Document14 pagesResearch Proposal: MPT (Cardio Respiratory Disorders)permanaNo ratings yet
- Effectiveness of Airway ClearanceDocument7 pagesEffectiveness of Airway ClearanceNelly Lutfieta SariNo ratings yet
- Wa0042.Document4 pagesWa0042.ENFERMERIA EMERGENCIANo ratings yet
- An Evaluation of Chest Physiotherapy in The Management of Acute Bronchiolitis Changing Clinical Practice PDFDocument6 pagesAn Evaluation of Chest Physiotherapy in The Management of Acute Bronchiolitis Changing Clinical Practice PDFKopi143No ratings yet
- Lung and Diaphragm Protective Ventilation Guided by The EsophagealDocument3 pagesLung and Diaphragm Protective Ventilation Guided by The Esophagealema moralesNo ratings yet
- Fessler - 2010Document12 pagesFessler - 2010Cindy KarmilaNo ratings yet
- Chest Physical Therapy For Patients in Intensive Care Unit: Key WordsDocument17 pagesChest Physical Therapy For Patients in Intensive Care Unit: Key WordsNeil Francis VillagonzaloNo ratings yet
- Ventilación Del Pulmón Sano CC Current 20Document5 pagesVentilación Del Pulmón Sano CC Current 20Silvia Lorena Mireles GonzálezNo ratings yet
- 36 Update On Ventilatory Management of Extremely Preterm InfantsDocument9 pages36 Update On Ventilatory Management of Extremely Preterm Infantsema moralesNo ratings yet
- Rehabilitacion Pulmonar en La UciDocument19 pagesRehabilitacion Pulmonar en La UcimavhelllinaNo ratings yet
- Atelectasias en ObesosDocument6 pagesAtelectasias en ObesosHernan Dario GuerreroNo ratings yet
- Chatham 2004Document5 pagesChatham 2004raul huertaNo ratings yet
- Mauri 2017 - Optimum Support by High Flow Nasal Cannula in AHRFDocument11 pagesMauri 2017 - Optimum Support by High Flow Nasal Cannula in AHRFgiadungdanamallNo ratings yet
- Kim 2017 PDFDocument7 pagesKim 2017 PDFPablo IgnacioNo ratings yet
- ResuscitationDocument8 pagesResuscitation85tq5nhsqbNo ratings yet
- PEEP - Ventilação - Perfusão em Prona e Supino ArtigosDocument9 pagesPEEP - Ventilação - Perfusão em Prona e Supino Artigosle franchiNo ratings yet
- Effect of Volume-Oriented Versus Flow-Oriented Incentive Spirometry On Chest Wall Volumes, Inspiratory Muscle Activity, and Thoracoabdominal Synchrony in The ElderlyDocument7 pagesEffect of Volume-Oriented Versus Flow-Oriented Incentive Spirometry On Chest Wall Volumes, Inspiratory Muscle Activity, and Thoracoabdominal Synchrony in The ElderlyErina SeptianaNo ratings yet
- Paper MaryorieDocument9 pagesPaper MaryoriekakokineNo ratings yet
- Airway Management During Upper GI Endoscopic Procedures2016Document9 pagesAirway Management During Upper GI Endoscopic Procedures2016jcarl_20063003No ratings yet
- Rochat ...Document11 pagesRochat ...Vanessa SuazoNo ratings yet
- Chest Physical Therapy For Patients in Intensive Care Unit: Key WordsDocument17 pagesChest Physical Therapy For Patients in Intensive Care Unit: Key Wordsketrin maladaNo ratings yet
- PIIS1744165X23000677Document10 pagesPIIS1744165X23000677crislatorreferNo ratings yet
- RCCM 201902-0334ocDocument10 pagesRCCM 201902-0334ocrodolfo riosNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- J Physio 2006 09 004Document5 pagesJ Physio 2006 09 004ganesh goreNo ratings yet
- Chest Physiotherapy in Mechanically Ventilated Children: A ReviewDocument8 pagesChest Physiotherapy in Mechanically Ventilated Children: A Reviewganesh goreNo ratings yet
- Co 2Document5 pagesCo 2ganesh goreNo ratings yet
- Agneta 2Document13 pagesAgneta 2ganesh goreNo ratings yet
- Helicure - Google SearchDocument1 pageHelicure - Google Searchalijan deparNo ratings yet
- Sustainable Development Is To Make A World A Better Place For Everyone Now Without Destroying The Possibilities For The Next Generations.Document3 pagesSustainable Development Is To Make A World A Better Place For Everyone Now Without Destroying The Possibilities For The Next Generations.rico molNo ratings yet
- Roberto Padlan (Resume)Document5 pagesRoberto Padlan (Resume)Merian PadlanNo ratings yet
- Guide For Alternative Inhalers During Stock Shortages Related To Coronavirus (COVID-19)Document2 pagesGuide For Alternative Inhalers During Stock Shortages Related To Coronavirus (COVID-19)Devs AbdouNo ratings yet
- Essay GardeningDocument1 pageEssay Gardeningsharen310895660% (1)
- Hyperemesis Gravidarum ProtocolDocument6 pagesHyperemesis Gravidarum ProtocolArumDesiPratiwi0% (1)
- Kinerja Pusk Kalikajar I 2015Document32 pagesKinerja Pusk Kalikajar I 2015asabri yunisNo ratings yet
- Analysis of Breastfeeding Pattern With Early Childhood CariesDocument4 pagesAnalysis of Breastfeeding Pattern With Early Childhood CariesSusi susiNo ratings yet
- Cancer TypesDocument12 pagesCancer TypeskisNo ratings yet
- Comparison of High-Grade and Low-Grade Mobilization Techniques in The Management of Adhesive Capsulitis of The Shoulder: Randomized Controlled TrialDocument14 pagesComparison of High-Grade and Low-Grade Mobilization Techniques in The Management of Adhesive Capsulitis of The Shoulder: Randomized Controlled TrialLakshmi PrasannaNo ratings yet
- What Causes Iron-Deficiency Anemia?Document2 pagesWhat Causes Iron-Deficiency Anemia?AidaDesNo ratings yet
- Food Security and Vision 2025Document38 pagesFood Security and Vision 2025madihaNo ratings yet
- DiabeticRetPPP2014 SummaryBenchmarkPagesDocument2 pagesDiabeticRetPPP2014 SummaryBenchmarkPageskomite medikNo ratings yet
- The Evolution of Biotechnology and Its Impact On Health CareDocument10 pagesThe Evolution of Biotechnology and Its Impact On Health Carejose david obeso morenoNo ratings yet
- Concept Paper: Submitted By: John Paul T. Yu BSPA - 3A Submitted To: Ma'am Maha Dumama MidtimbangDocument3 pagesConcept Paper: Submitted By: John Paul T. Yu BSPA - 3A Submitted To: Ma'am Maha Dumama MidtimbangMark TayuanNo ratings yet
- Winnebago County Health Department, Food Service Inspection Report, Guilford High SchoolDocument7 pagesWinnebago County Health Department, Food Service Inspection Report, Guilford High Schoolcorina curryNo ratings yet
- NCM 114 Topic 4 Comprehensive Geriatric AssessmentDocument16 pagesNCM 114 Topic 4 Comprehensive Geriatric AssessmentCaitlynNo ratings yet
- Chapter 1Document52 pagesChapter 1marialourdes2489100% (15)
- Benefits of Aerobics, Zumba, Pilates, and Tae BoDocument3 pagesBenefits of Aerobics, Zumba, Pilates, and Tae BoTRIXIEJOY INIONNo ratings yet
- Career Technology Learners Resource Pack (Corrected)Document72 pagesCareer Technology Learners Resource Pack (Corrected)Tejasvini HummingwaveNo ratings yet
- Top 10 Herbs For Cancer in Ayurveda - Cancer TreatmentDocument8 pagesTop 10 Herbs For Cancer in Ayurveda - Cancer TreatmentSN WijesinheNo ratings yet
- Case Pres 317 - GADDocument25 pagesCase Pres 317 - GADPAOLA LUZ CRUZNo ratings yet
- Orchitis 160406115741Document28 pagesOrchitis 160406115741Right VentricleNo ratings yet
- Benelam 2009 Nutrition - BulletinDocument48 pagesBenelam 2009 Nutrition - BulletinCarlos Julio Fonseca SilvaNo ratings yet
- Theatre Operational PolicyDocument26 pagesTheatre Operational PolicyEmma Sunday OdyenyNo ratings yet
- HES 032 BSN - Lab Comprehensive ExamDocument40 pagesHES 032 BSN - Lab Comprehensive ExamDIAZ, GIANNA D.No ratings yet
- PharmacyDocument19 pagesPharmacyBotemi0% (1)