Download as pdf or txt
You might also like
- Guideline Watch 2021Document24 pagesGuideline Watch 2021Pedro NicolatoNo ratings yet
- Acute Kidney Injury - Seminar Lancet 2019Document16 pagesAcute Kidney Injury - Seminar Lancet 2019Giliana P. García AcevedoNo ratings yet
- Understanding Chronic Kidney Disease: A guide for the non-specialistFrom EverandUnderstanding Chronic Kidney Disease: A guide for the non-specialistRating: 4 out of 5 stars4/5 (3)
- Anemia Concept Mapping. Group 1Document82 pagesAnemia Concept Mapping. Group 1Giselle EstoquiaNo ratings yet
- AdimeDocument4 pagesAdimeapi-294212644No ratings yet
- Obgyn NotesDocument2 pagesObgyn NotesBillie AllenNo ratings yet
- Clinical Guidance: Acute Kidney InjuryDocument25 pagesClinical Guidance: Acute Kidney Injuryfahad nokiaNo ratings yet
- Aki 1Document9 pagesAki 1MARCELO DE ROSANo ratings yet
- 2020 Article 390Document2 pages2020 Article 390Riswanto RuslanNo ratings yet
- Prevention and Management of Acute Kidney InjuryDocument30 pagesPrevention and Management of Acute Kidney InjuryIren DawsonNo ratings yet
- The Definition of Acute Kidney Injury and Its Use in PracticeDocument12 pagesThe Definition of Acute Kidney Injury and Its Use in PracticeErwin SiahaanNo ratings yet
- Ben-Haim Et Al. 2022 - Forced Diuresis With Matched Isotonic Intravenous Hydration Prevents Renal Contrast Media Accumulation PDFDocument10 pagesBen-Haim Et Al. 2022 - Forced Diuresis With Matched Isotonic Intravenous Hydration Prevents Renal Contrast Media Accumulation PDFadm kdmyNo ratings yet
- Acut Kidney InjuryDocument12 pagesAcut Kidney InjuryorriNo ratings yet
- AKI Perioperatif 2Document12 pagesAKI Perioperatif 2Kevin JohanesNo ratings yet
- Acute Kidney Injury: Current Concepts and New Insights: Key WordsDocument5 pagesAcute Kidney Injury: Current Concepts and New Insights: Key WordsIHNo ratings yet
- Periop AKIDocument12 pagesPeriop AKINavjot KaurNo ratings yet
- Acute Kidney Injury - Final Draft (08 January 2011)Document58 pagesAcute Kidney Injury - Final Draft (08 January 2011)Mary-kate HengNo ratings yet
- Acute Kidney Injury An UpdateDocument9 pagesAcute Kidney Injury An Updatekarol fernandezNo ratings yet
- Diagnosis and Treatment of Acute Kidney Injury in PediatricsDocument13 pagesDiagnosis and Treatment of Acute Kidney Injury in PediatricsagungNo ratings yet
- The Japanese Clinical Practice Guideline For Acute Kidney Injury 2016Document55 pagesThe Japanese Clinical Practice Guideline For Acute Kidney Injury 2016RobertNo ratings yet
- Incidence and Characteristics of Acute Kidney Injury in Severe Diabetic KetoacidosisDocument6 pagesIncidence and Characteristics of Acute Kidney Injury in Severe Diabetic KetoacidosisMarcelliaNo ratings yet
- Study of Clinical Profile of Patient With Acute Kidney DiseaseDocument7 pagesStudy of Clinical Profile of Patient With Acute Kidney DiseaseIJAR JOURNALNo ratings yet
- Aas 13308Document11 pagesAas 13308kbfx6vxnjzNo ratings yet
- AKI - Acute Kidney Injury Classification RIFLE and AKIN CriteriaDocument6 pagesAKI - Acute Kidney Injury Classification RIFLE and AKIN CriteriaIntan Siti HulaimaNo ratings yet
- The Definition of Acute Kidney Injury and Its Use in PracticeDocument12 pagesThe Definition of Acute Kidney Injury and Its Use in PracticewelinNo ratings yet
- 16 PDFDocument8 pages16 PDFAkhileshNo ratings yet
- Aki AcpDocument21 pagesAki AcpAndrés FelipeNo ratings yet
- NHS England AKI Webinar Final Version AaaaaaaaaaaaaadsadadaDocument18 pagesNHS England AKI Webinar Final Version AaaaaaaaaaaaaadsadadaAlmen Pandangan AdjulNo ratings yet
- Prerenalacutekidneyinjury 2020Document9 pagesPrerenalacutekidneyinjury 2020diana ramirezNo ratings yet
- FINAL AKI GuidelineDocument120 pagesFINAL AKI GuidelineArjun Kumar Adhikari100% (1)
- Acute Kidney Injury Review 2017Document20 pagesAcute Kidney Injury Review 2017Eduardo MoraesNo ratings yet
- Síndrome Hepatorrenal Cirrosis Eur Gast J 2021Document9 pagesSíndrome Hepatorrenal Cirrosis Eur Gast J 2021Anabel GonzalezNo ratings yet
- Research Article: Incidence and Risk Factors For Early Acute Kidney Injury in Nonsurgical Patients: A Cohort StudyDocument9 pagesResearch Article: Incidence and Risk Factors For Early Acute Kidney Injury in Nonsurgical Patients: A Cohort StudyAbdul RahimNo ratings yet
- Acute Kidney Injury 2019Document16 pagesAcute Kidney Injury 2019ShadowK 99No ratings yet
- Seminars in Fetal and Neonatal MedicineDocument9 pagesSeminars in Fetal and Neonatal MedicineI SakinNo ratings yet
- Segar 2021Document9 pagesSegar 2021I SakinNo ratings yet
- Recognition and Management of Acute Kidney Injury: Thomas Oates and Shabbir MoochhalaDocument5 pagesRecognition and Management of Acute Kidney Injury: Thomas Oates and Shabbir MoochhalaIntan NoaNo ratings yet
- Aki en UciDocument9 pagesAki en UciArariwaMoralesNo ratings yet
- Renal Medicine in ICUDocument13 pagesRenal Medicine in ICUManigoldo CamelaNo ratings yet
- Acute Kidney Injury - Mark BradyDocument17 pagesAcute Kidney Injury - Mark BradyLalu Bramawangsa Banjar GetasNo ratings yet
- Covid-19 With Kidney Disorders in Dustira HospitalDocument24 pagesCovid-19 With Kidney Disorders in Dustira HospitalPbkkel 15No ratings yet
- Biomarcadores en AKIDocument14 pagesBiomarcadores en AKIhemer hadyn calderon alvitesNo ratings yet
- DDDT 14 4695Document7 pagesDDDT 14 4695IvanGómezNo ratings yet
- Study of Etiology, Clinical Profile and Outcome of Acute Kidney (AKI) in Medical Intensive Care UnitDocument4 pagesStudy of Etiology, Clinical Profile and Outcome of Acute Kidney (AKI) in Medical Intensive Care UnitDavid Al HavizNo ratings yet
- Clinical Significance of Urinary L-FABP in The Emergency DepartmentDocument7 pagesClinical Significance of Urinary L-FABP in The Emergency DepartmentmentariNo ratings yet
- Patient Outcomes Following AKI and AKD: A Population-Based Cohort StudyDocument17 pagesPatient Outcomes Following AKI and AKD: A Population-Based Cohort StudyDr Meenakshi ParwaniNo ratings yet
- Quality of Life of Caregivers and Patients On Peritoneal DialysisDocument7 pagesQuality of Life of Caregivers and Patients On Peritoneal Dialysisandrada14No ratings yet
- Management of Acute Kidney Injury: Core Curriculum 2018Document13 pagesManagement of Acute Kidney Injury: Core Curriculum 2018Kholida NabilaNo ratings yet
- Beyond FurosemideDocument13 pagesBeyond FurosemideHeath HensleyNo ratings yet
- Complications of Chronic Kidney Disease Current STDocument32 pagesComplications of Chronic Kidney Disease Current STmetaNo ratings yet
- Spectra Optia® For Automated Red Blood Cell Exchange in Patients With Sickle Cell Disease - A NICE Medical Technology GuidanceDocument14 pagesSpectra Optia® For Automated Red Blood Cell Exchange in Patients With Sickle Cell Disease - A NICE Medical Technology GuidanceNader AlharbiNo ratings yet
- Acute Kidney InjuryDocument16 pagesAcute Kidney InjuryAdo QuirozNo ratings yet
- Feline Acute Kidney Injury. 2. Approach To Diagnosis, Treatment and PrognosisDocument9 pagesFeline Acute Kidney Injury. 2. Approach To Diagnosis, Treatment and PrognosisMartín QuirogaNo ratings yet
- Kher 2017Document39 pagesKher 2017Evelyn LimNo ratings yet
- Acute Kidney Injury BMJDocument144 pagesAcute Kidney Injury BMJAreli Rolando SinarahuaNo ratings yet
- 1 s2.0 S0085253821006621 MainDocument11 pages1 s2.0 S0085253821006621 MainAllison Eunice ServandoNo ratings yet
- Management Guidelines For Gallstone Pancreatitis ADocument6 pagesManagement Guidelines For Gallstone Pancreatitis AkartikapuspitNo ratings yet
- Acute Kidney Injury LANCETDocument11 pagesAcute Kidney Injury LANCETJessica AdvínculaNo ratings yet
- Management of Acute Kidney Injury - Core Curriculum 2018Document13 pagesManagement of Acute Kidney Injury - Core Curriculum 2018Enrique Aguilar MNo ratings yet
- Falla Renal 2011Document8 pagesFalla Renal 2011Mattya SalazarNo ratings yet
- Acute Kidney Injury Lancet RoncoDocument16 pagesAcute Kidney Injury Lancet RoncoRogelio MarchanNo ratings yet
- Peritonitis Clinical Pathway PDFDocument4 pagesPeritonitis Clinical Pathway PDFIndah95No ratings yet
- Supportive Care: Integration of Patient-Centered Kidney Care To Manage Symptoms and Geriatric SyndromesDocument10 pagesSupportive Care: Integration of Patient-Centered Kidney Care To Manage Symptoms and Geriatric Syndromesyanuar esthoNo ratings yet
- HPV Diagnosis Is There An Impact On Women's Sexual and Mental HealthDocument11 pagesHPV Diagnosis Is There An Impact On Women's Sexual and Mental HealthAlinaBNo ratings yet
- Journal Impact Factor 2017Document466 pagesJournal Impact Factor 2017hpkrsigmpsaNo ratings yet
- ILLINOIS - EE Health Policy Agreement PDFDocument2 pagesILLINOIS - EE Health Policy Agreement PDFKaren Cecilia RodriguezNo ratings yet
- Anderson2008 Levofloxasin A ReviewDocument31 pagesAnderson2008 Levofloxasin A ReviewFazdrah AssyuaraNo ratings yet
- Inst Branchwise Mds 301022Document15 pagesInst Branchwise Mds 301022White WolfNo ratings yet
- Autism Handbook Parents GuideDocument46 pagesAutism Handbook Parents Guideapi-469538687No ratings yet
- Guidelines For Data Collection On The American Nurses Association's National Quality Forum Endorsed MeasuresDocument21 pagesGuidelines For Data Collection On The American Nurses Association's National Quality Forum Endorsed MeasuresMaria Fudji HastutiNo ratings yet
- Unit 4 Heath TopicDocument32 pagesUnit 4 Heath Topicralph allan bibatNo ratings yet
- A Framework For The Veterinary ConsultationDocument14 pagesA Framework For The Veterinary ConsultationMarzthNo ratings yet
- Drug Abuse Prevention and ControlDocument40 pagesDrug Abuse Prevention and ControlAbhijit DasNo ratings yet
- 05 - Thoracic Cavity Lab - NZFDocument42 pages05 - Thoracic Cavity Lab - NZFRolin KhatibNo ratings yet
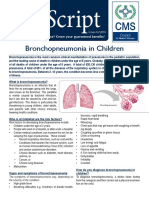
- Bronchopneumonia in ChildrenDocument3 pagesBronchopneumonia in ChildrenputraNo ratings yet
- Lecture NPPCD DeafnessDocument35 pagesLecture NPPCD DeafnessAkshay50% (2)
- ld50 ChartDocument3 pagesld50 Chartapi-320373674No ratings yet
- AOP Form 3Document4 pagesAOP Form 3Ferzada SajiranNo ratings yet
- AdiHatmoko Hospital PDFDocument100 pagesAdiHatmoko Hospital PDFina labokNo ratings yet
- Drug StudyDocument3 pagesDrug StudyfortunelobsterNo ratings yet
- Palliative Care Guiding Principles and ResourcesDocument1 pagePalliative Care Guiding Principles and ResourcesJully TNo ratings yet
- Breathe Light To Breathe Right - PDF RoomDocument58 pagesBreathe Light To Breathe Right - PDF Roomfabricio100% (3)
- Msap Safety IDocument5 pagesMsap Safety IJoseph AldrinNo ratings yet
- Date and Time Objectives Learning Contents Strategies Target Population Resources Evaluation OutcomeDocument8 pagesDate and Time Objectives Learning Contents Strategies Target Population Resources Evaluation OutcometrizzlecNo ratings yet
- Human HealthDocument9 pagesHuman HealthCreativity HouseNo ratings yet
- Mammography CMEDocument1 pageMammography CMEKirstie Marie SaldoNo ratings yet
- RBM 2530 - Tutorial 2 - Neuropathology-2011Document6 pagesRBM 2530 - Tutorial 2 - Neuropathology-2011Lina TanNo ratings yet
- Newborn CareDocument30 pagesNewborn CareAlexandria P. OrcajadaNo ratings yet
- IMNCIDocument31 pagesIMNCIJaya Prabha100% (2)