Download as pdf or txt
You might also like
- 2022 TaxReturnDocument6 pages2022 TaxReturnLALLOUS KHOURY100% (3)
- Shoplot Tenancy Agreement 2020: WhereasDocument9 pagesShoplot Tenancy Agreement 2020: WhereasChristine Liew100% (1)
- State of Content Marketing 2023Document126 pagesState of Content Marketing 2023pavan teja100% (1)
- COVID Immunization Record Correction RequestDocument1 pageCOVID Immunization Record Correction RequestNBC 10 WJAR50% (2)
- Hospital Indemnity Claim Form: Policy NumberDocument2 pagesHospital Indemnity Claim Form: Policy NumberMoyo Mitchell0% (1)
- Master Patient Index FormDocument2 pagesMaster Patient Index Formapi-355199088No ratings yet
- Auca Press 1Document15 pagesAuca Press 1Dev DuttNo ratings yet
- Consent Form - Pfizer-Biontech Covid-19 VaccineDocument2 pagesConsent Form - Pfizer-Biontech Covid-19 VaccineRommel Bucasas GarciaNo ratings yet
- Authorization For Release of Medical InformationDocument1 pageAuthorization For Release of Medical Informationcig3fNo ratings yet
- Hepatitis B HCP Reporting Form May2022Document2 pagesHepatitis B HCP Reporting Form May2022YERSON MUNARNo ratings yet
- APRIL 16TH, 2020 Text Text Text: Jaxon ScottDocument3 pagesAPRIL 16TH, 2020 Text Text Text: Jaxon Scottgordon scottNo ratings yet
- Session 3 Registration PacketDocument4 pagesSession 3 Registration PacketASYMCA YCONo ratings yet
- Checklist For New Patients or Prior Patients Not Seen Within 3 YearsDocument20 pagesChecklist For New Patients or Prior Patients Not Seen Within 3 YearsRebecca KnightNo ratings yet
- CONSENT FORM - COVID-19 VaccineDocument5 pagesCONSENT FORM - COVID-19 Vaccinebersabeh abayNo ratings yet
- COVID-19 Vaccine Consent FormDocument5 pagesCOVID-19 Vaccine Consent FormSiamakNo ratings yet
- South301 NP PaperworkDocument12 pagesSouth301 NP Paperworkdusanlu10No ratings yet
- YL Camping Consent and Health FormDocument4 pagesYL Camping Consent and Health Formmcronin1970No ratings yet
- Accident/Hospital Indemnity Wellness Benefit Claim Form: CW 061999 Page 1 of 2 02/14Document2 pagesAccident/Hospital Indemnity Wellness Benefit Claim Form: CW 061999 Page 1 of 2 02/14Stam AnNo ratings yet
- Medical Application Form: Insured Name: Inception DateDocument3 pagesMedical Application Form: Insured Name: Inception DateDidier G PeñuelaNo ratings yet
- Adult PacketDocument5 pagesAdult PacketcentraltexasentNo ratings yet
- Labama Enior X: Client Intake FormDocument2 pagesLabama Enior X: Client Intake FormNicole FrederickNo ratings yet
- MEDICARDDocument1 pageMEDICARDFei TrinidadNo ratings yet
- Family Medical Insurance Application PDFDocument6 pagesFamily Medical Insurance Application PDFScribdTranslationsNo ratings yet
- Aflac Cancer Claim FormDocument2 pagesAflac Cancer Claim FormBrian HollingtonNo ratings yet
- BivalentConsent MichaelBelen HAG322426Document2 pagesBivalentConsent MichaelBelen HAG322426michaeljohnbelen14No ratings yet
- BMS Patient Assistance FoundationDocument4 pagesBMS Patient Assistance FoundationJhoanna MonterolaNo ratings yet
- Domingo, Elvira ApplicationFormDocument1 pageDomingo, Elvira ApplicationFormelviradomingo1575No ratings yet
- New Axa FormDocument2 pagesNew Axa FormAzrul Azuar Azrul Azuar100% (1)
- Patient Registration Form: A. Demographic InformationDocument3 pagesPatient Registration Form: A. Demographic Informationyusviyah nurhidayatiNo ratings yet
- Health Statement FormDocument2 pagesHealth Statement FormRose Ann DuqueNo ratings yet
- English Financial Assistance ApplicationDocument4 pagesEnglish Financial Assistance ApplicationAlyssa JenningsNo ratings yet
- AppForm - GroupMedIns - Member - 2016-06 (June14)Document3 pagesAppForm - GroupMedIns - Member - 2016-06 (June14)Ruchie EtolleNo ratings yet
- Voluntary Group Life Insurance Application Form FinalDocument1 pageVoluntary Group Life Insurance Application Form FinalNoli Azanza IIINo ratings yet
- Youth Ministries Medical and Liability Release Kayaking Trip August 10Document4 pagesYouth Ministries Medical and Liability Release Kayaking Trip August 10DiaanNo ratings yet
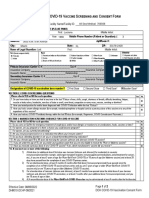
- Covid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 VaccineDocument2 pagesCovid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 Vaccinesiriamma wiliamsNo ratings yet
- Mississippi State Board of Medical Licensure: Complaint FormDocument5 pagesMississippi State Board of Medical Licensure: Complaint FormScott SistersNo ratings yet
- MetLife Basic GTL CertificateDocument63 pagesMetLife Basic GTL Certificatereddyraj036No ratings yet
- Medical Application Form PDFDocument3 pagesMedical Application Form PDFHumanNo ratings yet
- Medical Records Release Partners English PDFDocument2 pagesMedical Records Release Partners English PDFBobbie StJohnNo ratings yet
- DoGH FormDocument2 pagesDoGH FormcoolgrassNo ratings yet
- Prulife Uk Form PiDocument3 pagesPrulife Uk Form PiPaulie TitoNo ratings yet
- Vaccination Notice: Notice To Agent Is Notice To Principal Notice To Principal Is Notice To AgentDocument3 pagesVaccination Notice: Notice To Agent Is Notice To Principal Notice To Principal Is Notice To AgentOne HereNo ratings yet
- W-1QMBR BlankDocument3 pagesW-1QMBR BlankehaegertNo ratings yet
- ISS Birth MailIn FINAL Rev 1 21Document2 pagesISS Birth MailIn FINAL Rev 1 21David AcostaNo ratings yet
- COVID19 Vaccine Administration Form Rev 9222Document2 pagesCOVID19 Vaccine Administration Form Rev 9222Amín CarrilloNo ratings yet
- Application For Medicare Savings Programs (QMB, SLMB, ALMB) : State of Connecticut Department of Social ServicesDocument6 pagesApplication For Medicare Savings Programs (QMB, SLMB, ALMB) : State of Connecticut Department of Social ServicesMohammad HamidNo ratings yet
- COVID-19 Vaccination Pre-Registration Form - 1 Dose: 1. BiodataDocument2 pagesCOVID-19 Vaccination Pre-Registration Form - 1 Dose: 1. BiodataMaimoon AliNo ratings yet
- Pediatric Patient Registration Form TemplateDocument5 pagesPediatric Patient Registration Form TemplateHasfi YakobNo ratings yet
- DOH - Covid Vaccine Screening Consent FormDocument2 pagesDOH - Covid Vaccine Screening Consent FormCasey Feindt100% (1)
- Registration Forms Session 4Document4 pagesRegistration Forms Session 4ASYMCA YCONo ratings yet
- Project 2Document11 pagesProject 2api-343650991No ratings yet
- Final Check List: Revised: 4/16/13Document6 pagesFinal Check List: Revised: 4/16/13levi_sum2008No ratings yet
- D - Vaccination Minor Consent FormDocument2 pagesD - Vaccination Minor Consent FormNoemi CamberosNo ratings yet
- BivalentConsent LucianaPedrosopessoa 559154Document2 pagesBivalentConsent LucianaPedrosopessoa 559154Tatah SouzaNo ratings yet
- Proposal Form New India Floater Mediclaim Policy 21012020 - 1Document6 pagesProposal Form New India Floater Mediclaim Policy 21012020 - 1aj iseNo ratings yet
- Patient Access Request - CostcoDocument1 pagePatient Access Request - Costcocorey SgarsNo ratings yet
- Cancer WellnessDocument3 pagesCancer WellnessErin PhilbrookNo ratings yet
- Covid-19 Vaccine Consent Form: Information About Person To Receive Vaccine (Please Print)Document2 pagesCovid-19 Vaccine Consent Form: Information About Person To Receive Vaccine (Please Print)Karylle PetilNo ratings yet
- If HP Maid Combined Assessor Provider Form ElectronicDocument10 pagesIf HP Maid Combined Assessor Provider Form ElectronicdawnNo ratings yet
- The Vaccine Court: The Dark Truth of America's Vaccine Injury Compensation ProgramFrom EverandThe Vaccine Court: The Dark Truth of America's Vaccine Injury Compensation ProgramRating: 5 out of 5 stars5/5 (2)
- What Your Doctor Wants You to Know to Crush Medical Debt: A Health System Insider's 3 Steps to Protect Yourself from America's #1 Cause of BankruptcyFrom EverandWhat Your Doctor Wants You to Know to Crush Medical Debt: A Health System Insider's 3 Steps to Protect Yourself from America's #1 Cause of BankruptcyNo ratings yet
- Health Care Disparity in the United States of AmericaFrom EverandHealth Care Disparity in the United States of AmericaRating: 1 out of 5 stars1/5 (1)
- 901 Santa Fe ST BrochureDocument6 pages901 Santa Fe ST BrochureLALLOUS KHOURYNo ratings yet
- Receipt # 181848849: Payment DetailsDocument1 pageReceipt # 181848849: Payment DetailsLALLOUS KHOURYNo ratings yet
- StatementDocument2 pagesStatementLALLOUS KHOURYNo ratings yet
- Winning The Easy GameDocument18 pagesWinning The Easy GameLeonardo PiovesanNo ratings yet
- English File 4e Elementary TG PCM Comm 5ADocument1 pageEnglish File 4e Elementary TG PCM Comm 5ARaffael NuñezNo ratings yet
- Idioms and Collocations RevisionDocument3 pagesIdioms and Collocations RevisionNgọc TâmNo ratings yet
- The Prayer of The Prophet (Sallallaho Alaihe Wa Sallam)Document13 pagesThe Prayer of The Prophet (Sallallaho Alaihe Wa Sallam)Dawah ChannelNo ratings yet
- World-Wide Volkswagen Corp. v. WoodsonDocument2 pagesWorld-Wide Volkswagen Corp. v. WoodsonRonnie Barcena Jr.No ratings yet
- Mission - List Codigos Commandos 2Document3 pagesMission - List Codigos Commandos 2Cristian Andres0% (1)
- Constitution Template For Mobile Legends Esports ClubDocument5 pagesConstitution Template For Mobile Legends Esports Clubpcipm pcipmsebrangulu2plgNo ratings yet
- Advanced Vehicle Technologies, Autonomous Vehicles and CyclingDocument15 pagesAdvanced Vehicle Technologies, Autonomous Vehicles and CyclingGiampaolo PastorinoNo ratings yet
- Sur MBL - Kmtcpusg482545Document2 pagesSur MBL - Kmtcpusg482545nanaNo ratings yet
- Banaszynski v. United States Government - Document No. 4Document2 pagesBanaszynski v. United States Government - Document No. 4Justia.comNo ratings yet
- Explaining The TrinityDocument3 pagesExplaining The TrinityAriellaNo ratings yet
- Quiz - BRITISH AMERICAN CULTUREDocument16 pagesQuiz - BRITISH AMERICAN CULTUREK28 Chuyên Tin CHLNo ratings yet
- Law of Succession CATDocument11 pagesLaw of Succession CATSancho SanchezNo ratings yet
- Information Before Stay BFDocument7 pagesInformation Before Stay BFBrat SiostraNo ratings yet
- The Jet Volume 7 Number 4Document24 pagesThe Jet Volume 7 Number 4THE JETNo ratings yet
- Akshay Akshay Akshay Akshay Akshay Akshay Akshay Akshay Akshay Ashis Ashis Ashis Ashis Ashis Ashis Ashis Ashis Ashis Ashis Shrena Shrena Shrena Shrena Shrena Shrena Shrena Shrena ShrenaDocument31 pagesAkshay Akshay Akshay Akshay Akshay Akshay Akshay Akshay Akshay Ashis Ashis Ashis Ashis Ashis Ashis Ashis Ashis Ashis Ashis Shrena Shrena Shrena Shrena Shrena Shrena Shrena Shrena Shrenaashish_phadNo ratings yet
- January NightDocument7 pagesJanuary NightShazia ParveenNo ratings yet
- April 13, 2016, A.P. (DIR Series) Circular No.60Document4 pagesApril 13, 2016, A.P. (DIR Series) Circular No.60Sayan DebNo ratings yet
- Research Output of Readings in Philippine History 1Document12 pagesResearch Output of Readings in Philippine History 1Itshaaa MeeNo ratings yet
- Satire Powerpoint Without PicsDocument19 pagesSatire Powerpoint Without Picsapi-300762638No ratings yet
- NDTDocument2 pagesNDTTiến TrungNo ratings yet
- Facility Level SopDocument26 pagesFacility Level SopGuillaume TableyNo ratings yet
- Exploring Rfid'S Use in Shipping: Prepared For Kennesaw State University's Information Technology Students and StaffDocument22 pagesExploring Rfid'S Use in Shipping: Prepared For Kennesaw State University's Information Technology Students and Staffcallaway20No ratings yet
- Sri-Lanka From SamudraNewsAlerts SouthAsiaNewsAlertsDocument342 pagesSri-Lanka From SamudraNewsAlerts SouthAsiaNewsAlertsInvestor BritishNo ratings yet
- CivilPro Cases 37 and 38 Full Texts - AyingDocument15 pagesCivilPro Cases 37 and 38 Full Texts - Ayingvienuell ayingNo ratings yet
- Assignment HazardsDocument11 pagesAssignment HazardsCh TälhåNo ratings yet
- Spectra Precision FAST Survey User ManualDocument68 pagesSpectra Precision FAST Survey User ManualAlexis Olaf Montores CuNo ratings yet