Download as pdf or txt
You might also like
- 276) 2010 Cerio - Mechanism Action Clinical Benefits Colloidal Oatmeal Dermatologic PracticeDocument5 pages276) 2010 Cerio - Mechanism Action Clinical Benefits Colloidal Oatmeal Dermatologic Practicezebulon78No ratings yet
- Austrilia Health CareDocument23 pagesAustrilia Health CarePandaman PandaNo ratings yet
- Paranoid Personality Disorder PDFDocument3 pagesParanoid Personality Disorder PDFGerald Jader100% (1)
- Diabetic NephropathyDocument35 pagesDiabetic NephropathyIstanli CarrascalNo ratings yet
- Idiopathic Intussusception in Infancy and Childhood: ArticlesDocument3 pagesIdiopathic Intussusception in Infancy and Childhood: ArticlesIndana ZulfaNo ratings yet
- Peads ExtDCRDocument4 pagesPeads ExtDCRdradnanahmad82No ratings yet
- Journal of Pediatric Surgery: Indepent Review ArticlesDocument4 pagesJournal of Pediatric Surgery: Indepent Review ArticlesNur Ainatun NadrahNo ratings yet
- IdiopathicDocument3 pagesIdiopathicAulya ArchuletaNo ratings yet
- 2020 原著論文 Outcomes of Colonic Resection for Chronic Idiopathic Constipation in ChildhoodDocument4 pages2020 原著論文 Outcomes of Colonic Resection for Chronic Idiopathic Constipation in ChildhoodRyo TamuraNo ratings yet
- Laparoscopic Herniotomy For Congenital Inguinal Hernia Prospective Assessment of Feasibility and Outcome Analysis in Tertiary Center in NepalDocument5 pagesLaparoscopic Herniotomy For Congenital Inguinal Hernia Prospective Assessment of Feasibility and Outcome Analysis in Tertiary Center in NepalrhmathidayatNo ratings yet
- Air Enema and Liquid Enema For ReductionDocument3 pagesAir Enema and Liquid Enema For ReductionBrandon NegronNo ratings yet
- Colorectal Surgical Pathologies Frequency and Management in The Visceral Surgery Department of The National Hospital Donka CHU in ConakryDocument5 pagesColorectal Surgical Pathologies Frequency and Management in The Visceral Surgery Department of The National Hospital Donka CHU in ConakryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Complications Associated With Surgical Treatment of Congenital Intrinsic Duodenal ObstructionDocument4 pagesComplications Associated With Surgical Treatment of Congenital Intrinsic Duodenal ObstructionJess PeltraNo ratings yet
- Carlos A Olivares Et AlDocument3 pagesCarlos A Olivares Et AlFathiyya RizkaNo ratings yet
- Minimal Access Surgery in Children - 5 Years Institutional ExperienceDocument8 pagesMinimal Access Surgery in Children - 5 Years Institutional ExperienceGunduz AgaNo ratings yet
- Lane1999 PDFDocument6 pagesLane1999 PDFkatsuiaNo ratings yet
- Lich GregoirDocument5 pagesLich GregoirIoannis ValioulisNo ratings yet
- Torsion 1Document4 pagesTorsion 1Sharii AritonangNo ratings yet
- Number: 0420: Please See Amendment For Pennsylvania Medicaid at The End of This CPBDocument19 pagesNumber: 0420: Please See Amendment For Pennsylvania Medicaid at The End of This CPBAryanto AntoNo ratings yet
- Recurrent Thyroglossal Duct Cysts: A 15-Year Review of Presentation, Management and Outcomes From A Tertiary Paediatric InstitutionDocument6 pagesRecurrent Thyroglossal Duct Cysts: A 15-Year Review of Presentation, Management and Outcomes From A Tertiary Paediatric InstitutionTasia RozakiahNo ratings yet
- ReoperastionDocument5 pagesReoperastionanon_235857083No ratings yet
- Indian AediatricDocument2 pagesIndian AediatricMuhamad RizauddinNo ratings yet
- Dandy Walker SyndromeDocument5 pagesDandy Walker SyndromeMelia Fatrani RufaidahNo ratings yet
- Role of X Ray and USG in Patient Admitted With Acute AbdomenDocument6 pagesRole of X Ray and USG in Patient Admitted With Acute AbdomenkuramaNo ratings yet
- Primary Female Epispadias: Perineal Approach or Kelly Repair?Document7 pagesPrimary Female Epispadias: Perineal Approach or Kelly Repair?Adnan WalidNo ratings yet
- Laparoscopic Ventral Hernia Repair With Tacker Only Mesh Fixation: Single Centre ExperienceDocument5 pagesLaparoscopic Ventral Hernia Repair With Tacker Only Mesh Fixation: Single Centre ExperienceMudassar SattarNo ratings yet
- Endoscopic Interventional Management Using Adrenaline-Normal Saline Injection For Actively Bleeding Peptic Ulcers in South Kashmir, IndiaDocument6 pagesEndoscopic Interventional Management Using Adrenaline-Normal Saline Injection For Actively Bleeding Peptic Ulcers in South Kashmir, IndiaIJAR JOURNALNo ratings yet
- Complete Repair of Exstrophy Further ExpDocument3 pagesComplete Repair of Exstrophy Further ExpGündüz AğayevNo ratings yet
- A Safe and Effective Method of ControllingDocument3 pagesA Safe and Effective Method of Controllingelizabeth2112No ratings yet
- Current Success in The Treatment of Intussusception in ChildrenDocument9 pagesCurrent Success in The Treatment of Intussusception in ChildrenOby RomdhoniNo ratings yet
- The Great Ormond Street Protocol For Ward Decannulation of Children With Tracheostomy - Increasing Safety and Decreasing CostDocument8 pagesThe Great Ormond Street Protocol For Ward Decannulation of Children With Tracheostomy - Increasing Safety and Decreasing Costanitaabreu123No ratings yet
- General Considerations: 1392 International AbstractsDocument2 pagesGeneral Considerations: 1392 International Abstractsdewi sumbangNo ratings yet
- Complications of Long Operations: A Prospective Study of Morbidity Associated With Prolonged Operative Time ( 6 H)Document4 pagesComplications of Long Operations: A Prospective Study of Morbidity Associated With Prolonged Operative Time ( 6 H)Syahrir HtbNo ratings yet
- PICO InvaginasiDocument4 pagesPICO InvaginasimutimutimutiNo ratings yet
- Duplex Systems EndoscopicallyDocument5 pagesDuplex Systems EndoscopicallyIoannis ValioulisNo ratings yet
- RCCM 200601-027ocDocument7 pagesRCCM 200601-027ocDiego AndradeNo ratings yet
- Comparison of Urokinase and Video-Assisted Thoracoscopic Surgery For Treatment of Childhood EmpyemaDocument7 pagesComparison of Urokinase and Video-Assisted Thoracoscopic Surgery For Treatment of Childhood EmpyemaDr Nilesh NagdeveNo ratings yet
- 2014-Journal of Orthopaedic ResearchDocument13 pages2014-Journal of Orthopaedic ResearchChilo PrimaNo ratings yet
- Surgical Treatment of Thalamic Tumors in ChildrenDocument11 pagesSurgical Treatment of Thalamic Tumors in ChildrenPavel SebastianNo ratings yet
- Dis Colon Rectum - Endoscopic Mucosal Resection of Large Sessile Colorectal PolypsDocument10 pagesDis Colon Rectum - Endoscopic Mucosal Resection of Large Sessile Colorectal PolypsChargerNo ratings yet
- Merits of Kerrisons Punch Over Powered Drill in Endonasal DCRDocument4 pagesMerits of Kerrisons Punch Over Powered Drill in Endonasal DCRVikrant VazeNo ratings yet
- JournalDocument6 pagesJournalYosuaNo ratings yet
- Annrcse01544 0027Document3 pagesAnnrcse01544 0027Ma. Jessa Victoria VallangcaNo ratings yet
- Posterior Fossa Epidural Hematomas in CHDocument5 pagesPosterior Fossa Epidural Hematomas in CHmirmasottNo ratings yet
- Robotic Surgery For HirschsprungsDocument7 pagesRobotic Surgery For HirschsprungsmachalliNo ratings yet
- Abdomen: International Abstracts of Pediatric Surgery 593Document1 pageAbdomen: International Abstracts of Pediatric Surgery 593Yohanes WilliamNo ratings yet
- Functional Outcomes of Surgical Treatment of Ureteral Injury Following Gynecological and Obstetrical SurgeryDocument4 pagesFunctional Outcomes of Surgical Treatment of Ureteral Injury Following Gynecological and Obstetrical SurgeryKharizmaNo ratings yet
- Outcome and Complication of Paediatric Dacryocystorhinostomy at Mardan Medical Complex Ophthalmology UnitDocument3 pagesOutcome and Complication of Paediatric Dacryocystorhinostomy at Mardan Medical Complex Ophthalmology UnitInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Large-Volume Paracentesis in The Management of Ascites in ChildrenDocument5 pagesLarge-Volume Paracentesis in The Management of Ascites in ChildrenMed MorciNo ratings yet
- Rushfeldt Et Al 2008 Introducing An Asymmetric Cleft Lift Technique As A Uniform Procedure For Pilonidal Sinus SurgeryDocument5 pagesRushfeldt Et Al 2008 Introducing An Asymmetric Cleft Lift Technique As A Uniform Procedure For Pilonidal Sinus SurgeryMohammed FaragNo ratings yet
- Comparative Study Between Hydrostatic and Pneumatic Reduction For Early Intussusception in PediatricsDocument6 pagesComparative Study Between Hydrostatic and Pneumatic Reduction For Early Intussusception in PediatricsMostafa MosbehNo ratings yet
- Mid Term Results of Pneumatic Balloon Dilatation in Patients With AchalasiaDocument3 pagesMid Term Results of Pneumatic Balloon Dilatation in Patients With AchalasiaLuis PerazaNo ratings yet
- Modified Young-Dees-Leadbetter Bladder Neck Reconstruction in Patients With Successful Primary Bladder Closure Elsewhere.2018Document3 pagesModified Young-Dees-Leadbetter Bladder Neck Reconstruction in Patients With Successful Primary Bladder Closure Elsewhere.2018Gunduz AgaNo ratings yet
- HemivaginaDocument3 pagesHemivaginafitriamarizkaNo ratings yet
- Clinical Study: Delorme's Procedure For Complete Rectal Prolapse: A Study of Recurrence Patterns in The Long TermDocument6 pagesClinical Study: Delorme's Procedure For Complete Rectal Prolapse: A Study of Recurrence Patterns in The Long TermAnonymous A1ycUQ9zVINo ratings yet
- Arlen - 2016 - Outcomes of Complex Robot-AssistedDocument6 pagesArlen - 2016 - Outcomes of Complex Robot-AssistedAntonio López MolláNo ratings yet
- Endoscopic Excision of Antrochoanal PolypDocument3 pagesEndoscopic Excision of Antrochoanal PolypreginalisaNo ratings yet
- Distal Hypospadias Management at CHOP 09182017Document14 pagesDistal Hypospadias Management at CHOP 09182017kashifNo ratings yet
- Aul Agne 2010Document4 pagesAul Agne 2010Muhammad HidayatNo ratings yet
- 4 Kuratani2008Document5 pages4 Kuratani2008M RidwanNo ratings yet
- Management of Rectal Prolapse in ChildrenDocument6 pagesManagement of Rectal Prolapse in ChildrenWaNda GrNo ratings yet
- Ans 12950Document6 pagesAns 12950AYŞE GÜLŞAH ATASEVERNo ratings yet
- 12 The Optic Disc in Congenital GlaucomaDocument25 pages12 The Optic Disc in Congenital GlaucomaviticodocNo ratings yet
- Psychosocial Needs of The Elderly: Learner's GuideDocument33 pagesPsychosocial Needs of The Elderly: Learner's GuideDani PhilipNo ratings yet
- CareFusion LTV1150 BrochureDocument4 pagesCareFusion LTV1150 BrochureQasim AliNo ratings yet
- Radi 694 Brochure 1Document2 pagesRadi 694 Brochure 1api-356213702No ratings yet
- Ajr 09 2544Document7 pagesAjr 09 2544Elly LutfiasariNo ratings yet
- 13 Patient Saefty and Quality ImprovementDocument36 pages13 Patient Saefty and Quality ImprovementShafiq Ur RahmanNo ratings yet
- Drug StudyDocument12 pagesDrug Studychelsea anne80% (5)
- Introduction To Integrative TherapyDocument91 pagesIntroduction To Integrative Therapynikos kasiktsis100% (2)
- Concept of SanitationDocument12 pagesConcept of Sanitationsumanpunia100% (9)
- Systemic Couple Therapy and DepressionDocument3 pagesSystemic Couple Therapy and DepressionAna MoraisNo ratings yet
- AlcoholDocument12 pagesAlcoholLauraLoaizaNo ratings yet
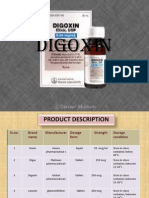
- DigoxinDocument20 pagesDigoxinAbdulRehmanChaudaryNo ratings yet
- Surya Namaskar Some Practical GuidelinesDocument5 pagesSurya Namaskar Some Practical Guidelinesarchana.mitcon4979No ratings yet
- Final Paper 603Document214 pagesFinal Paper 603api-576649735No ratings yet
- Pemberton SignDocument2 pagesPemberton SignEniryz M. SalomonNo ratings yet
- Example Personal Statement PDFDocument2 pagesExample Personal Statement PDFRajeev SrinivasNo ratings yet
- Obstructive UropathyDocument8 pagesObstructive UropathyTeslim Raji100% (1)
- Inotropes: Liverpool Health Service Intensive Care UnitDocument36 pagesInotropes: Liverpool Health Service Intensive Care Unitjudith_bruechertNo ratings yet
- Hand - Foot - Mouth Disease: Prepared By: Dr. NGUYEN QUANG DIEN Emergency DepartmentDocument24 pagesHand - Foot - Mouth Disease: Prepared By: Dr. NGUYEN QUANG DIEN Emergency DepartmentRayhan CeinNo ratings yet
- Prezentare ReabilitareDocument20 pagesPrezentare ReabilitareCenean VladNo ratings yet
- Shahnaz Husain Herbal Products Visit Us at Management - Umakant.infoDocument7 pagesShahnaz Husain Herbal Products Visit Us at Management - Umakant.infowelcome2jungleNo ratings yet
- ME Pharma Form July 2010Document3 pagesME Pharma Form July 2010darningNo ratings yet
- First Selective Relaxant Binding Agent Sugammadex: Clinical PharmacologyDocument9 pagesFirst Selective Relaxant Binding Agent Sugammadex: Clinical PharmacologyyoshiudaNo ratings yet
- Public SpeakingDocument6 pagesPublic SpeakingMosto DaniNo ratings yet
- Saskatoon Ostomy Association Bulletin For April 2016Document12 pagesSaskatoon Ostomy Association Bulletin For April 2016Peter FolkNo ratings yet
- Bja MGDocument6 pagesBja MGVignesh VenkatesanNo ratings yet
- Applying Hot and Cold WaterDocument9 pagesApplying Hot and Cold WaterdamarNo ratings yet