
Hypertriglyceridemia (962) Paper Final
Hypertriglyceridemia (962) Paper Final
You might also like
- SlimFit Gym Edition PDF PDFDocument12 pagesSlimFit Gym Edition PDF PDFyes100% (3)
- Sport and Exercise Nutrition (The Nutrition Society Textbook)Document399 pagesSport and Exercise Nutrition (The Nutrition Society Textbook)danke1122394% (17)
- The Macronutrient Blueprint PDFDocument22 pagesThe Macronutrient Blueprint PDFShirley Hernandez100% (4)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4.5 out of 5 stars4.5/5 (3)
- Case ReportDocument9 pagesCase ReportSuis MionooNo ratings yet
- Case StudyDocument5 pagesCase Studyapi-247850107No ratings yet
- Glucosa 2012Document6 pagesGlucosa 2012martynbbNo ratings yet
- Gestational Diabetes Mellitus (GDM) .TriceDocument47 pagesGestational Diabetes Mellitus (GDM) .TricejerrydanfordfxNo ratings yet
- DMDocument76 pagesDMrose ann ayala100% (1)
- 2004-Case Study Diabetes in A Patient With Cirrhosis PDFDocument5 pages2004-Case Study Diabetes in A Patient With Cirrhosis PDFAnugrah ElfaNo ratings yet
- Article PublishedDocument5 pagesArticle PublishedKamran AmeerNo ratings yet
- Case Study: Diabetes in A Patient With Cirrhosis: PresentationDocument5 pagesCase Study: Diabetes in A Patient With Cirrhosis: PresentationJohanLazuardiNo ratings yet
- InsulinaDocument8 pagesInsulinaClaudiu SufleaNo ratings yet
- Case Report NovitaDocument12 pagesCase Report NovitaChristian PoerniawanNo ratings yet
- Clinical Nutrition: Original ArticleDocument6 pagesClinical Nutrition: Original ArticleMed AjNo ratings yet
- Diabetes AssignmentDocument8 pagesDiabetes AssignmentMildred Obeng AgyeiwaaNo ratings yet
- Pharmacological Management of Type 1 DiabetesDocument6 pagesPharmacological Management of Type 1 DiabetesMI RFNo ratings yet
- Article - Ghrelin and Leptin in Insulin Resistance (CHECKED)Document6 pagesArticle - Ghrelin and Leptin in Insulin Resistance (CHECKED)pixoguiasNo ratings yet
- Disorders of Carbohydrate and Lipid Metabolism-Converted - WatermarkDocument82 pagesDisorders of Carbohydrate and Lipid Metabolism-Converted - WatermarkAbhi VarnaNo ratings yet
- DiabetesDocument26 pagesDiabetesAlina Juliana MagopetNo ratings yet
- Journal of DiabetesDocument6 pagesJournal of DiabetesSartika Rizky HapsariNo ratings yet
- Title of The Research: Diabetes Mellitus By: Abdelrahman Gamal Course Title: Pharmacology Academic Year: Fourth 2019-2020Document11 pagesTitle of The Research: Diabetes Mellitus By: Abdelrahman Gamal Course Title: Pharmacology Academic Year: Fourth 2019-2020LAZKILLERNo ratings yet
- Glycemic Variability and Hypoglycemia Before and ADocument7 pagesGlycemic Variability and Hypoglycemia Before and ALeonorNo ratings yet
- Jurnal Alun 3Document11 pagesJurnal Alun 3Dwi PurwantiNo ratings yet
- Publikasi DM Apik MedicinaDocument15 pagesPublikasi DM Apik MedicinakadekapiklestariNo ratings yet
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientDocument12 pagesManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NNo ratings yet
- Diabetic Ketoacidosis in Toddler With A Diaper RashDocument4 pagesDiabetic Ketoacidosis in Toddler With A Diaper RashKarl Angelo MontanoNo ratings yet
- Insulin Secretion and FunctionDocument8 pagesInsulin Secretion and FunctionWendy EscalanteNo ratings yet
- Diabetes MellitusDocument32 pagesDiabetes Mellitusanfalalamin9915No ratings yet
- Hipertrigliseridemia in PregnancyDocument5 pagesHipertrigliseridemia in PregnancySparkling PinkNo ratings yet
- Edit Adih LaptopDocument6 pagesEdit Adih LaptopTry Ahmad MirzaNo ratings yet
- Hepatic Glycogenosis Associated With Type 1 Diabetes (A Case Report)Document5 pagesHepatic Glycogenosis Associated With Type 1 Diabetes (A Case Report)IJAR JOURNALNo ratings yet
- Dental Management of Patients With Diabetes MellitusDocument8 pagesDental Management of Patients With Diabetes Mellitusاحمد سلامNo ratings yet
- Management of Newly Diagnosed Type 2 DiabetesDocument24 pagesManagement of Newly Diagnosed Type 2 DiabetesZulhida YuniNo ratings yet
- Exenatide Response in An Adolescent's Morbid Obesity: Pharmacology & Pharmacy, 2014, 5, 419-424Document6 pagesExenatide Response in An Adolescent's Morbid Obesity: Pharmacology & Pharmacy, 2014, 5, 419-424CamiNo ratings yet
- Nutrisi Ulseratif KolitisDocument1 pageNutrisi Ulseratif KolitisFetria MelaniNo ratings yet
- Overt Diabetes: Diabetes Mellitus in PregnancyDocument3 pagesOvert Diabetes: Diabetes Mellitus in PregnancyBrian TiopengcoNo ratings yet
- Metformin For GDMDocument7 pagesMetformin For GDMRoro WidyastutiNo ratings yet
- 66 2 171 PDFDocument5 pages66 2 171 PDF2C Sabayo Julia Andre J.No ratings yet
- Case StudyDocument3 pagesCase StudyAnnie Laiza BacayNo ratings yet
- J Clin Endocrinol Metab. 2012 97 16 38Document23 pagesJ Clin Endocrinol Metab. 2012 97 16 38rizwan234No ratings yet
- Diabetes PregnancyDocument65 pagesDiabetes PregnancyJohn Christopher LucesNo ratings yet
- Jurnal DMDocument5 pagesJurnal DMratihparmadiniNo ratings yet
- Eksperimental Metabolic-SyndromeDocument4 pagesEksperimental Metabolic-SyndromePrajna AdityaraniNo ratings yet
- Pi Is 1054139 X 13003157Document6 pagesPi Is 1054139 X 13003157Pablo Andres Encina AbrigoNo ratings yet
- Type A Insulin Resistance Syndrome and HAIRDocument2 pagesType A Insulin Resistance Syndrome and HAIRLaura BryantNo ratings yet
- Seminar 5 - DM in PregnancyDocument19 pagesSeminar 5 - DM in PregnancyHakimah K. SuhaimiNo ratings yet
- Managing Hipertriglyceridemia in Daily PracticeDocument7 pagesManaging Hipertriglyceridemia in Daily PracticeFrillyDeyanaNo ratings yet
- A Case Report of Hyperosmolar Hyperglycemic StateDocument1 pageA Case Report of Hyperosmolar Hyperglycemic StateHareesh ChanderNo ratings yet
- Indikasi Insulin InfusionDocument7 pagesIndikasi Insulin InfusionnikeNo ratings yet
- NCP Diabetes Mellitus Prepregnancy GestationalDocument12 pagesNCP Diabetes Mellitus Prepregnancy GestationalRichson BacayNo ratings yet
- Cetoacidosis Diabética Normoglicémica en El Embarazo. Caso ClínicoDocument5 pagesCetoacidosis Diabética Normoglicémica en El Embarazo. Caso ClínicoLvis Zevallos MavricioNo ratings yet
- Presentation Metabolic SyndromeDocument56 pagesPresentation Metabolic SyndromeAbdulhakeem Tleimat100% (1)
- Hypo Guidelines BrochureDocument2 pagesHypo Guidelines BrochureNellie RamosNo ratings yet
- Diabetus Mellitus: Dr. Fawzi Radi F.R.C.O.GDocument19 pagesDiabetus Mellitus: Dr. Fawzi Radi F.R.C.O.GCrissLaraNo ratings yet
- SGD 3: CASE DIABETES: "A Sweet Way To Lose Weight": Guide QuestionsDocument5 pagesSGD 3: CASE DIABETES: "A Sweet Way To Lose Weight": Guide QuestionsKaren Kaye CordovaNo ratings yet
- HypoglycemiaDocument19 pagesHypoglycemiaJesus PadillaNo ratings yet
- Diabetes in PregnencyDocument51 pagesDiabetes in PregnencyMuneeb JanNo ratings yet
- Diabetes Intraoperative Management ArticleDocument5 pagesDiabetes Intraoperative Management ArticlenesredeNo ratings yet
- Diabetes in Palliative Care CompletedDocument4 pagesDiabetes in Palliative Care Completedaya PermatasariNo ratings yet
- Katarak DM RemajaDocument8 pagesKatarak DM RemajaHIstoryNo ratings yet
- Metabolic Evaluation of Young Women With Congenital Adrenal HyperplasiaDocument7 pagesMetabolic Evaluation of Young Women With Congenital Adrenal HyperplasiaOnysapto PramanaNo ratings yet
- Neonatal Hyperglycemia: RPA Newborn Care Protocol BookDocument3 pagesNeonatal Hyperglycemia: RPA Newborn Care Protocol BookAnggia NoverinaNo ratings yet
- PCOS HealingDocument36 pagesPCOS HealingKheyrne Danu100% (1)
- How To Lose Weight Fast in 3 Simple StepsDocument8 pagesHow To Lose Weight Fast in 3 Simple StepsVarinder SinghNo ratings yet
- NCM 116 NutritionDocument9 pagesNCM 116 Nutritionrommel magoNo ratings yet
- Dairy Science and TechnologyDocument83 pagesDairy Science and Technologyیاسمین ثریاNo ratings yet
- Test Bank For Contemporary Nutrition 8th Edition Gordon WardlawDocument20 pagesTest Bank For Contemporary Nutrition 8th Edition Gordon WardlawJustin Zeches100% (34)
- Red MeatDocument9 pagesRed Meatarka prava LahiriNo ratings yet
- 1983 Speth (Garnsey Bison Kill BOOK)Document255 pages1983 Speth (Garnsey Bison Kill BOOK)jdspethNo ratings yet
- Intensive Booklet-P1-Print 2017Document20 pagesIntensive Booklet-P1-Print 2017Teacher FláviaNo ratings yet
- 2000 Cal Meal Planning GuideDocument6 pages2000 Cal Meal Planning GuideKaren MouraNo ratings yet
- Formerly: Notre Dame Hospital and School of Midwifery: 2. Identify and Discuss The Function of Macro and Micro NutrientsDocument20 pagesFormerly: Notre Dame Hospital and School of Midwifery: 2. Identify and Discuss The Function of Macro and Micro NutrientsMhianne SarmientoNo ratings yet
- Callebaut - Champ KremDocument3 pagesCallebaut - Champ KremCristian VasilescuNo ratings yet
- Nutrition in The Critically Ill PatientDocument13 pagesNutrition in The Critically Ill PatientnainazahraNo ratings yet
- Lipid PDFDocument17 pagesLipid PDFAnonymous xt41ryNo ratings yet
- Animal Nutrition - YR 10 WEEKS 2 & 3Document108 pagesAnimal Nutrition - YR 10 WEEKS 2 & 3BrioNo ratings yet
- Why Barley Is Good For Following Illnesses....Document2 pagesWhy Barley Is Good For Following Illnesses....jayarninianNo ratings yet
- Imani-Lara Lansiquot Masterclass: Half Marathon Guide Shakes For DaysDocument70 pagesImani-Lara Lansiquot Masterclass: Half Marathon Guide Shakes For DaysArnav GautamNo ratings yet
- Fibromyalgia - Causative Factors & Possible SolutionsDocument12 pagesFibromyalgia - Causative Factors & Possible SolutionsChef-doctor JemichelNo ratings yet
- Clinical Influence of Triple Omega Fatty Acids (Omega-3, 6, 9)Document3 pagesClinical Influence of Triple Omega Fatty Acids (Omega-3, 6, 9)Hạnh NguyễnNo ratings yet
- Egyptian Sweet Pastry Dessert (Umm Ali) : Start Reacting TodayDocument1 pageEgyptian Sweet Pastry Dessert (Umm Ali) : Start Reacting TodaySike Silvia GunawanNo ratings yet
- Goat Soybean Velvewt Bean GrowthDocument12 pagesGoat Soybean Velvewt Bean Growthwynferd ssNo ratings yet
- Photosynthesis Revision NoteDocument20 pagesPhotosynthesis Revision NoteUsman Mukhtar AbbasiNo ratings yet
- The Tre en en StoryDocument26 pagesThe Tre en en StoryNishit Kotak100% (1)
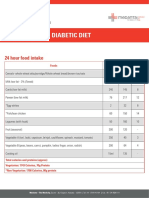
- 1800 Calories Diabetic DietDocument4 pages1800 Calories Diabetic DietNaing ooNo ratings yet
- Nutritive Value of MeatDocument16 pagesNutritive Value of MeatPooja Sri V S BE FPPTNo ratings yet
- Chemistry Holiday Homework Project For CBSE: Dry Fruit AnalysisDocument37 pagesChemistry Holiday Homework Project For CBSE: Dry Fruit AnalysisEkasNo ratings yet
- Fat Burn ConceptDocument31 pagesFat Burn ConceptManoj100% (1)
- Brochure Calibra EmailDocument24 pagesBrochure Calibra Emaila99602No ratings yet
























































































Download as docx, pdf, or txt
You might also like
- SlimFit Gym Edition PDF PDFDocument12 pagesSlimFit Gym Edition PDF PDFyes100% (3)
- Sport and Exercise Nutrition (The Nutrition Society Textbook)Document399 pagesSport and Exercise Nutrition (The Nutrition Society Textbook)danke1122394% (17)
- The Macronutrient Blueprint PDFDocument22 pagesThe Macronutrient Blueprint PDFShirley Hernandez100% (4)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4.5 out of 5 stars4.5/5 (3)
- Case ReportDocument9 pagesCase ReportSuis MionooNo ratings yet
- Case StudyDocument5 pagesCase Studyapi-247850107No ratings yet
- Glucosa 2012Document6 pagesGlucosa 2012martynbbNo ratings yet
- Gestational Diabetes Mellitus (GDM) .TriceDocument47 pagesGestational Diabetes Mellitus (GDM) .TricejerrydanfordfxNo ratings yet
- DMDocument76 pagesDMrose ann ayala100% (1)
- 2004-Case Study Diabetes in A Patient With Cirrhosis PDFDocument5 pages2004-Case Study Diabetes in A Patient With Cirrhosis PDFAnugrah ElfaNo ratings yet
- Article PublishedDocument5 pagesArticle PublishedKamran AmeerNo ratings yet
- Case Study: Diabetes in A Patient With Cirrhosis: PresentationDocument5 pagesCase Study: Diabetes in A Patient With Cirrhosis: PresentationJohanLazuardiNo ratings yet
- InsulinaDocument8 pagesInsulinaClaudiu SufleaNo ratings yet
- Case Report NovitaDocument12 pagesCase Report NovitaChristian PoerniawanNo ratings yet
- Clinical Nutrition: Original ArticleDocument6 pagesClinical Nutrition: Original ArticleMed AjNo ratings yet
- Diabetes AssignmentDocument8 pagesDiabetes AssignmentMildred Obeng AgyeiwaaNo ratings yet
- Pharmacological Management of Type 1 DiabetesDocument6 pagesPharmacological Management of Type 1 DiabetesMI RFNo ratings yet
- Article - Ghrelin and Leptin in Insulin Resistance (CHECKED)Document6 pagesArticle - Ghrelin and Leptin in Insulin Resistance (CHECKED)pixoguiasNo ratings yet
- Disorders of Carbohydrate and Lipid Metabolism-Converted - WatermarkDocument82 pagesDisorders of Carbohydrate and Lipid Metabolism-Converted - WatermarkAbhi VarnaNo ratings yet
- DiabetesDocument26 pagesDiabetesAlina Juliana MagopetNo ratings yet
- Journal of DiabetesDocument6 pagesJournal of DiabetesSartika Rizky HapsariNo ratings yet
- Title of The Research: Diabetes Mellitus By: Abdelrahman Gamal Course Title: Pharmacology Academic Year: Fourth 2019-2020Document11 pagesTitle of The Research: Diabetes Mellitus By: Abdelrahman Gamal Course Title: Pharmacology Academic Year: Fourth 2019-2020LAZKILLERNo ratings yet
- Glycemic Variability and Hypoglycemia Before and ADocument7 pagesGlycemic Variability and Hypoglycemia Before and ALeonorNo ratings yet
- Jurnal Alun 3Document11 pagesJurnal Alun 3Dwi PurwantiNo ratings yet
- Publikasi DM Apik MedicinaDocument15 pagesPublikasi DM Apik MedicinakadekapiklestariNo ratings yet
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientDocument12 pagesManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NNo ratings yet
- Diabetic Ketoacidosis in Toddler With A Diaper RashDocument4 pagesDiabetic Ketoacidosis in Toddler With A Diaper RashKarl Angelo MontanoNo ratings yet
- Insulin Secretion and FunctionDocument8 pagesInsulin Secretion and FunctionWendy EscalanteNo ratings yet
- Diabetes MellitusDocument32 pagesDiabetes Mellitusanfalalamin9915No ratings yet
- Hipertrigliseridemia in PregnancyDocument5 pagesHipertrigliseridemia in PregnancySparkling PinkNo ratings yet
- Edit Adih LaptopDocument6 pagesEdit Adih LaptopTry Ahmad MirzaNo ratings yet
- Hepatic Glycogenosis Associated With Type 1 Diabetes (A Case Report)Document5 pagesHepatic Glycogenosis Associated With Type 1 Diabetes (A Case Report)IJAR JOURNALNo ratings yet
- Dental Management of Patients With Diabetes MellitusDocument8 pagesDental Management of Patients With Diabetes Mellitusاحمد سلامNo ratings yet
- Management of Newly Diagnosed Type 2 DiabetesDocument24 pagesManagement of Newly Diagnosed Type 2 DiabetesZulhida YuniNo ratings yet
- Exenatide Response in An Adolescent's Morbid Obesity: Pharmacology & Pharmacy, 2014, 5, 419-424Document6 pagesExenatide Response in An Adolescent's Morbid Obesity: Pharmacology & Pharmacy, 2014, 5, 419-424CamiNo ratings yet
- Nutrisi Ulseratif KolitisDocument1 pageNutrisi Ulseratif KolitisFetria MelaniNo ratings yet
- Overt Diabetes: Diabetes Mellitus in PregnancyDocument3 pagesOvert Diabetes: Diabetes Mellitus in PregnancyBrian TiopengcoNo ratings yet
- Metformin For GDMDocument7 pagesMetformin For GDMRoro WidyastutiNo ratings yet
- 66 2 171 PDFDocument5 pages66 2 171 PDF2C Sabayo Julia Andre J.No ratings yet
- Case StudyDocument3 pagesCase StudyAnnie Laiza BacayNo ratings yet
- J Clin Endocrinol Metab. 2012 97 16 38Document23 pagesJ Clin Endocrinol Metab. 2012 97 16 38rizwan234No ratings yet
- Diabetes PregnancyDocument65 pagesDiabetes PregnancyJohn Christopher LucesNo ratings yet
- Jurnal DMDocument5 pagesJurnal DMratihparmadiniNo ratings yet
- Eksperimental Metabolic-SyndromeDocument4 pagesEksperimental Metabolic-SyndromePrajna AdityaraniNo ratings yet
- Pi Is 1054139 X 13003157Document6 pagesPi Is 1054139 X 13003157Pablo Andres Encina AbrigoNo ratings yet
- Type A Insulin Resistance Syndrome and HAIRDocument2 pagesType A Insulin Resistance Syndrome and HAIRLaura BryantNo ratings yet
- Seminar 5 - DM in PregnancyDocument19 pagesSeminar 5 - DM in PregnancyHakimah K. SuhaimiNo ratings yet
- Managing Hipertriglyceridemia in Daily PracticeDocument7 pagesManaging Hipertriglyceridemia in Daily PracticeFrillyDeyanaNo ratings yet
- A Case Report of Hyperosmolar Hyperglycemic StateDocument1 pageA Case Report of Hyperosmolar Hyperglycemic StateHareesh ChanderNo ratings yet
- Indikasi Insulin InfusionDocument7 pagesIndikasi Insulin InfusionnikeNo ratings yet
- NCP Diabetes Mellitus Prepregnancy GestationalDocument12 pagesNCP Diabetes Mellitus Prepregnancy GestationalRichson BacayNo ratings yet
- Cetoacidosis Diabética Normoglicémica en El Embarazo. Caso ClínicoDocument5 pagesCetoacidosis Diabética Normoglicémica en El Embarazo. Caso ClínicoLvis Zevallos MavricioNo ratings yet
- Presentation Metabolic SyndromeDocument56 pagesPresentation Metabolic SyndromeAbdulhakeem Tleimat100% (1)
- Hypo Guidelines BrochureDocument2 pagesHypo Guidelines BrochureNellie RamosNo ratings yet
- Diabetus Mellitus: Dr. Fawzi Radi F.R.C.O.GDocument19 pagesDiabetus Mellitus: Dr. Fawzi Radi F.R.C.O.GCrissLaraNo ratings yet
- SGD 3: CASE DIABETES: "A Sweet Way To Lose Weight": Guide QuestionsDocument5 pagesSGD 3: CASE DIABETES: "A Sweet Way To Lose Weight": Guide QuestionsKaren Kaye CordovaNo ratings yet
- HypoglycemiaDocument19 pagesHypoglycemiaJesus PadillaNo ratings yet
- Diabetes in PregnencyDocument51 pagesDiabetes in PregnencyMuneeb JanNo ratings yet
- Diabetes Intraoperative Management ArticleDocument5 pagesDiabetes Intraoperative Management ArticlenesredeNo ratings yet
- Diabetes in Palliative Care CompletedDocument4 pagesDiabetes in Palliative Care Completedaya PermatasariNo ratings yet
- Katarak DM RemajaDocument8 pagesKatarak DM RemajaHIstoryNo ratings yet
- Metabolic Evaluation of Young Women With Congenital Adrenal HyperplasiaDocument7 pagesMetabolic Evaluation of Young Women With Congenital Adrenal HyperplasiaOnysapto PramanaNo ratings yet
- Neonatal Hyperglycemia: RPA Newborn Care Protocol BookDocument3 pagesNeonatal Hyperglycemia: RPA Newborn Care Protocol BookAnggia NoverinaNo ratings yet
- PCOS HealingDocument36 pagesPCOS HealingKheyrne Danu100% (1)
- How To Lose Weight Fast in 3 Simple StepsDocument8 pagesHow To Lose Weight Fast in 3 Simple StepsVarinder SinghNo ratings yet
- NCM 116 NutritionDocument9 pagesNCM 116 Nutritionrommel magoNo ratings yet
- Dairy Science and TechnologyDocument83 pagesDairy Science and Technologyیاسمین ثریاNo ratings yet
- Test Bank For Contemporary Nutrition 8th Edition Gordon WardlawDocument20 pagesTest Bank For Contemporary Nutrition 8th Edition Gordon WardlawJustin Zeches100% (34)
- Red MeatDocument9 pagesRed Meatarka prava LahiriNo ratings yet
- 1983 Speth (Garnsey Bison Kill BOOK)Document255 pages1983 Speth (Garnsey Bison Kill BOOK)jdspethNo ratings yet
- Intensive Booklet-P1-Print 2017Document20 pagesIntensive Booklet-P1-Print 2017Teacher FláviaNo ratings yet
- 2000 Cal Meal Planning GuideDocument6 pages2000 Cal Meal Planning GuideKaren MouraNo ratings yet
- Formerly: Notre Dame Hospital and School of Midwifery: 2. Identify and Discuss The Function of Macro and Micro NutrientsDocument20 pagesFormerly: Notre Dame Hospital and School of Midwifery: 2. Identify and Discuss The Function of Macro and Micro NutrientsMhianne SarmientoNo ratings yet
- Callebaut - Champ KremDocument3 pagesCallebaut - Champ KremCristian VasilescuNo ratings yet
- Nutrition in The Critically Ill PatientDocument13 pagesNutrition in The Critically Ill PatientnainazahraNo ratings yet
- Lipid PDFDocument17 pagesLipid PDFAnonymous xt41ryNo ratings yet
- Animal Nutrition - YR 10 WEEKS 2 & 3Document108 pagesAnimal Nutrition - YR 10 WEEKS 2 & 3BrioNo ratings yet
- Why Barley Is Good For Following Illnesses....Document2 pagesWhy Barley Is Good For Following Illnesses....jayarninianNo ratings yet
- Imani-Lara Lansiquot Masterclass: Half Marathon Guide Shakes For DaysDocument70 pagesImani-Lara Lansiquot Masterclass: Half Marathon Guide Shakes For DaysArnav GautamNo ratings yet
- Fibromyalgia - Causative Factors & Possible SolutionsDocument12 pagesFibromyalgia - Causative Factors & Possible SolutionsChef-doctor JemichelNo ratings yet
- Clinical Influence of Triple Omega Fatty Acids (Omega-3, 6, 9)Document3 pagesClinical Influence of Triple Omega Fatty Acids (Omega-3, 6, 9)Hạnh NguyễnNo ratings yet
- Egyptian Sweet Pastry Dessert (Umm Ali) : Start Reacting TodayDocument1 pageEgyptian Sweet Pastry Dessert (Umm Ali) : Start Reacting TodaySike Silvia GunawanNo ratings yet
- Goat Soybean Velvewt Bean GrowthDocument12 pagesGoat Soybean Velvewt Bean Growthwynferd ssNo ratings yet
- Photosynthesis Revision NoteDocument20 pagesPhotosynthesis Revision NoteUsman Mukhtar AbbasiNo ratings yet
- The Tre en en StoryDocument26 pagesThe Tre en en StoryNishit Kotak100% (1)
- 1800 Calories Diabetic DietDocument4 pages1800 Calories Diabetic DietNaing ooNo ratings yet
- Nutritive Value of MeatDocument16 pagesNutritive Value of MeatPooja Sri V S BE FPPTNo ratings yet
- Chemistry Holiday Homework Project For CBSE: Dry Fruit AnalysisDocument37 pagesChemistry Holiday Homework Project For CBSE: Dry Fruit AnalysisEkasNo ratings yet
- Fat Burn ConceptDocument31 pagesFat Burn ConceptManoj100% (1)
- Brochure Calibra EmailDocument24 pagesBrochure Calibra Emaila99602No ratings yet