Download as pdf or txt
You might also like
- Hayssen Training ElectricalDocument17 pagesHayssen Training ElectricalRoberto SanchezNo ratings yet
- August 14 - Sequencig Using Signal WordsDocument3 pagesAugust 14 - Sequencig Using Signal Wordsshe88% (8)
- Primarchs DatasheetsDocument24 pagesPrimarchs DatasheetsJosiah Young1100% (5)
- GUELMAN - 02 - PTSD Y EPIGEN+ëTICADocument15 pagesGUELMAN - 02 - PTSD Y EPIGEN+ëTICAMaría Alejandra DamborskyNo ratings yet
- Brain Circuit Dysfunction in Post - Traumatic Stress Disorder: From Mouse To Man - Robert J. FensterDocument17 pagesBrain Circuit Dysfunction in Post - Traumatic Stress Disorder: From Mouse To Man - Robert J. FensterAlvaro Arboledas LoriteNo ratings yet
- Linking Molecules To Mood: New Insight Into The Biology of DepressionDocument16 pagesLinking Molecules To Mood: New Insight Into The Biology of Depressiondudul pudlianNo ratings yet
- Biophy Lang TuDocument8 pagesBiophy Lang TuMay PerezNo ratings yet
- Altered Metabotropic Glutamate Receptor 5 Markers in PTSD - Pnas.201701749Document6 pagesAltered Metabotropic Glutamate Receptor 5 Markers in PTSD - Pnas.201701749iqrjtpNo ratings yet
- 2018 Theranostic Pharmacology in PTSDDocument52 pages2018 Theranostic Pharmacology in PTSDDiego HormacheaNo ratings yet
- Case Study - PTSD Final PaperDocument29 pagesCase Study - PTSD Final PaperMay PerezNo ratings yet
- Behavioral Neurobiology of PTSDDocument274 pagesBehavioral Neurobiology of PTSDCarlos Hernan Castañeda Ruiz100% (1)
- Artigo Fisiopato DepressãoDocument21 pagesArtigo Fisiopato DepressãoJ VichhyNo ratings yet
- Metaanaliza Serotonin Transporter and Amygdala ActiovationDocument6 pagesMetaanaliza Serotonin Transporter and Amygdala ActiovationCellaNo ratings yet
- Sequential Fear Generalization and Network Connectivity in Trauma Exposed Humans With and Without PsychopathologyDocument9 pagesSequential Fear Generalization and Network Connectivity in Trauma Exposed Humans With and Without Psychopathologyheidarihamed4No ratings yet
- PTSD As A Health Issue in SocietyDocument8 pagesPTSD As A Health Issue in SocietyjohnmorriscryptoNo ratings yet
- Higher Cortisol Levels Following Exposur PDFDocument34 pagesHigher Cortisol Levels Following Exposur PDFIván CornuNo ratings yet
- Literature Review On PTSDDocument4 pagesLiterature Review On PTSDozbvtcvkg100% (1)
- Brain, Behavior, and Immunity: Thaddeus W.W. Pace, Christine M. HeimDocument8 pagesBrain, Behavior, and Immunity: Thaddeus W.W. Pace, Christine M. HeimmarielaNo ratings yet
- Accepted Manuscript: Une Adrian J. BradleyDocument63 pagesAccepted Manuscript: Une Adrian J. BradleyJuliana MejiaNo ratings yet
- Rachel Yehuda Cortisol PTSD Policía BomberosDocument14 pagesRachel Yehuda Cortisol PTSD Policía BomberosPaulo GermanottaNo ratings yet
- Otto 2004Document10 pagesOtto 2004Nurul Muqarribah Pratiwi IshaqNo ratings yet
- The Neurobiology and Pharmacotherapy of Posttraumatic Stress PDFDocument21 pagesThe Neurobiology and Pharmacotherapy of Posttraumatic Stress PDFUSM San IgnacioNo ratings yet
- TEP y Psicosis 2019 OjoDocument11 pagesTEP y Psicosis 2019 OjosiralkNo ratings yet
- Fnins 15 678548Document14 pagesFnins 15 678548VickeyNo ratings yet
- NPP 2013327Document9 pagesNPP 2013327Egy Sunanda PutraNo ratings yet
- Literature Review Post Traumatic Stress DisorderDocument7 pagesLiterature Review Post Traumatic Stress Disorderc5r08vf7100% (1)
- Progress in Neuro-Psychopharmacology & Biological PsychiatryDocument5 pagesProgress in Neuro-Psychopharmacology & Biological PsychiatryHamil5No ratings yet
- Torres-Reading On PTSDDocument15 pagesTorres-Reading On PTSDbabiNo ratings yet
- GenticsreviewdepressionDocument9 pagesGenticsreviewdepressionapi-188978784No ratings yet
- The Evolutionary Significance of Depression in Pathogen Host Defense (PATHOS-D)Document23 pagesThe Evolutionary Significance of Depression in Pathogen Host Defense (PATHOS-D)Angel Ruben Maldonado GarciaNo ratings yet
- Animal Models of Suicide-Trait-Related BehaviorsDocument9 pagesAnimal Models of Suicide-Trait-Related BehaviorsDoina AlbescuNo ratings yet
- Letters To The Editor: Trichotillomania and Bipolar DisorderDocument1 pageLetters To The Editor: Trichotillomania and Bipolar Disordermohamad safiiNo ratings yet
- Diferencias de GeneroDocument11 pagesDiferencias de GeneroIvan GabrielNo ratings yet
- Tsai1999 SerotoninDocument3 pagesTsai1999 SerotoninFitri anaNo ratings yet
- Nemeroff Heim PTSDDocument12 pagesNemeroff Heim PTSDmariela100% (1)
- Journal Pre-Proof: Biological Psychiatry: Cognitive Neuroscience and NeuroimagingDocument32 pagesJournal Pre-Proof: Biological Psychiatry: Cognitive Neuroscience and NeuroimagingPradeep DeNo ratings yet
- Posttraumatic Psychopathology and The Pace of The Epigenetic Clock: A Longitudinal InvestigationDocument14 pagesPosttraumatic Psychopathology and The Pace of The Epigenetic Clock: A Longitudinal InvestigationzainNo ratings yet
- Schmitt2014 - MozartDocument3 pagesSchmitt2014 - MozartArif Erdem KöroğluNo ratings yet
- Summary and General DiscussionDocument14 pagesSummary and General DiscussionAli ElHadi MarmarNo ratings yet
- Literature Review of PTSDDocument4 pagesLiterature Review of PTSDfvhj1y00100% (1)
- MainDocument8 pagesMainajNo ratings yet
- Comentario PSDDocument8 pagesComentario PSDImja94No ratings yet
- Biological Psychology: ArticleinfoDocument15 pagesBiological Psychology: ArticleinfoManuela SilvaNo ratings yet
- DNB 29 4 407 20 Hus PDFDocument14 pagesDNB 29 4 407 20 Hus PDFthedi28No ratings yet
- Openness To Experience SiswaDocument15 pagesOpenness To Experience Siswariski agustianNo ratings yet
- Prazosin TX PTSDMetaanalysis 2020Document8 pagesPrazosin TX PTSDMetaanalysis 2020Dr. José Juan PeralesNo ratings yet
- Appi Ajp 2010 10040541Document9 pagesAppi Ajp 2010 10040541FebniNo ratings yet
- Statistical Research Proposal - EditedDocument6 pagesStatistical Research Proposal - EditedSirena WritersNo ratings yet
- Allelic Variation in 5-HT Receptor Expression Is Associated With Anxiety-And Depression-Related Personality TraitsDocument9 pagesAllelic Variation in 5-HT Receptor Expression Is Associated With Anxiety-And Depression-Related Personality TraitsTânia SilvaNo ratings yet
- Meta-Analysis of FKBP5 Gene Polymorphisms Association WithDocument6 pagesMeta-Analysis of FKBP5 Gene Polymorphisms Association WithamirNo ratings yet
- Posttraumatic Stress Disorder and Adherence To Medications in Survivors of Strokes and Transient Ischemic AttacksDocument7 pagesPosttraumatic Stress Disorder and Adherence To Medications in Survivors of Strokes and Transient Ischemic AttacksNicky Adi SaputraNo ratings yet
- Posttraumatic Stress Disorder and Depression Following Trauma: Understanding ComorbidityDocument7 pagesPosttraumatic Stress Disorder and Depression Following Trauma: Understanding ComorbiditySharon AdeleNo ratings yet
- Personality Traits According To HormonesDocument23 pagesPersonality Traits According To HormonesTakudzwa Raphael MuzaNo ratings yet
- Schizophrenia Research: Rebecca Rodrigues, Kelly K. AndersonDocument10 pagesSchizophrenia Research: Rebecca Rodrigues, Kelly K. Andersonsamira6alvarado6zebaNo ratings yet
- DialoguesClinNeurosci 21 417Document12 pagesDialoguesClinNeurosci 21 417VickeyNo ratings yet
- 102 FullDocument10 pages102 FullBney MaharjanNo ratings yet
- Epigenetic Biomarkers As Predictors and Correlates of Symptom Improvement Following Psychotherapy in Combat Veterans With PTSDDocument14 pagesEpigenetic Biomarkers As Predictors and Correlates of Symptom Improvement Following Psychotherapy in Combat Veterans With PTSDmarielaNo ratings yet
- Brenner 2018Document6 pagesBrenner 2018Yeray GranadoNo ratings yet
- M - P I - 6 L P D D: ETA Analysis of Lasma Nterleukine Evels in Atients With Epressive IsorderDocument5 pagesM - P I - 6 L P D D: ETA Analysis of Lasma Nterleukine Evels in Atients With Epressive IsorderMakkai Popa Mihai VladimirNo ratings yet
- Neuropharmacology: Hagit Cohen, Nitsan Kozlovsky, Cramer Alona, Michael A. Matar, Zohar JosephDocument10 pagesNeuropharmacology: Hagit Cohen, Nitsan Kozlovsky, Cramer Alona, Michael A. Matar, Zohar JosephDoina AlbescuNo ratings yet
- tmp33F4 TMPDocument7 pagestmp33F4 TMPFrontiersNo ratings yet
- Science SignalingDocument7 pagesScience SignalingSharon AdeleNo ratings yet
- Use of Cannabis in the Treatment of Post-Traumatic Stress DisorderFrom EverandUse of Cannabis in the Treatment of Post-Traumatic Stress DisorderNo ratings yet
- Marketing Channels and Supply Chain ManagementDocument28 pagesMarketing Channels and Supply Chain ManagementGangadhar MamadapurNo ratings yet
- EScan Corporate 360 UGDocument601 pagesEScan Corporate 360 UG11F10 RUCHITA MAARANNo ratings yet
- Itch Mechanisms and ManagementDocument464 pagesItch Mechanisms and ManagementGaurav JaswalNo ratings yet
- Turbine Gas G.T.G. 1Document17 pagesTurbine Gas G.T.G. 1wilsonNo ratings yet
- Analytical Chem Chap11Document18 pagesAnalytical Chem Chap11Nicole Ann PedriñaNo ratings yet
- ATS3445 Tutorial 1 2023Document16 pagesATS3445 Tutorial 1 2023april ngNo ratings yet
- Top 40 C Programming Interview Questions and AnswersDocument8 pagesTop 40 C Programming Interview Questions and Answersasanga_indrajithNo ratings yet
- E Statement 20221120Document4 pagesE Statement 20221120Nik HafizNo ratings yet
- Stamens PDFDocument10 pagesStamens PDFAmeya KannamwarNo ratings yet
- Fragment D Une Statue D Osiris ConsacreDocument11 pagesFragment D Une Statue D Osiris ConsacrePedro Hernández PostelNo ratings yet
- A Practical Grammar of The Sanskrit LanguageDocument408 pagesA Practical Grammar of The Sanskrit LanguageungulataNo ratings yet
- Michael & Co. vs. Enriquez (33 Phil 87 (1915)Document3 pagesMichael & Co. vs. Enriquez (33 Phil 87 (1915)Analyn Grace Yongco BasayNo ratings yet
- Coast Artillery Journal - Oct 1946Document84 pagesCoast Artillery Journal - Oct 1946CAP History LibraryNo ratings yet
- MODBUS TCP/IP (0x/1x Range Adjustable) : HMI SettingDocument5 pagesMODBUS TCP/IP (0x/1x Range Adjustable) : HMI SettingÁnh VũNo ratings yet
- ESD122 2-Channel ESD Protection Diode For USB Type-C and HDMI 2.0Document27 pagesESD122 2-Channel ESD Protection Diode For USB Type-C and HDMI 2.0H tavangarNo ratings yet
- Rational Expressions WorksheetDocument4 pagesRational Expressions WorksheetSishira PattanNo ratings yet
- PDF Sermon Notes - The Temptation of Christ (Luke 4.1-13)Document5 pagesPDF Sermon Notes - The Temptation of Christ (Luke 4.1-13)fergie45315No ratings yet
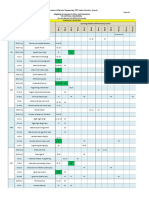
- Mapping PEC 2021-Oct-20 Annex-D Courses Vs PLO Vs TaxonomyDocument2 pagesMapping PEC 2021-Oct-20 Annex-D Courses Vs PLO Vs TaxonomyEngr.Mohsin ShaikhNo ratings yet
- 02TP PrelimExam MITDocument2 pages02TP PrelimExam MITSnapShop by AJNo ratings yet
- Dictionary of Mission Theology, History, Perspectives Müller, KarlDocument552 pagesDictionary of Mission Theology, History, Perspectives Müller, KarlRev. Johana VangchhiaNo ratings yet
- Grade 6 Worksheet DypisDocument2 pagesGrade 6 Worksheet DypisPehel MehtaNo ratings yet
- Friction Worksheet: Part A Questions - Multiple ChoiceDocument2 pagesFriction Worksheet: Part A Questions - Multiple ChoiceAmos JosephatNo ratings yet
- Module 6 - Sequential Circuits, Excitation Function, State Table, State DiagramDocument21 pagesModule 6 - Sequential Circuits, Excitation Function, State Table, State DiagramYvanne Esquia CuregNo ratings yet
- Foreign Body Airway ObstructionDocument16 pagesForeign Body Airway ObstructionKatNo ratings yet
- 1 IntroductionDocument28 pages1 Introductionkevnnicl921216No ratings yet
- Working With MongoDB - 518Document11 pagesWorking With MongoDB - 518Sivaraman AlagappanNo ratings yet
- Gr11 Mock Exam Schedule 2024Document13 pagesGr11 Mock Exam Schedule 2024potrillo0330No ratings yet