
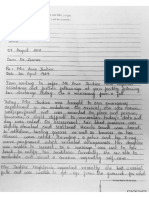
Medicine Cupboard Keys Part B
Medicine Cupboard Keys Part B
You might also like
- Multiple Choice Questions in Paediatric SurgeryFrom EverandMultiple Choice Questions in Paediatric SurgeryRating: 1 out of 5 stars1/5 (1)
- Medical Surgical Nursing Clinical Management For Positive Outcomes Single Volume 8th Edition Black Test BankDocument36 pagesMedical Surgical Nursing Clinical Management For Positive Outcomes Single Volume 8th Edition Black Test Bankpremiseembrightac0ntd100% (32)
- Reading Sub-Test: Part ADocument17 pagesReading Sub-Test: Part AVijayalakshmi Narayanaswami78% (9)
- Test Bank For Clinical Manifestations and Assessment of Respiratory Disease 7th Edition by Des JardinsDocument3 pagesTest Bank For Clinical Manifestations and Assessment of Respiratory Disease 7th Edition by Des Jardinsnoumenalskall0wewNo ratings yet
- Patient Confidentiality Part BDocument6 pagesPatient Confidentiality Part BSojiNo ratings yet
- Rodak Questions CompilationDocument40 pagesRodak Questions CompilationGertrudeshane IletoNo ratings yet
- Chapter 10: Parenteral Administration: Safe Preparation of Parenteral Medications Test BankDocument6 pagesChapter 10: Parenteral Administration: Safe Preparation of Parenteral Medications Test BankLuna TunaNo ratings yet
- MCQ AnsDocument65 pagesMCQ AnsFatima Hasnain100% (7)
- Iilt File 13Document23 pagesIilt File 13Rosmin AnsuNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Compre - NP 3 Ans. KeyDocument13 pagesCompre - NP 3 Ans. KeyJune Dumdumaya100% (2)
- Reading Sub-Test - Question Paper: Parts B & CDocument16 pagesReading Sub-Test - Question Paper: Parts B & CShyju Paul100% (2)
- Nursing Board Exam Review Questions in Emergency Part 6Document3 pagesNursing Board Exam Review Questions in Emergency Part 6Kristine Nagasan50% (2)
- Reading-Sample-Test-2-Question-Paper-Part-BCDocument16 pagesReading-Sample-Test-2-Question-Paper-Part-BCRithu SanthoshNo ratings yet
- Reading Sample Test 2 Question Paper Part BCDocument16 pagesReading Sample Test 2 Question Paper Part BCSusan HsiaoNo ratings yet
- Wa0010.Document9 pagesWa0010.SojiNo ratings yet
- PPP Reading Test 7 Parts BC Question PaperDocument16 pagesPPP Reading Test 7 Parts BC Question PaperhaffizmoradNo ratings yet
- Reading Sample Test 1 Question Paper Part BCDocument14 pagesReading Sample Test 1 Question Paper Part BCvidyaNo ratings yet
- Reading Test 4 - Paracetamol OverdoseDocument7 pagesReading Test 4 - Paracetamol OverdoseOlive Group0% (1)
- Practice Test 2 Reading Part BDocument5 pagesPractice Test 2 Reading Part BkholiooNo ratings yet
- Reading Sample Test 5 - Reading Part BC Question PaperDocument16 pagesReading Sample Test 5 - Reading Part BC Question PaperNanda NandaNo ratings yet
- HHHHHHDocument16 pagesHHHHHHiffat hanifNo ratings yet
- Columban College Finals Fundamentals of NursingDocument22 pagesColumban College Finals Fundamentals of NursingMatelyn OargaNo ratings yet
- Chapter 38 NS1030 Sue Study GuideDocument19 pagesChapter 38 NS1030 Sue Study GuideLuke Rachel WurzNo ratings yet
- Manual On Surgery Part BDocument6 pagesManual On Surgery Part BSojiNo ratings yet
- Chapter 13: Support Surfaces and Special Beds Perry Et Al.: Clinical Nursing Skills & Techniques, 9th Edition Multiple ChoiceDocument11 pagesChapter 13: Support Surfaces and Special Beds Perry Et Al.: Clinical Nursing Skills & Techniques, 9th Edition Multiple ChoiceComfort YaaNo ratings yet
- Finshed Profread Preboard NCM1Document29 pagesFinshed Profread Preboard NCM1imyutheyu07No ratings yet
- Board Exam Compilation Book 2 SampleDocument11 pagesBoard Exam Compilation Book 2 SampleElizabella Henrietta TanaquilNo ratings yet
- NPT 3Document8 pagesNPT 3chrizthineeNo ratings yet
- Chapter 038Document19 pagesChapter 038dtheart2821100% (2)
- Full Download PDF of Test Bank For Clinical Manifestations and Assessment of Respiratory Disease 7th Edition by Des Jardins All ChapterDocument14 pagesFull Download PDF of Test Bank For Clinical Manifestations and Assessment of Respiratory Disease 7th Edition by Des Jardins All Chaptercaxakawita100% (4)
- Occupational English Test Oet Reading Part BC Test 04Document16 pagesOccupational English Test Oet Reading Part BC Test 04AndreaNo ratings yet
- Board Exam Compilation Book 2 SampleDocument10 pagesBoard Exam Compilation Book 2 SampleebookwholesellerNo ratings yet
- Reading Sample Test 1 Question Paper Part BCDocument16 pagesReading Sample Test 1 Question Paper Part BCpratim deyNo ratings yet
- Post Test 2 RationalesDocument11 pagesPost Test 2 Rationalesrhymes2u100% (2)
- Reading Sample Test 1 Question Paper Part BCDocument16 pagesReading Sample Test 1 Question Paper Part BCAnat Rose TomNo ratings yet
- 6 ETS VenipunctureDocument7 pages6 ETS VenipunctureMyedelle SeacorNo ratings yet
- Office of The Infection Control Committee: Allied Care Experts (Ace) Medical Center - PaterosDocument5 pagesOffice of The Infection Control Committee: Allied Care Experts (Ace) Medical Center - PaterosCris GalendezNo ratings yet
- NP3 SET A With AnswersDocument11 pagesNP3 SET A With AnswersMiss GNo ratings yet
- ReadingTest Question Paper Part B CDocument16 pagesReadingTest Question Paper Part B CkholiooNo ratings yet
- Manila Adventist College: REFERENCE For Your Answers. Best If You Will Use Your Book ReferenceDocument13 pagesManila Adventist College: REFERENCE For Your Answers. Best If You Will Use Your Book ReferenceAb Staholic BoiiNo ratings yet
- Suctioning Procedure ChecklistDocument3 pagesSuctioning Procedure Checklistzulycajamalul1No ratings yet
- Wa0011.Document10 pagesWa0011.SojiNo ratings yet
- Full Download Essentials of Psychiatric Mental Health Nursing 3rd Edition Varcarolis Test Bank PDF Full ChapterDocument36 pagesFull Download Essentials of Psychiatric Mental Health Nursing 3rd Edition Varcarolis Test Bank PDF Full Chapterdiodontmetacism.0jw2al100% (20)
- PerioperativeDocument37 pagesPerioperativemj CanilangNo ratings yet
- RodakQuestions ComDocument46 pagesRodakQuestions ComMJ ArboledaNo ratings yet
- Full Download Pharmacology A Nursing Process Approach 7th Edition Kee Test BankDocument35 pagesFull Download Pharmacology A Nursing Process Approach 7th Edition Kee Test Bankc3miabutler100% (39)
- Sample Test 4 PtBC Question PaperDocument16 pagesSample Test 4 PtBC Question PaperRithu SanthoshNo ratings yet
- RENR 200 Items Comprehensive TestDocument35 pagesRENR 200 Items Comprehensive TestForevera QueenNo ratings yet
- Preboard Exam NP 4 MsDocument20 pagesPreboard Exam NP 4 MsDavid Lopez50% (2)
- UntitledDocument2 pagesUntitledgovindchoudhary1995aug22No ratings yet
- Board Exam Compilation Book 2Document163 pagesBoard Exam Compilation Book 2Aaron Cy Untalan100% (6)
- NLE Reviewer (June 2008) NP1Document25 pagesNLE Reviewer (June 2008) NP1Honey BiteNo ratings yet
- Nursing Practice 3 (Dec 2006)Document11 pagesNursing Practice 3 (Dec 2006)ɹǝʍdןnosNo ratings yet
- MOCK Read BC PDFDocument16 pagesMOCK Read BC PDFfaysal83% (6)
- Digestive System 2Document32 pagesDigestive System 2Johnmer AvelinoNo ratings yet
- Ms 1 PerioperativeDocument41 pagesMs 1 PerioperativeSheana TmplNo ratings yet
- Fundamentals of Nursing QuestionsDocument74 pagesFundamentals of Nursing QuestionsVin Lorenzo CampbellNo ratings yet
- OET 2 Reading Test 10 Part BDocument4 pagesOET 2 Reading Test 10 Part BAlice ChirilaNo ratings yet
- Snippets in Surgery Vol 1: Illustrated Essentials of General SurgeryFrom EverandSnippets in Surgery Vol 1: Illustrated Essentials of General SurgeryRating: 5 out of 5 stars5/5 (1)
- Infection Control For Dental Pract. Part BDocument6 pagesInfection Control For Dental Pract. Part BSoji100% (1)
- Wa0009.Document11 pagesWa0009.SojiNo ratings yet
- Malaria Part ADocument6 pagesMalaria Part ASoji100% (1)
- Mr. Malcolm WhittakerDocument2 pagesMr. Malcolm WhittakerSoji100% (1)
- Wa0038.Document11 pagesWa0038.SojiNo ratings yet
- Pneumothorax Part ADocument4 pagesPneumothorax Part ASoji0% (1)
- Warm Up Questions For NursesDocument13 pagesWarm Up Questions For NursesSoji100% (1)
- Basam Metabolic Rate Part ADocument5 pagesBasam Metabolic Rate Part ASojiNo ratings yet
- FB Img 1694087555722Document59 pagesFB Img 1694087555722SojiNo ratings yet
- Mr. Robert ScottDocument2 pagesMr. Robert ScottSojiNo ratings yet
- Mr. George PalostiveDocument2 pagesMr. George PalostiveSojiNo ratings yet
- Img 20230825 001955Document2 pagesImg 20230825 001955SojiNo ratings yet
- VN - Technical Officer (Measles) - (2307909)Document2 pagesVN - Technical Officer (Measles) - (2307909)SojiNo ratings yet
- Writing 101 2Document2 pagesWriting 101 2Soji0% (1)
- Mr. Janet HardyDocument2 pagesMr. Janet HardySoji100% (1)
- Ms Anne JenkinsDocument2 pagesMs Anne JenkinsSojiNo ratings yet
- Cardiac Outflow Tract TableDocument3 pagesCardiac Outflow Tract TableCathyCluverNo ratings yet
- HEALTH CARE DELIVERY SYSTEM Lesson PlanDocument22 pagesHEALTH CARE DELIVERY SYSTEM Lesson PlanJosephin dayanaNo ratings yet
- Personalized AyurvedDocument13 pagesPersonalized AyurvedAtul WaghNo ratings yet
- Janumet PM eDocument62 pagesJanumet PM eRaffi DerderianNo ratings yet
- SPIRITUALITYDocument4 pagesSPIRITUALITYAnne Arboleda100% (1)
- SPM TRIAL 2007 English Paper 2Document19 pagesSPM TRIAL 2007 English Paper 2Raymond Cheang Chee-CheongNo ratings yet
- Eng Kafo PDFDocument20 pagesEng Kafo PDFRaden Achmad Candra PutraNo ratings yet
- Kalamata Programma FinalDocument26 pagesKalamata Programma FinalkalamatasummercampNo ratings yet
- Paediatric Drug Chart CalculatorDocument3 pagesPaediatric Drug Chart CalculatorgregraynerNo ratings yet
- Mukta Sharma ReportDocument2 pagesMukta Sharma ReportARUN SHANKARNo ratings yet
- Quality Control of Sterile ProductsDocument21 pagesQuality Control of Sterile Productskunasahu1100% (3)
- PBL GuideDocument30 pagesPBL GuideNur Afiqa AzalanNo ratings yet
- Why Am I So Sick - Traditional Medical AstrologyDocument3 pagesWhy Am I So Sick - Traditional Medical AstrologyKevin RiceNo ratings yet
- Baroudi Seroma - How To Avoid It and How To Treat ItDocument3 pagesBaroudi Seroma - How To Avoid It and How To Treat ItLuisCRNo ratings yet
- Post DeliveryDocument26 pagesPost DeliverySaid Said (ابو خالد)No ratings yet
- FORMULARIUM Kasih Karunia 2021Document32 pagesFORMULARIUM Kasih Karunia 2021dwirahma slNo ratings yet
- Health Care Delivery System FinalDocument14 pagesHealth Care Delivery System FinalAkhosh Somarajan79% (14)
- Continued Growth Hormone GH Treatment ADocument5 pagesContinued Growth Hormone GH Treatment AAnghel Ana-MariaNo ratings yet
- Tugas Bhs. Inggris: Nama: Muhamad Wahyu S. Kelas: Xiipa2 NO.: 19Document4 pagesTugas Bhs. Inggris: Nama: Muhamad Wahyu S. Kelas: Xiipa2 NO.: 19Wahyu SetyobudiNo ratings yet
- Broncho DilatorsDocument53 pagesBroncho DilatorsDocRNNo ratings yet
- Open Letter To NJSDDocument4 pagesOpen Letter To NJSDWBAYNo ratings yet
- IMNCI Chart Booklet (New) OrignalDocument36 pagesIMNCI Chart Booklet (New) OrignaleresdNo ratings yet
- Shimadzu Radspeed MC Radspeed M BrochureDocument5 pagesShimadzu Radspeed MC Radspeed M BrochureMuhammad Areeb100% (1)
- Drug PresentationDocument9 pagesDrug PresentationAddah, Dhenaraiza H.No ratings yet
- HIV and Islam Is HIV Prevalence Lower Am PDFDocument6 pagesHIV and Islam Is HIV Prevalence Lower Am PDFPriyo DjatmikoNo ratings yet
- 1st Round CounsellngDocument112 pages1st Round CounsellngRavi SinghNo ratings yet
- Mechanical Ventilation of Adults in The Emergency Department - UpToDateDocument28 pagesMechanical Ventilation of Adults in The Emergency Department - UpToDateCarlos E. Morales AyoraNo ratings yet
- WISC IV Cross Culture ComparisonDocument21 pagesWISC IV Cross Culture ComparisongwzglNo ratings yet
- Reabilitare Dupa AvcDocument91 pagesReabilitare Dupa AvcDiana StancaNo ratings yet



































































































Download as pdf or txt
You might also like
- Multiple Choice Questions in Paediatric SurgeryFrom EverandMultiple Choice Questions in Paediatric SurgeryRating: 1 out of 5 stars1/5 (1)
- Medical Surgical Nursing Clinical Management For Positive Outcomes Single Volume 8th Edition Black Test BankDocument36 pagesMedical Surgical Nursing Clinical Management For Positive Outcomes Single Volume 8th Edition Black Test Bankpremiseembrightac0ntd100% (32)
- Reading Sub-Test: Part ADocument17 pagesReading Sub-Test: Part AVijayalakshmi Narayanaswami78% (9)
- Test Bank For Clinical Manifestations and Assessment of Respiratory Disease 7th Edition by Des JardinsDocument3 pagesTest Bank For Clinical Manifestations and Assessment of Respiratory Disease 7th Edition by Des Jardinsnoumenalskall0wewNo ratings yet
- Patient Confidentiality Part BDocument6 pagesPatient Confidentiality Part BSojiNo ratings yet
- Rodak Questions CompilationDocument40 pagesRodak Questions CompilationGertrudeshane IletoNo ratings yet
- Chapter 10: Parenteral Administration: Safe Preparation of Parenteral Medications Test BankDocument6 pagesChapter 10: Parenteral Administration: Safe Preparation of Parenteral Medications Test BankLuna TunaNo ratings yet
- MCQ AnsDocument65 pagesMCQ AnsFatima Hasnain100% (7)
- Iilt File 13Document23 pagesIilt File 13Rosmin AnsuNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Compre - NP 3 Ans. KeyDocument13 pagesCompre - NP 3 Ans. KeyJune Dumdumaya100% (2)
- Reading Sub-Test - Question Paper: Parts B & CDocument16 pagesReading Sub-Test - Question Paper: Parts B & CShyju Paul100% (2)
- Nursing Board Exam Review Questions in Emergency Part 6Document3 pagesNursing Board Exam Review Questions in Emergency Part 6Kristine Nagasan50% (2)
- Reading-Sample-Test-2-Question-Paper-Part-BCDocument16 pagesReading-Sample-Test-2-Question-Paper-Part-BCRithu SanthoshNo ratings yet
- Reading Sample Test 2 Question Paper Part BCDocument16 pagesReading Sample Test 2 Question Paper Part BCSusan HsiaoNo ratings yet
- Wa0010.Document9 pagesWa0010.SojiNo ratings yet
- PPP Reading Test 7 Parts BC Question PaperDocument16 pagesPPP Reading Test 7 Parts BC Question PaperhaffizmoradNo ratings yet
- Reading Sample Test 1 Question Paper Part BCDocument14 pagesReading Sample Test 1 Question Paper Part BCvidyaNo ratings yet
- Reading Test 4 - Paracetamol OverdoseDocument7 pagesReading Test 4 - Paracetamol OverdoseOlive Group0% (1)
- Practice Test 2 Reading Part BDocument5 pagesPractice Test 2 Reading Part BkholiooNo ratings yet
- Reading Sample Test 5 - Reading Part BC Question PaperDocument16 pagesReading Sample Test 5 - Reading Part BC Question PaperNanda NandaNo ratings yet
- HHHHHHDocument16 pagesHHHHHHiffat hanifNo ratings yet
- Columban College Finals Fundamentals of NursingDocument22 pagesColumban College Finals Fundamentals of NursingMatelyn OargaNo ratings yet
- Chapter 38 NS1030 Sue Study GuideDocument19 pagesChapter 38 NS1030 Sue Study GuideLuke Rachel WurzNo ratings yet
- Manual On Surgery Part BDocument6 pagesManual On Surgery Part BSojiNo ratings yet
- Chapter 13: Support Surfaces and Special Beds Perry Et Al.: Clinical Nursing Skills & Techniques, 9th Edition Multiple ChoiceDocument11 pagesChapter 13: Support Surfaces and Special Beds Perry Et Al.: Clinical Nursing Skills & Techniques, 9th Edition Multiple ChoiceComfort YaaNo ratings yet
- Finshed Profread Preboard NCM1Document29 pagesFinshed Profread Preboard NCM1imyutheyu07No ratings yet
- Board Exam Compilation Book 2 SampleDocument11 pagesBoard Exam Compilation Book 2 SampleElizabella Henrietta TanaquilNo ratings yet
- NPT 3Document8 pagesNPT 3chrizthineeNo ratings yet
- Chapter 038Document19 pagesChapter 038dtheart2821100% (2)
- Full Download PDF of Test Bank For Clinical Manifestations and Assessment of Respiratory Disease 7th Edition by Des Jardins All ChapterDocument14 pagesFull Download PDF of Test Bank For Clinical Manifestations and Assessment of Respiratory Disease 7th Edition by Des Jardins All Chaptercaxakawita100% (4)
- Occupational English Test Oet Reading Part BC Test 04Document16 pagesOccupational English Test Oet Reading Part BC Test 04AndreaNo ratings yet
- Board Exam Compilation Book 2 SampleDocument10 pagesBoard Exam Compilation Book 2 SampleebookwholesellerNo ratings yet
- Reading Sample Test 1 Question Paper Part BCDocument16 pagesReading Sample Test 1 Question Paper Part BCpratim deyNo ratings yet
- Post Test 2 RationalesDocument11 pagesPost Test 2 Rationalesrhymes2u100% (2)
- Reading Sample Test 1 Question Paper Part BCDocument16 pagesReading Sample Test 1 Question Paper Part BCAnat Rose TomNo ratings yet
- 6 ETS VenipunctureDocument7 pages6 ETS VenipunctureMyedelle SeacorNo ratings yet
- Office of The Infection Control Committee: Allied Care Experts (Ace) Medical Center - PaterosDocument5 pagesOffice of The Infection Control Committee: Allied Care Experts (Ace) Medical Center - PaterosCris GalendezNo ratings yet
- NP3 SET A With AnswersDocument11 pagesNP3 SET A With AnswersMiss GNo ratings yet
- ReadingTest Question Paper Part B CDocument16 pagesReadingTest Question Paper Part B CkholiooNo ratings yet
- Manila Adventist College: REFERENCE For Your Answers. Best If You Will Use Your Book ReferenceDocument13 pagesManila Adventist College: REFERENCE For Your Answers. Best If You Will Use Your Book ReferenceAb Staholic BoiiNo ratings yet
- Suctioning Procedure ChecklistDocument3 pagesSuctioning Procedure Checklistzulycajamalul1No ratings yet
- Wa0011.Document10 pagesWa0011.SojiNo ratings yet
- Full Download Essentials of Psychiatric Mental Health Nursing 3rd Edition Varcarolis Test Bank PDF Full ChapterDocument36 pagesFull Download Essentials of Psychiatric Mental Health Nursing 3rd Edition Varcarolis Test Bank PDF Full Chapterdiodontmetacism.0jw2al100% (20)
- PerioperativeDocument37 pagesPerioperativemj CanilangNo ratings yet
- RodakQuestions ComDocument46 pagesRodakQuestions ComMJ ArboledaNo ratings yet
- Full Download Pharmacology A Nursing Process Approach 7th Edition Kee Test BankDocument35 pagesFull Download Pharmacology A Nursing Process Approach 7th Edition Kee Test Bankc3miabutler100% (39)
- Sample Test 4 PtBC Question PaperDocument16 pagesSample Test 4 PtBC Question PaperRithu SanthoshNo ratings yet
- RENR 200 Items Comprehensive TestDocument35 pagesRENR 200 Items Comprehensive TestForevera QueenNo ratings yet
- Preboard Exam NP 4 MsDocument20 pagesPreboard Exam NP 4 MsDavid Lopez50% (2)
- UntitledDocument2 pagesUntitledgovindchoudhary1995aug22No ratings yet
- Board Exam Compilation Book 2Document163 pagesBoard Exam Compilation Book 2Aaron Cy Untalan100% (6)
- NLE Reviewer (June 2008) NP1Document25 pagesNLE Reviewer (June 2008) NP1Honey BiteNo ratings yet
- Nursing Practice 3 (Dec 2006)Document11 pagesNursing Practice 3 (Dec 2006)ɹǝʍdןnosNo ratings yet
- MOCK Read BC PDFDocument16 pagesMOCK Read BC PDFfaysal83% (6)
- Digestive System 2Document32 pagesDigestive System 2Johnmer AvelinoNo ratings yet
- Ms 1 PerioperativeDocument41 pagesMs 1 PerioperativeSheana TmplNo ratings yet
- Fundamentals of Nursing QuestionsDocument74 pagesFundamentals of Nursing QuestionsVin Lorenzo CampbellNo ratings yet
- OET 2 Reading Test 10 Part BDocument4 pagesOET 2 Reading Test 10 Part BAlice ChirilaNo ratings yet
- Snippets in Surgery Vol 1: Illustrated Essentials of General SurgeryFrom EverandSnippets in Surgery Vol 1: Illustrated Essentials of General SurgeryRating: 5 out of 5 stars5/5 (1)
- Infection Control For Dental Pract. Part BDocument6 pagesInfection Control For Dental Pract. Part BSoji100% (1)
- Wa0009.Document11 pagesWa0009.SojiNo ratings yet
- Malaria Part ADocument6 pagesMalaria Part ASoji100% (1)
- Mr. Malcolm WhittakerDocument2 pagesMr. Malcolm WhittakerSoji100% (1)
- Wa0038.Document11 pagesWa0038.SojiNo ratings yet
- Pneumothorax Part ADocument4 pagesPneumothorax Part ASoji0% (1)
- Warm Up Questions For NursesDocument13 pagesWarm Up Questions For NursesSoji100% (1)
- Basam Metabolic Rate Part ADocument5 pagesBasam Metabolic Rate Part ASojiNo ratings yet
- FB Img 1694087555722Document59 pagesFB Img 1694087555722SojiNo ratings yet
- Mr. Robert ScottDocument2 pagesMr. Robert ScottSojiNo ratings yet
- Mr. George PalostiveDocument2 pagesMr. George PalostiveSojiNo ratings yet
- Img 20230825 001955Document2 pagesImg 20230825 001955SojiNo ratings yet
- VN - Technical Officer (Measles) - (2307909)Document2 pagesVN - Technical Officer (Measles) - (2307909)SojiNo ratings yet
- Writing 101 2Document2 pagesWriting 101 2Soji0% (1)
- Mr. Janet HardyDocument2 pagesMr. Janet HardySoji100% (1)
- Ms Anne JenkinsDocument2 pagesMs Anne JenkinsSojiNo ratings yet
- Cardiac Outflow Tract TableDocument3 pagesCardiac Outflow Tract TableCathyCluverNo ratings yet
- HEALTH CARE DELIVERY SYSTEM Lesson PlanDocument22 pagesHEALTH CARE DELIVERY SYSTEM Lesson PlanJosephin dayanaNo ratings yet
- Personalized AyurvedDocument13 pagesPersonalized AyurvedAtul WaghNo ratings yet
- Janumet PM eDocument62 pagesJanumet PM eRaffi DerderianNo ratings yet
- SPIRITUALITYDocument4 pagesSPIRITUALITYAnne Arboleda100% (1)
- SPM TRIAL 2007 English Paper 2Document19 pagesSPM TRIAL 2007 English Paper 2Raymond Cheang Chee-CheongNo ratings yet
- Eng Kafo PDFDocument20 pagesEng Kafo PDFRaden Achmad Candra PutraNo ratings yet
- Kalamata Programma FinalDocument26 pagesKalamata Programma FinalkalamatasummercampNo ratings yet
- Paediatric Drug Chart CalculatorDocument3 pagesPaediatric Drug Chart CalculatorgregraynerNo ratings yet
- Mukta Sharma ReportDocument2 pagesMukta Sharma ReportARUN SHANKARNo ratings yet
- Quality Control of Sterile ProductsDocument21 pagesQuality Control of Sterile Productskunasahu1100% (3)
- PBL GuideDocument30 pagesPBL GuideNur Afiqa AzalanNo ratings yet
- Why Am I So Sick - Traditional Medical AstrologyDocument3 pagesWhy Am I So Sick - Traditional Medical AstrologyKevin RiceNo ratings yet
- Baroudi Seroma - How To Avoid It and How To Treat ItDocument3 pagesBaroudi Seroma - How To Avoid It and How To Treat ItLuisCRNo ratings yet
- Post DeliveryDocument26 pagesPost DeliverySaid Said (ابو خالد)No ratings yet
- FORMULARIUM Kasih Karunia 2021Document32 pagesFORMULARIUM Kasih Karunia 2021dwirahma slNo ratings yet
- Health Care Delivery System FinalDocument14 pagesHealth Care Delivery System FinalAkhosh Somarajan79% (14)
- Continued Growth Hormone GH Treatment ADocument5 pagesContinued Growth Hormone GH Treatment AAnghel Ana-MariaNo ratings yet
- Tugas Bhs. Inggris: Nama: Muhamad Wahyu S. Kelas: Xiipa2 NO.: 19Document4 pagesTugas Bhs. Inggris: Nama: Muhamad Wahyu S. Kelas: Xiipa2 NO.: 19Wahyu SetyobudiNo ratings yet
- Broncho DilatorsDocument53 pagesBroncho DilatorsDocRNNo ratings yet
- Open Letter To NJSDDocument4 pagesOpen Letter To NJSDWBAYNo ratings yet
- IMNCI Chart Booklet (New) OrignalDocument36 pagesIMNCI Chart Booklet (New) OrignaleresdNo ratings yet
- Shimadzu Radspeed MC Radspeed M BrochureDocument5 pagesShimadzu Radspeed MC Radspeed M BrochureMuhammad Areeb100% (1)
- Drug PresentationDocument9 pagesDrug PresentationAddah, Dhenaraiza H.No ratings yet
- HIV and Islam Is HIV Prevalence Lower Am PDFDocument6 pagesHIV and Islam Is HIV Prevalence Lower Am PDFPriyo DjatmikoNo ratings yet
- 1st Round CounsellngDocument112 pages1st Round CounsellngRavi SinghNo ratings yet
- Mechanical Ventilation of Adults in The Emergency Department - UpToDateDocument28 pagesMechanical Ventilation of Adults in The Emergency Department - UpToDateCarlos E. Morales AyoraNo ratings yet
- WISC IV Cross Culture ComparisonDocument21 pagesWISC IV Cross Culture ComparisongwzglNo ratings yet
- Reabilitare Dupa AvcDocument91 pagesReabilitare Dupa AvcDiana StancaNo ratings yet