Download as pdf or txt
You might also like
- CST Interview Guide PDFDocument159 pagesCST Interview Guide PDFTaha Haq100% (1)
- TVP-2020-1112 Managing Feline Urethral ObstructionDocument6 pagesTVP-2020-1112 Managing Feline Urethral ObstructionLucas Dos Santos MacedoNo ratings yet
- PRN00936 II Pharmacy First Clinical Pathways v.1.6Document7 pagesPRN00936 II Pharmacy First Clinical Pathways v.1.6Oladimeji Raphael OnibonNo ratings yet
- Test Bank Medical Terminology A Short Course 6th Edition ChabnerDocument12 pagesTest Bank Medical Terminology A Short Course 6th Edition ChabnerDawn Fischer100% (35)
- Harmonized Household Profiling ToolDocument2 pagesHarmonized Household Profiling ToolJessa Mae89% (9)
- GI NursingDocument14 pagesGI NursingKarl Bayonito100% (5)
- Lesson Plan ON Assessment of Urinary SystemDocument11 pagesLesson Plan ON Assessment of Urinary SystemVeenasravanthi100% (1)
- Acute Painful Scrotum: ALGORITHM-Suspicion For Testicular TorsionDocument13 pagesAcute Painful Scrotum: ALGORITHM-Suspicion For Testicular TorsionM. ANDRI PRASETYONo ratings yet
- Emergenze Addome RXDocument9 pagesEmergenze Addome RXBrovazzo PieroNo ratings yet
- Urological RefferalDocument12 pagesUrological Refferalmichelle octavianiNo ratings yet
- XXXDocument13 pagesXXXtiaraNo ratings yet
- 3 Urinary Incontinence in WomenDocument4 pages3 Urinary Incontinence in WomenDanilo Pereira Dos SantosNo ratings yet
- finalsURINARY ELIMINATION DIAGNOSTICSDocument11 pagesfinalsURINARY ELIMINATION DIAGNOSTICSFrances LiqueNo ratings yet
- Acute Abdomen Practical Approach FransDocument29 pagesAcute Abdomen Practical Approach FransAbel MncaNo ratings yet
- Ilovepdf Merged 2-69Document1 pageIlovepdf Merged 2-69qwivy.comNo ratings yet
- Abdominal PainDocument3 pagesAbdominal PainNoor AlblushiNo ratings yet
- 4 Protocol For Snakebite Management 1.4Document1 page4 Protocol For Snakebite Management 1.4Aakash BalasubramanianNo ratings yet
- Im Irritable Bowel Syndrome Intestinal Obstruction Acute Appendicitis Lecture TransDocument6 pagesIm Irritable Bowel Syndrome Intestinal Obstruction Acute Appendicitis Lecture TransMelissa LabadorNo ratings yet
- Urinary Tract Infection and Pyelonephritis AIIMS Kalyani 7th SemesterDocument39 pagesUrinary Tract Infection and Pyelonephritis AIIMS Kalyani 7th Semesterrakesh raushanNo ratings yet
- Acute AUBDocument9 pagesAcute AUBJessa MaeNo ratings yet
- High Velocity Manipulation TechniquesDocument2 pagesHigh Velocity Manipulation TechniquesBhargavaNo ratings yet
- Nausea and Vomiting PDFDocument8 pagesNausea and Vomiting PDFRoosita Arbaane SafitriNo ratings yet
- Evidence Statement Anal Incontinence Flowchart PDFDocument2 pagesEvidence Statement Anal Incontinence Flowchart PDFsilkofosNo ratings yet
- KNGF Evidence Statement: Anal IncontinenceDocument2 pagesKNGF Evidence Statement: Anal IncontinencesilkofosNo ratings yet
- Pelvic Anatomy Slides FINALDocument36 pagesPelvic Anatomy Slides FINALRajashekharNo ratings yet
- Cholecyctitis Nursing Concept Map DocDocument1 pageCholecyctitis Nursing Concept Map DocSteffiNo ratings yet
- Acute Abdominal Pain Pathway: Management - Primary Care and Community SettingsDocument2 pagesAcute Abdominal Pain Pathway: Management - Primary Care and Community Settingsshella1selinaNo ratings yet
- H.A.M. Akil Fardah Akil: "GI Disorders" Lecture in GERIATRI System, FKUHDocument14 pagesH.A.M. Akil Fardah Akil: "GI Disorders" Lecture in GERIATRI System, FKUHCutDianafitriaNo ratings yet
- Làm Gì Khi SDMA TăngDocument1 pageLàm Gì Khi SDMA TăngNguyễn Tấn TàiNo ratings yet
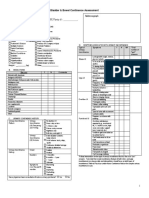
- Bladder & Bowel Continence Assessment: Chart (C), RN, RPN, PSW, OtherDocument4 pagesBladder & Bowel Continence Assessment: Chart (C), RN, RPN, PSW, OtherMeenakshiputraeashwarprasad MacherlaNo ratings yet
- Appendicitis: Anetha Jodhan Ravindra SinghDocument34 pagesAppendicitis: Anetha Jodhan Ravindra SinghMarlon GeorgeNo ratings yet
- 69 Obstrucc - IntestinalDocument10 pages69 Obstrucc - IntestinalMaria Jose GiraldoNo ratings yet
- Colorectal CancerDocument11 pagesColorectal CancerFrances LiqueNo ratings yet
- LUTS-OAB ManagementDocument26 pagesLUTS-OAB Managementratihdyahayu_rdaNo ratings yet
- Drug StudyDocument5 pagesDrug StudyGAYOL BREEN IRAH A.No ratings yet
- The GI System Is Composed of Two General Parts Gi TractDocument14 pagesThe GI System Is Composed of Two General Parts Gi TractRexson Alcantara DalanginNo ratings yet
- 1-Differential Diagnosis of Vomiting 2021 PsáderR SAM3Document28 pages1-Differential Diagnosis of Vomiting 2021 PsáderR SAM3Simay KızılkayaNo ratings yet
- Illustrator File Edit Select Effect View Window HelpDocument9 pagesIllustrator File Edit Select Effect View Window HelpHaizel BieberNo ratings yet
- HARLE FinalsDocument15 pagesHARLE Finalsangelapadilla0893No ratings yet
- 02 ConstipationDocument11 pages02 ConstipationYunus AmmarieNo ratings yet
- Cause: Diverticular DiseaseDocument4 pagesCause: Diverticular DiseaseJANELLE GIFT SENARLONo ratings yet
- Urinary StoneDocument5 pagesUrinary StoneThakoon TtsNo ratings yet
- 1 Urinary Incontinence in ChildrenDocument5 pages1 Urinary Incontinence in Childrenguido murrieta rojasNo ratings yet
- Assignment GiDocument14 pagesAssignment GiVoid LessNo ratings yet
- Pathophysiology of CholelithiasisDocument2 pagesPathophysiology of CholelithiasisSherilNo ratings yet
- Acute Abdomen (Modified From DR James Roring)Document18 pagesAcute Abdomen (Modified From DR James Roring)Arga KafiNo ratings yet
- Palliative Care Management of ConstipationDocument5 pagesPalliative Care Management of ConstipationnehaNo ratings yet
- DR Remson SPB - Akut AbdomenDocument38 pagesDR Remson SPB - Akut AbdomenArio RinaldoNo ratings yet
- Abdome AgudoDocument63 pagesAbdome AgudoAnne Caroline De Morais AlvesNo ratings yet
- Acute Abdomen: The "Black Hole" of MedicineDocument97 pagesAcute Abdomen: The "Black Hole" of Medicineedward iskandarNo ratings yet
- Protocol-ABDOMINAL DISTENTION-ServandoDocument4 pagesProtocol-ABDOMINAL DISTENTION-ServandoAllison Eunice ServandoNo ratings yet
- Acute AbdomenDocument31 pagesAcute AbdomenWildan AngelouNo ratings yet
- 1 Gastrointestinal System DisordersDocument14 pages1 Gastrointestinal System DisordersAnna Sofia Reyes100% (1)
- Preceptorial Format 2023 Group 2Document5 pagesPreceptorial Format 2023 Group 2Cayla DeniceNo ratings yet
- Quiz BukasDocument3 pagesQuiz BukasDYRAH GRACE COPAUSNo ratings yet
- How Can You Help Your Patients With An Uncomplicated UTI?: Know?Document1 pageHow Can You Help Your Patients With An Uncomplicated UTI?: Know?gegeNo ratings yet
- Akut Abdomen Aspek Klinis Dan DiagnosisDocument41 pagesAkut Abdomen Aspek Klinis Dan DiagnosisAchmad Yunus100% (1)
- Volvulus GROUP 4Document7 pagesVolvulus GROUP 41S VILLEGAS GabrielNo ratings yet
- Abdominal Pain: LSU Medical Student Clerkship, New Orleans, LADocument48 pagesAbdominal Pain: LSU Medical Student Clerkship, New Orleans, LALeonardo Adi BestNo ratings yet
- Isolated Hematuria - Genitourinary Disorders - MSD Manual Professional EditionDocument3 pagesIsolated Hematuria - Genitourinary Disorders - MSD Manual Professional EditionleozdmNo ratings yet
- Abdominal Pain: Kerut SuardanaDocument48 pagesAbdominal Pain: Kerut SuardanaDiah SandiNo ratings yet
- An Approach To The Acute AbdomenDocument6 pagesAn Approach To The Acute AbdomenHardik JeenaNo ratings yet
- 7 Abdominal TraumaDocument9 pages7 Abdominal TraumaMyrtle Yvonne RagubNo ratings yet
- The Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesFrom EverandThe Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesNo ratings yet
- Vitamin D Deficiency PathwayDocument12 pagesVitamin D Deficiency PathwayJessa MaeNo ratings yet
- SepsisDocument10 pagesSepsisJessa MaeNo ratings yet
- Thrombosis ManagementDocument14 pagesThrombosis ManagementJessa MaeNo ratings yet
- Acetaminophen (APAP) ToxicityDocument12 pagesAcetaminophen (APAP) ToxicityJessa MaeNo ratings yet
- Sanitary Permit To Operate TabinaDocument1 pageSanitary Permit To Operate TabinaJessa MaeNo ratings yet
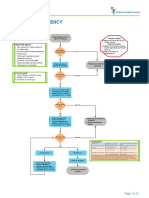
- Undescended Testicle PathwayDocument8 pagesUndescended Testicle PathwayJessa MaeNo ratings yet
- FORMS Informed Consent (For Procedures)Document1 pageFORMS Informed Consent (For Procedures)Jessa MaeNo ratings yet
- Acute Chest Syndrome (ACS) CCGDocument11 pagesAcute Chest Syndrome (ACS) CCGJessa MaeNo ratings yet
- RHU Various Sanitary FormsDocument5 pagesRHU Various Sanitary FormsJessa MaeNo ratings yet
- FORMS Reseta and All Forms 2022 PDFDocument16 pagesFORMS Reseta and All Forms 2022 PDFJessa MaeNo ratings yet
- Referral Form Jessa 2021Document1 pageReferral Form Jessa 2021Jessa MaeNo ratings yet
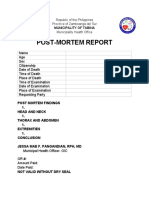
- Postmortem Report Tabina 2022Document1 pagePostmortem Report Tabina 2022Jessa MaeNo ratings yet
- Driver Ticket FormDocument4 pagesDriver Ticket FormJessa MaeNo ratings yet
- Exhumation PermitDocument1 pageExhumation PermitJessa Mae0% (1)
- Sexually Transmitted InfectionsDocument73 pagesSexually Transmitted InfectionsJessa MaeNo ratings yet
- Kidney Healthy Diet Cebuano EditionDocument2 pagesKidney Healthy Diet Cebuano EditionJessa MaeNo ratings yet
- Free XrayDocument2 pagesFree XrayJessa MaeNo ratings yet
- FB POST CKD FOODDocument2 pagesFB POST CKD FOODJessa MaeNo ratings yet
- Pediatric Community-Acquired Pneumonia: CC Trisha Pamela OquendoDocument70 pagesPediatric Community-Acquired Pneumonia: CC Trisha Pamela OquendoJessa MaeNo ratings yet
- Kidney Healthy DietDocument4 pagesKidney Healthy DietJessa MaeNo ratings yet
- PhilHealth Circular 2020-0021 Accreditation For Provision of Konsulta Package As Primary Care Benefit PackageDocument7 pagesPhilHealth Circular 2020-0021 Accreditation For Provision of Konsulta Package As Primary Care Benefit PackageJessa MaeNo ratings yet
- MalariaDocument1 pageMalariaJessa MaeNo ratings yet
- Health Assessment FormDocument2 pagesHealth Assessment FormJessa MaeNo ratings yet
- JAO 2020-0001 Registration of Filipino To PCPDocument5 pagesJAO 2020-0001 Registration of Filipino To PCPJessa MaeNo ratings yet
- dm2021 0261 Advisory On Provisional Primary Care CertificationDocument2 pagesdm2021 0261 Advisory On Provisional Primary Care CertificationJessa Mae75% (4)
- Family Planning: CC Bernabe Excelsior 2017Document51 pagesFamily Planning: CC Bernabe Excelsior 2017Jessa MaeNo ratings yet
- Facility Service Assessment Tool For Primary Care FacilitiesDocument15 pagesFacility Service Assessment Tool For Primary Care FacilitiesJessa MaeNo ratings yet
- Dystocia: August Gay C. MilitanteDocument39 pagesDystocia: August Gay C. MilitanteJessa MaeNo ratings yet
- DIABETESDocument44 pagesDIABETESJessa MaeNo ratings yet
- AIAPGET: 2021: RD THDocument13 pagesAIAPGET: 2021: RD THNikhil BisuiNo ratings yet
- Urinary Tract Infection in Older Adults: DefinitionsDocument10 pagesUrinary Tract Infection in Older Adults: DefinitionsWila AnandaNo ratings yet
- Nephritic, Nephrotic Syndrome and Acute Kidney Injury in ChildrenDocument79 pagesNephritic, Nephrotic Syndrome and Acute Kidney Injury in ChildrenB AuNo ratings yet
- MS UrologyDocument73 pagesMS UrologyZeeshan AliNo ratings yet
- Acute Renal Failure DXDocument7 pagesAcute Renal Failure DXfarid akbarNo ratings yet
- NSAIDs - Acute Kidney Injury (Acute Renal Failure) - UpToDateDocument14 pagesNSAIDs - Acute Kidney Injury (Acute Renal Failure) - UpToDateLucía Aldhaiz Lazo CusihuallpaNo ratings yet
- Patofisiologi Kolik RenalDocument6 pagesPatofisiologi Kolik RenalGusti FerriNo ratings yet
- Approach To Hematuria and Proteinuria in ChildrenDocument52 pagesApproach To Hematuria and Proteinuria in ChildrenMysheb SS100% (1)
- Urinary Tract InfectionsDocument23 pagesUrinary Tract InfectionsJay AberinNo ratings yet
- Diseases o F Urinary System 5 LevelDocument6 pagesDiseases o F Urinary System 5 LevelABDULLAH AMROONNo ratings yet
- Child With HematuriaDocument42 pagesChild With HematuriaalaaNo ratings yet
- Common Medical AbbreviationsDocument4 pagesCommon Medical AbbreviationsApril Joy de LimaNo ratings yet
- NCM 114 Case Scenario Surgical Rotation 1 2Document13 pagesNCM 114 Case Scenario Surgical Rotation 1 2Darren RobertoNo ratings yet
- AUA GuidelinesDocument9 pagesAUA GuidelinesAna Maria rendonNo ratings yet
- Urinary Tract Infection: Arnaiz, Neptaly PDocument49 pagesUrinary Tract Infection: Arnaiz, Neptaly PNeptaly P. ArnaizNo ratings yet
- ICD 10 & Icd 9 Rawat Jalan: Daftar KodingDocument26 pagesICD 10 & Icd 9 Rawat Jalan: Daftar KodingdanuantariNo ratings yet
- Chapter 21 - Urologic Aspects of Pediatric Nephrology - Campbell - Walsh-Wein UROLOGY 12thDocument19 pagesChapter 21 - Urologic Aspects of Pediatric Nephrology - Campbell - Walsh-Wein UROLOGY 12thkrisnaNo ratings yet
- 156-Article Text-211-1-10-20211028Document6 pages156-Article Text-211-1-10-20211028Manoj KumarNo ratings yet
- Renal UroDocument120 pagesRenal UroMazharul IslamNo ratings yet
- DiagnosisManagementOfRenalColic PDFDocument7 pagesDiagnosisManagementOfRenalColic PDFイアン リムホト ザナガNo ratings yet
- ACP Board Review Nephrology 20052ndDocument35 pagesACP Board Review Nephrology 20052nddoctormido2010100% (1)
- Surgitoons Part 3 Special SurgeryDocument157 pagesSurgitoons Part 3 Special Surgerywertfghuji100% (7)
- Lecture 2 - Urine ExaminationDocument62 pagesLecture 2 - Urine ExaminationmihalachemirelaNo ratings yet
- Sign and Symptoms in Urology 1Document15 pagesSign and Symptoms in Urology 1Sri PertiwiNo ratings yet
- A Detailed Lesson Plan in Science IvDocument4 pagesA Detailed Lesson Plan in Science IvEmiliano Dela CruzNo ratings yet
- Clinical Manifestations and Diagnostic Evaluation of Benign Prostatic Hyperplasia - UpToDateDocument11 pagesClinical Manifestations and Diagnostic Evaluation of Benign Prostatic Hyperplasia - UpToDateFeer VillarrealNo ratings yet
- Soal MCQDocument39 pagesSoal MCQRonald Allan Valle SantosNo ratings yet