Download as pdf or txt
You might also like
- USA Doctors DirectoryDocument280 pagesUSA Doctors Directorysonukarma321100% (1)
- Total Burn CareDocument896 pagesTotal Burn CareAdrián Armada100% (3)
- Evidence Based Nursing PracticeDocument21 pagesEvidence Based Nursing PracticeChithra Saju71% (7)
- Dementia Research ProposalDocument12 pagesDementia Research ProposalOmowunmiItunuNo ratings yet
- Ovarian Cancer Paper Final Version 4Document9 pagesOvarian Cancer Paper Final Version 4api-241216897No ratings yet
- J Ijscr 2020 10 081Document4 pagesJ Ijscr 2020 10 081Fatma BalciNo ratings yet
- Gossypiboma Revisited A Never Ending IssueDocument5 pagesGossypiboma Revisited A Never Ending IssueChon ChiNo ratings yet
- Isj-5899 oDocument5 pagesIsj-5899 oAbhiram MundleNo ratings yet
- Articulo de Daños de OblitoDocument6 pagesArticulo de Daños de OblitofernazocarNo ratings yet
- A Prospective Comparativestudy of Open Versus Laparoscopic Appendectomy: A Single Unit StudyDocument8 pagesA Prospective Comparativestudy of Open Versus Laparoscopic Appendectomy: A Single Unit StudyIJAR JOURNALNo ratings yet
- Clinical Study of Incidence and Surgical Management of Incisional HerniaDocument4 pagesClinical Study of Incidence and Surgical Management of Incisional HerniaDevasyaNo ratings yet
- Open Versus Laparoscopic Mesh Repair of Ventral Hernias: A Prospective StudyDocument3 pagesOpen Versus Laparoscopic Mesh Repair of Ventral Hernias: A Prospective Study'Adil MuhammadNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument9 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Surgery & Surgical Procedures: International Journal ofDocument3 pagesSurgery & Surgical Procedures: International Journal ofRinaldy T SetiawanNo ratings yet
- Dubois 2010Document7 pagesDubois 2010mia widiastutiNo ratings yet
- Oamjms 10b 1148Document5 pagesOamjms 10b 1148hanifNo ratings yet
- Histeroctomy PDFDocument6 pagesHisteroctomy PDFsanta_pangaribuan_1No ratings yet
- Choksey M Malik I Shunt - InfectionsDocument5 pagesChoksey M Malik I Shunt - InfectionsmunchisolichokseyNo ratings yet
- Dolivet 2020Document6 pagesDolivet 2020Jasper RaelisonNo ratings yet
- Laparoscopic Appendectomy For Complicated Appendicitis - An Evaluation of Postoperative Factors.Document5 pagesLaparoscopic Appendectomy For Complicated Appendicitis - An Evaluation of Postoperative Factors.Juan Carlos SantamariaNo ratings yet
- Laparoscopic Appendicectomy in All Trimesters of PregnancyDocument7 pagesLaparoscopic Appendicectomy in All Trimesters of PregnancyJason CalvinNo ratings yet
- Laparoscopic Appendectomy PostoperativeDocument6 pagesLaparoscopic Appendectomy PostoperativeDamal An NasherNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument5 pagesAnnals of Medicine and Surgery: SciencedirectMishel Rodriguez GuzmanNo ratings yet
- Role of Wound Drains VS Abdominal Binder and Percutaneous Aspiration After Open Repair of Ventral Hernia Using Polyprolene MeshDocument12 pagesRole of Wound Drains VS Abdominal Binder and Percutaneous Aspiration After Open Repair of Ventral Hernia Using Polyprolene MeshIJAR JOURNALNo ratings yet
- Ciencia e Technica Omentum Overlay PDFDocument10 pagesCiencia e Technica Omentum Overlay PDFAlin MihetiuNo ratings yet
- Journal AppDocument3 pagesJournal AppliqqamuqitaNo ratings yet
- Cierre de Piel de Herida de Estoma Con Tecnica Purse-StringDocument7 pagesCierre de Piel de Herida de Estoma Con Tecnica Purse-Stringjesus aguirreNo ratings yet
- Emergency Inguinal Hernia Repair Under Local Anesthesia: A 5-Year Experience in A Teaching HospitalDocument5 pagesEmergency Inguinal Hernia Repair Under Local Anesthesia: A 5-Year Experience in A Teaching HospitalleonardoNo ratings yet
- Updateon OvariohysterecomtyDocument9 pagesUpdateon Ovariohysterecomtysimon alfaro gonzálezNo ratings yet
- Hernia UmmaDocument9 pagesHernia UmmaHeny KambuNo ratings yet
- Hernia InguinalisDocument7 pagesHernia InguinalisabduNo ratings yet
- 1 s2.0 S1015958422008909 MainDocument4 pages1 s2.0 S1015958422008909 MainYohan WijayabahuNo ratings yet
- Research ArticleDocument4 pagesResearch Articleshah hassaanNo ratings yet
- Souza 2017Document4 pagesSouza 2017CRISTHIAN CASTILLO JIBAJANo ratings yet
- Complicated AppendicitisDocument4 pagesComplicated AppendicitisMedardo ApoloNo ratings yet
- Article IJGCP 131 PDFDocument7 pagesArticle IJGCP 131 PDFDSSNo ratings yet
- An Unconventional Therapeutic Approach To A Migratory IUD Causing Perforation of The RectumDocument2 pagesAn Unconventional Therapeutic Approach To A Migratory IUD Causing Perforation of The Rectumvianchasamiera berlianaNo ratings yet
- Stuck Up!!! - Case Report of A Rectal Foreign BodyDocument6 pagesStuck Up!!! - Case Report of A Rectal Foreign BodyIJAR JOURNALNo ratings yet
- Closure Vs Nonclosure of PeritoneumDocument6 pagesClosure Vs Nonclosure of PeritoneumFrancisco Xavier Beltrán Vallejo100% (1)
- 1 s2.0 S2214751921001584 MainDocument7 pages1 s2.0 S2214751921001584 MainfitriNo ratings yet
- Zero Tolerance To Shunt Infections: Can It Be Achieved?: PaperDocument5 pagesZero Tolerance To Shunt Infections: Can It Be Achieved?: PaperChristian Sanchez AlvaNo ratings yet
- Surgical Management of Recurrent Inguinal Hernia A Study of 50 Cases - April - 2023 - 9089115640 - 5948273Document3 pagesSurgical Management of Recurrent Inguinal Hernia A Study of 50 Cases - April - 2023 - 9089115640 - 5948273Ssam CivilNo ratings yet
- Synthetic Versus Biological Mesh in Laparoscopic and Open Ventral Hérnia RepairDocument9 pagesSynthetic Versus Biological Mesh in Laparoscopic and Open Ventral Hérnia RepairRhuan AntonioNo ratings yet
- Yang 2019Document6 pagesYang 2019Imron BuhoriNo ratings yet
- Conventional Versus Laparoscopic Surgery For Acute AppendicitisDocument4 pagesConventional Versus Laparoscopic Surgery For Acute AppendicitisAna Luiza MatosNo ratings yet
- Entrapment of A Vaginal Ring Pessary - Case Report and Review of The LiteratureDocument2 pagesEntrapment of A Vaginal Ring Pessary - Case Report and Review of The LiteratureDR RISKA WAHYUNo ratings yet
- Complicationsoflapmyomectomy ANZ 2010Document7 pagesComplicationsoflapmyomectomy ANZ 2010Nadila 01No ratings yet
- ACUTE ABDOMEN Systemic SonographicDocument6 pagesACUTE ABDOMEN Systemic SonographiciwanNo ratings yet
- Prospective Evaluation of A New Device For The Treatment of Anal Fistulas 2016Document9 pagesProspective Evaluation of A New Device For The Treatment of Anal Fistulas 2016waldemar russellNo ratings yet
- Cirocchi2017 PDFDocument18 pagesCirocchi2017 PDFAndres TameNo ratings yet
- Recurrence of Ovarian Endometrioma After Laparoscopic ExcisionDocument4 pagesRecurrence of Ovarian Endometrioma After Laparoscopic ExcisionPutri Tamara DasantosNo ratings yet
- The Learning Curve For Hernia PDFDocument5 pagesThe Learning Curve For Hernia PDFIgor CemortanNo ratings yet
- MonopolarDocument2 pagesMonopolarTariNo ratings yet
- Two-Port Laparoscopic Appendectomy Assisted With Needle Grasper Comparison With Conventional..Document7 pagesTwo-Port Laparoscopic Appendectomy Assisted With Needle Grasper Comparison With Conventional..andreigustvNo ratings yet
- Inguinal HerniaDocument9 pagesInguinal HerniaAmanda RapaNo ratings yet
- Alexanders Care of The Patient in Surgery Rothrock 16th Edition Test BankDocument9 pagesAlexanders Care of The Patient in Surgery Rothrock 16th Edition Test Bankjoshuabakergpctsonbwj100% (40)
- Incidental Finding and Successful Management of La 2024 International JournaDocument3 pagesIncidental Finding and Successful Management of La 2024 International JournaRonald QuezadaNo ratings yet
- Test Bank Alexanders Care of The Patient in Surgery 16th Edition Rothrock DownloadDocument9 pagesTest Bank Alexanders Care of The Patient in Surgery 16th Edition Rothrock Downloadlaurafloresejzawnptxr100% (30)
- Perioperative Nursing Module 1Document169 pagesPerioperative Nursing Module 1fleur harrisonNo ratings yet
- Main PDFDocument4 pagesMain PDFhhNo ratings yet
- Trocar-Related Abdominal Wall Bleeding in 200 Patients After LAPAROSCOPIC CHOLECISTECTOMY 2006Document3 pagesTrocar-Related Abdominal Wall Bleeding in 200 Patients After LAPAROSCOPIC CHOLECISTECTOMY 2006waldemar russellNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument11 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Is 9Document9 pagesIs 9intan juitaNo ratings yet
- Brown 2014Document8 pagesBrown 2014nelly alconzNo ratings yet
- Case Studies of Postoperative Complications after Digestive SurgeryFrom EverandCase Studies of Postoperative Complications after Digestive SurgeryNo ratings yet
- Agency AssessmentDocument3 pagesAgency Assessmentapi-543254470No ratings yet
- Psychiatric Outcomes After Temporal Lobe Surgery in Patients With Temporal Lobe Epilepsy and Comorbid Psychiatric IllnessDocument8 pagesPsychiatric Outcomes After Temporal Lobe Surgery in Patients With Temporal Lobe Epilepsy and Comorbid Psychiatric IllnessFrancisco Javier Fierro RestrepoNo ratings yet
- Author Book TitleDocument13 pagesAuthor Book TitlejenniferxarmstrongNo ratings yet
- Nasogastric NG Tube Insertion OSCE GuideDocument7 pagesNasogastric NG Tube Insertion OSCE Guidepunam todkarNo ratings yet
- Manfaat Penerapan Rekam Medis Elektronik Di Negara Berkembang: Systematic Literature ReviewDocument11 pagesManfaat Penerapan Rekam Medis Elektronik Di Negara Berkembang: Systematic Literature ReviewLusi nurhayati SimanjuntakNo ratings yet
- CARNA Entry To Practice CompetenciesDocument24 pagesCARNA Entry To Practice Competenciesparisa.ahmed97No ratings yet
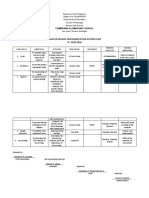
- Wash in School Implementation Action Plan SY. 2019-2020Document2 pagesWash in School Implementation Action Plan SY. 2019-2020RONALYN ALVAREZNo ratings yet
- Myanmar LNGO Directory 2012Document138 pagesMyanmar LNGO Directory 2012kk_mangneo100% (1)
- Highest Paying Psychology CoursesDocument3 pagesHighest Paying Psychology CoursestriptirathoreNo ratings yet
- Perioperative Care of The Cancer Patient Carin A Hagberg Vijaya N R Gottumukkala Bernhard J Riedel Joseph L Nates Donal J BuggyDocument70 pagesPerioperative Care of The Cancer Patient Carin A Hagberg Vijaya N R Gottumukkala Bernhard J Riedel Joseph L Nates Donal J Buggychristopherboyd498343100% (4)
- SC DHEC Infant Mortality Rate ReportDocument40 pagesSC DHEC Infant Mortality Rate ReportABC15 NewsNo ratings yet
- Infection Control InstituteDocument43 pagesInfection Control InstitutePŕìncëş Ğï ŘlNo ratings yet
- Information About Fm-Proc (Family Medicine Professional Choices)Document4 pagesInformation About Fm-Proc (Family Medicine Professional Choices)Hayder Al-TukmachiNo ratings yet
- RHCF: Reaching Primary Healthcare To The Base of The PyramidDocument31 pagesRHCF: Reaching Primary Healthcare To The Base of The PyramidHensi ShethNo ratings yet
- Proposed Training Design On The Symposium of Mental Health Among Barangay Health Workers and OfficialsDocument24 pagesProposed Training Design On The Symposium of Mental Health Among Barangay Health Workers and Officialswilliam bill doria100% (1)
- BDS - Programme - Textbook - List - 2016-17 For UK StudentsDocument5 pagesBDS - Programme - Textbook - List - 2016-17 For UK StudentsIshita SangiaNo ratings yet
- Sharma, Deven Prasad (2016) : Summary of Medical Device Law in New Zealand 2016Document30 pagesSharma, Deven Prasad (2016) : Summary of Medical Device Law in New Zealand 2016walterpdrakeNo ratings yet
- "Robodoc". The New Era of The Medical World.Document18 pages"Robodoc". The New Era of The Medical World.Merey SabdenaliyevaNo ratings yet
- Rphost/ E-Mail: Nationalhr@hse - IeDocument2 pagesRphost/ E-Mail: Nationalhr@hse - Iemuhammad tayyabNo ratings yet
- LEGASPI Nomination Papers For PGH Directorship (2015)Document6 pagesLEGASPI Nomination Papers For PGH Directorship (2015)karl_poorNo ratings yet
- NTB ppt-1Document76 pagesNTB ppt-1yazgariNo ratings yet
- LESSON TITLE: Confidentiality and The Management of Health Care InformationDocument2 pagesLESSON TITLE: Confidentiality and The Management of Health Care InformationLovelie GuerroNo ratings yet
- Management of Primigravida With Unengaged Head at Term: Original ArticleDocument4 pagesManagement of Primigravida With Unengaged Head at Term: Original Articleedi_wsNo ratings yet
- Guide To Informed Decision-Making in Health CareDocument80 pagesGuide To Informed Decision-Making in Health CareClauNo ratings yet
- Wesleyan University-Philippines: Mabini Extension, Cabanatuan City, Philippines 3100Document5 pagesWesleyan University-Philippines: Mabini Extension, Cabanatuan City, Philippines 3100Myla Narciso CunananNo ratings yet