Download as pdf or txt
You might also like
- Otitis Media: Bagian Ilmu Kesehatan THT-KL Fakultas Kedokteran Universitas Pattimura Ambon 2018Document2 pagesOtitis Media: Bagian Ilmu Kesehatan THT-KL Fakultas Kedokteran Universitas Pattimura Ambon 2018Riqqah USNo ratings yet
- Etiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisDocument8 pagesEtiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisakhmadNo ratings yet
- Higher Platelet Counts Are Associated With Metabolic Syndrome Independent of Fatty Liver DiagnosisDocument8 pagesHigher Platelet Counts Are Associated With Metabolic Syndrome Independent of Fatty Liver DiagnosisNestor TapiaNo ratings yet
- Imunosupresie in HCVDocument8 pagesImunosupresie in HCVdeliaNo ratings yet
- Medi 94 E1123Document7 pagesMedi 94 E1123ardytawaradaniNo ratings yet
- Lesson 9 Article 2Document11 pagesLesson 9 Article 2JafinNo ratings yet
- AppbjDocument6 pagesAppbjGilang IrwansyahNo ratings yet
- International Journal of Scientific Research: Internal MedicineDocument4 pagesInternational Journal of Scientific Research: Internal MedicineGreenThumbNo ratings yet
- Article 1540976401 PDFDocument3 pagesArticle 1540976401 PDFnreena aslamNo ratings yet
- A Cross-Sectional Study Reagarding Spectrum of Acute Viral Hepatitis at Our HospitalDocument3 pagesA Cross-Sectional Study Reagarding Spectrum of Acute Viral Hepatitis at Our Hospitalnreena aslamNo ratings yet
- Incidence and Risk Factors of Anti-Tuberculosis DRDocument11 pagesIncidence and Risk Factors of Anti-Tuberculosis DRDi LaNo ratings yet
- Pone 0190952Document14 pagesPone 0190952SangiliNo ratings yet
- Diacerein For The Treatment of Rheumatoid Arthritis in Patients With Inadequate Response To Methotrexate A Pilot Randomized, Double-Blind, Placebo-Controlled Add-On Trial - TEM HTMLDocument11 pagesDiacerein For The Treatment of Rheumatoid Arthritis in Patients With Inadequate Response To Methotrexate A Pilot Randomized, Double-Blind, Placebo-Controlled Add-On Trial - TEM HTMLAline Leal CortesNo ratings yet
- Apasl HBV Guideline 2016Document98 pagesApasl HBV Guideline 2016Nadya LiemNo ratings yet
- Clinical Profile of Patients With Acute Pancreatitis: Research ArticleDocument4 pagesClinical Profile of Patients With Acute Pancreatitis: Research ArticleN MemonNo ratings yet
- Hepatic Steatosis and Fibrosis in Chronic Hepatitis C in TaiwanDocument5 pagesHepatic Steatosis and Fibrosis in Chronic Hepatitis C in TaiwansaadNo ratings yet
- Oral CancerDocument7 pagesOral CancerBima Ewando KabanNo ratings yet
- Lee 2019Document14 pagesLee 2019Caique SilvaNo ratings yet
- 2015 Article 9675 PDFDocument98 pages2015 Article 9675 PDFRio MulyaNo ratings yet
- Apasl HBV Guideline 2016 PDFDocument98 pagesApasl HBV Guideline 2016 PDFDewanggaWahyuPrajaNo ratings yet
- Clinical Pharmacy Therapeu - 2020 - Wu - Loading Dose and Efficacy of Continuous or Extended Infusion of Beta LactamsDocument9 pagesClinical Pharmacy Therapeu - 2020 - Wu - Loading Dose and Efficacy of Continuous or Extended Infusion of Beta LactamsArturo ArturoNo ratings yet
- Content ServerDocument14 pagesContent ServerTisna WennyNo ratings yet
- 29 (Hepotin JMPR-11-319Document5 pages29 (Hepotin JMPR-11-319M.Akram TatriNo ratings yet
- JurnalDocument9 pagesJurnalAyu Indah LestariNo ratings yet
- Acute Pancreatitis. Lancet Seminar Sept 5, 2020Document9 pagesAcute Pancreatitis. Lancet Seminar Sept 5, 2020Luis Henrique SalesNo ratings yet
- APASL Guide - 2015 PDFDocument99 pagesAPASL Guide - 2015 PDFPulung Suryanta TariganNo ratings yet
- tmpC1E4 TMPDocument6 pagestmpC1E4 TMPFrontiersNo ratings yet
- Beclabuvir in Combination With Asunaprevir and Daclatasvir For Hepatitis C Virus Genotype 1 InfectionDocument12 pagesBeclabuvir in Combination With Asunaprevir and Daclatasvir For Hepatitis C Virus Genotype 1 Infectiontruongduyhieu1311No ratings yet
- Treatment of Venous Thromboembolism: ReviewDocument12 pagesTreatment of Venous Thromboembolism: ReviewMayra Alejandra Prada SerranoNo ratings yet
- Effect of Antibiotic Prophylaxis On Acute Necrotizing Pancreatitis: Results of A Randomized Controlled TrialDocument7 pagesEffect of Antibiotic Prophylaxis On Acute Necrotizing Pancreatitis: Results of A Randomized Controlled TrialKirsten HartmanNo ratings yet
- Abses HeparDocument4 pagesAbses HeparIecHa RizkaMaulidaNo ratings yet
- ACG Clinical Guideline: Management of Acute PancreatitisDocument8 pagesACG Clinical Guideline: Management of Acute PancreatitisNick ANo ratings yet
- An Observational Study To Determine Relation Between Various Indices of Acute PancreatitisDocument4 pagesAn Observational Study To Determine Relation Between Various Indices of Acute PancreatitisDr. NasrumminallahNo ratings yet
- JCM 11 04997Document11 pagesJCM 11 04997Omran AzzamNo ratings yet
- Divya Thesis Final (30th Jan)Document26 pagesDivya Thesis Final (30th Jan)smalaparaNo ratings yet
- Guidelines For The Diagnosis and Management of Hirschsprung-Associated EnterocolitisDocument5 pagesGuidelines For The Diagnosis and Management of Hirschsprung-Associated EnterocolitisNasrudin EfendiNo ratings yet
- Guideline HBV 2012 UpdateDocument31 pagesGuideline HBV 2012 UpdateHegandNo ratings yet
- Natali Zuma BDocument6 pagesNatali Zuma BsarahmooNo ratings yet
- 02 - Hav 2006Document6 pages02 - Hav 2006sunilpkumar18No ratings yet
- 1 s2.0 S0965229921000959 MainDocument7 pages1 s2.0 S0965229921000959 Mainanggana putriNo ratings yet
- Usefulness of Tumor Marker CA-125 Serum Levels For The Follow-Up of Therapeutic Responses in Tuberculosis Patients With and Without SerositisDocument6 pagesUsefulness of Tumor Marker CA-125 Serum Levels For The Follow-Up of Therapeutic Responses in Tuberculosis Patients With and Without Serositishumayun kabirNo ratings yet
- Medi 94 E1642Document8 pagesMedi 94 E1642Rudolph GameNo ratings yet
- Cambios en El Diagnostico de Hepatitis C-Jama 2014Document2 pagesCambios en El Diagnostico de Hepatitis C-Jama 2014Joe Felipe Vera OchoaNo ratings yet
- Trial of Early, Goal-Directed Resuscitation For Septic ShockDocument11 pagesTrial of Early, Goal-Directed Resuscitation For Septic Shockapi-308365861No ratings yet
- Articulo ADocument8 pagesArticulo AJaver Andres HernandezNo ratings yet
- Gastrointestinal Bleeding in Acute Pancreatitis: Etiology, Clinical Features, Risk Factors and OutcomeDocument6 pagesGastrointestinal Bleeding in Acute Pancreatitis: Etiology, Clinical Features, Risk Factors and OutcomeReni LubisNo ratings yet
- 2451-Article Text-10178-2-10-20211125Document5 pages2451-Article Text-10178-2-10-20211125rexaNo ratings yet
- Epidemiological Profile of Hepatitis C Patients at India's New Hub - HaryanaDocument6 pagesEpidemiological Profile of Hepatitis C Patients at India's New Hub - HaryanaJuniper PublishersNo ratings yet
- Prevalence of Hepatitis B and C Viruses in HIV-positive Patients in China: A Cross-Sectional StudyDocument9 pagesPrevalence of Hepatitis B and C Viruses in HIV-positive Patients in China: A Cross-Sectional StudyShree Narayan YadavNo ratings yet
- Umeno2018 Article ClinicalFeaturesOfChronicEnterDocument9 pagesUmeno2018 Article ClinicalFeaturesOfChronicEnterzhe zhNo ratings yet
- Easl Recomandari VHC 2018-15759Document51 pagesEasl Recomandari VHC 2018-15759Mihaela ShimanNo ratings yet
- Neutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisDocument7 pagesNeutrophil To Lymphocyte Ratio in Diagnosis of Complicated and Non-Complicated AppendicitisHamza AhmedNo ratings yet
- ACG Guideline Cdifficile April 2013Document21 pagesACG Guideline Cdifficile April 2013Fitria FieraNo ratings yet
- ResistinDocument3 pagesResistinDr Alamzeb JadoonNo ratings yet
- Technical and Operational - LOW RISE - 0Document68 pagesTechnical and Operational - LOW RISE - 0movieschannel307No ratings yet
- Article 2Document6 pagesArticle 2Haritha AtluriNo ratings yet
- Acute PancreatitsiDocument8 pagesAcute PancreatitsiAnty FftNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Liver Disease: A Clinical CasebookFrom EverandLiver Disease: A Clinical CasebookStanley Martin CohenNo ratings yet
- Critical Care Nutrition Therapy for Non-nutritionistsFrom EverandCritical Care Nutrition Therapy for Non-nutritionistsMette M. BergerNo ratings yet
- Evaluation and Management of Dysphagia: An Evidence-Based ApproachFrom EverandEvaluation and Management of Dysphagia: An Evidence-Based ApproachDhyanesh A. PatelNo ratings yet
- Impact of Immunosuppressive Regimen On Survival Of.20Document6 pagesImpact of Immunosuppressive Regimen On Survival Of.20deliaNo ratings yet
- Outcome Pe Termen Lung La AsociereDocument6 pagesOutcome Pe Termen Lung La AsocieredeliaNo ratings yet
- Lupus Si Ifn GeneralitatiDocument3 pagesLupus Si Ifn GeneralitatideliaNo ratings yet
- MMF Si VHC TransplantDocument11 pagesMMF Si VHC TransplantdeliaNo ratings yet
- Outcome Dupa Prednisolon Si CiclofDocument8 pagesOutcome Dupa Prednisolon Si CiclofdeliaNo ratings yet
- Ifn Si LupusDocument1 pageIfn Si LupusdeliaNo ratings yet
- VHC Si LesDocument4 pagesVHC Si LesdeliaNo ratings yet
- Lupus Si Ifn SpaniolaDocument3 pagesLupus Si Ifn SpanioladeliaNo ratings yet
- (Advances in Parasitology 35) J.R. Baker, R. Muller and D. Rollinson (Eds.) - Academic Press (1995)Document347 pages(Advances in Parasitology 35) J.R. Baker, R. Muller and D. Rollinson (Eds.) - Academic Press (1995)Stoian GoranovNo ratings yet
- Project Report On Human DiseasesDocument17 pagesProject Report On Human DiseasesNaven BansalNo ratings yet
- Autoimmune Liver DiseasesDocument8 pagesAutoimmune Liver DiseasesMehdi LaliliNo ratings yet
- Rabid: A Cultural History of The World's Most Diabolical Virus Is A Popular ScienceDocument2 pagesRabid: A Cultural History of The World's Most Diabolical Virus Is A Popular ScienceRama MurthyNo ratings yet
- Hematology Final ExamDocument20 pagesHematology Final ExamAlon GoldfainerNo ratings yet
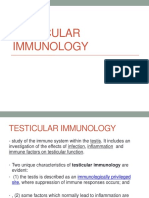
- Testicular ImmunologyDocument28 pagesTesticular Immunologytheodore nottNo ratings yet
- UrosepsisDocument6 pagesUrosepsisParama AdhikresnaNo ratings yet
- Technical Brief and Priority Action On OmicronDocument8 pagesTechnical Brief and Priority Action On OmicronABC Action NewsNo ratings yet
- Active Hexose Correlated Compound - Wikipedia, The Free EncyclopediaDocument7 pagesActive Hexose Correlated Compound - Wikipedia, The Free EncyclopedianurpeekNo ratings yet
- Immunization - When Should It Start?: Child Vaccination ScheduleDocument2 pagesImmunization - When Should It Start?: Child Vaccination SchedulenitinNo ratings yet
- 2.2.5.3 Limadenitis Akut Dan KronisDocument21 pages2.2.5.3 Limadenitis Akut Dan KronisFaizah Ashyfa RahmanNo ratings yet
- DIT 2010 Content IndexDocument2 pagesDIT 2010 Content Indexmone2222No ratings yet
- PNLE: Community Health Nursing Exam 5 - RNpediaDocument13 pagesPNLE: Community Health Nursing Exam 5 - RNpediaLot RositNo ratings yet
- LEC 1 Microbiology Intro and Hx. Lec 1Document62 pagesLEC 1 Microbiology Intro and Hx. Lec 1nicewanNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsWan Norhayati Wan Abdul GhaniNo ratings yet
- Chapter 19Document16 pagesChapter 19missy23pap100% (1)
- Blood Grouping Presentation 4Document13 pagesBlood Grouping Presentation 4Aisha ShahfiqueeNo ratings yet
- Testing For Tuberculosis (TB) : Tuberculin Skin Test (TST)Document2 pagesTesting For Tuberculosis (TB) : Tuberculin Skin Test (TST)Aluh L DiniNo ratings yet
- Revision Microbiology - EditedDocument14 pagesRevision Microbiology - EditedAzmyza AzmyNo ratings yet
- Campylobacter JejuniDocument4 pagesCampylobacter JejuniAgnieszkaNo ratings yet
- Bacterial Infections of The Gastrointestinal Tract: Rey Mark P. Gamiao Teacher: Mr. Jayson TojinoDocument2 pagesBacterial Infections of The Gastrointestinal Tract: Rey Mark P. Gamiao Teacher: Mr. Jayson TojinoJoharie EncaNo ratings yet
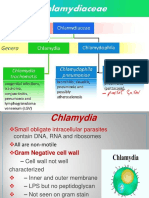
- Chlamydia&Rickettsia 2023Document29 pagesChlamydia&Rickettsia 2023Alhassn NasserNo ratings yet
- BACTERIAL-MENINGITISDocument2 pagesBACTERIAL-MENINGITISDaniela Nicole Manibog ValentinoNo ratings yet
- Community II UpDocument17 pagesCommunity II Upkuruvagadda sagarNo ratings yet
- TuberculosisDocument16 pagesTuberculosisdilsharakaviNo ratings yet
- Vasculitis in ChildrenDocument22 pagesVasculitis in ChildrenRashed ShatnawiNo ratings yet
- Health Myocarditis and Pericarditis Following CovidDocument6 pagesHealth Myocarditis and Pericarditis Following CovidHenny TantonoNo ratings yet
- BP InggrisDocument5 pagesBP InggrisJe'ii PadillaNo ratings yet