Download as pdf or txt
You might also like
- Olympus CLV s190 ManualDocument40 pagesOlympus CLV s190 ManualPolo RaztecaNo ratings yet
- Health Insurance Notes: Done By: Mohamed Arash (2020)Document18 pagesHealth Insurance Notes: Done By: Mohamed Arash (2020)Jag ProductionsNo ratings yet
- AntacidsDocument14 pagesAntacidsjakubstefanoNo ratings yet
- LWUA PrimerDocument5 pagesLWUA Primeralbinoski20053388No ratings yet
- Glenmark Pharmaceuticals Limited: Analytical Research Laboratory (Formulation), TalojaDocument5 pagesGlenmark Pharmaceuticals Limited: Analytical Research Laboratory (Formulation), Talojaरोहित जोशीNo ratings yet
- Comparative Effectiviness of Bariatric Procedures 2016Document19 pagesComparative Effectiviness of Bariatric Procedures 2016MDDberlyYnguaNo ratings yet
- Revisional Bariatric Surgery: Who, What, Where, and When?Document8 pagesRevisional Bariatric Surgery: Who, What, Where, and When?SiMo AL-WadaniNo ratings yet
- Ibele 2011Document5 pagesIbele 2011Alain GarcíaNo ratings yet
- 13 - 2017 - Nutritional Recommendations For Adult BariatricDocument13 pages13 - 2017 - Nutritional Recommendations For Adult Bariatricvictor eduardoNo ratings yet
- Leroux 2018Document18 pagesLeroux 2018bread maniacNo ratings yet
- Weight Regain After RYGBDocument9 pagesWeight Regain After RYGBSorin Niky MocanuNo ratings yet
- Accepted Manuscript: 10.1016/j.cgh.2015.12.030Document17 pagesAccepted Manuscript: 10.1016/j.cgh.2015.12.030lourdes marquezNo ratings yet
- Iron de Ficiency After Bariatric Surgery: What Is The Real Problem?Document11 pagesIron de Ficiency After Bariatric Surgery: What Is The Real Problem?NAYARA CAETANONo ratings yet
- Diarrhea After Bariatric Procedures: Diagnosis and TherapyDocument13 pagesDiarrhea After Bariatric Procedures: Diagnosis and TherapyAndrei SarmientoNo ratings yet
- Exercise and Bariatric SurgeryDocument9 pagesExercise and Bariatric SurgeryDusan OrescaninNo ratings yet
- Jurnal DindaDocument6 pagesJurnal Dindachiendo ymNo ratings yet
- Psychological Assessment For Bariatric Surgery: Current PracticesDocument4 pagesPsychological Assessment For Bariatric Surgery: Current PracticesLauraNo ratings yet
- Ruth 2013Document17 pagesRuth 2013Paul SimononNo ratings yet
- Modifiable Factors Associated With Weight Regain After Bariatric Surgery A Scoping ReviewDocument22 pagesModifiable Factors Associated With Weight Regain After Bariatric Surgery A Scoping Reviewc.eduardoNo ratings yet
- Jurnal ArafahDocument6 pagesJurnal ArafahAnonymous u0Fjt3No ratings yet
- Laparoscopic Roux-en-Y Gastric Bypass: 10-Year Follow-UpDocument10 pagesLaparoscopic Roux-en-Y Gastric Bypass: 10-Year Follow-UpAndrei SarmientoNo ratings yet
- Puzziferri Et Al., 2014 - BS Long TermDocument19 pagesPuzziferri Et Al., 2014 - BS Long TermJulia SCNo ratings yet
- Jejunoileal Shunt in Surgical Treatment of Morbid ObesityDocument11 pagesJejunoileal Shunt in Surgical Treatment of Morbid ObesityTiago VieiraNo ratings yet
- AACE TOS ASMBS Clinical Practice Guidlines 3.2013 PDFDocument33 pagesAACE TOS ASMBS Clinical Practice Guidlines 3.2013 PDFJorge MariaNo ratings yet
- Vol. 229, No. 4S2, October 2019 Scientific Poster Presentations E69Document2 pagesVol. 229, No. 4S2, October 2019 Scientific Poster Presentations E69Mateo TamayoNo ratings yet
- Conditioning Chemotherapy Dose Adjustmentin Obesepatients Bubalo BBMT2014Document18 pagesConditioning Chemotherapy Dose Adjustmentin Obesepatients Bubalo BBMT2014Giang Dinh NguyenNo ratings yet
- Study 2Document7 pagesStudy 2angelrullNo ratings yet
- Obesidad y PsiquiatriaDocument6 pagesObesidad y PsiquiatriaRoberto Alexis Molina CampuzanoNo ratings yet
- Artigo TX Bia 2011Document5 pagesArtigo TX Bia 2011gutorpNo ratings yet
- Impact On Mid Term Health Related Quality of Life After Duodenal Switch: A Systematic Review and Meta AnalysisDocument11 pagesImpact On Mid Term Health Related Quality of Life After Duodenal Switch: A Systematic Review and Meta AnalysisTan BulNo ratings yet
- Ligibel JA Et Al. 2022 Exercise, Diet and Weight Management During Cancer Treatment - ASCO GuidelineDocument20 pagesLigibel JA Et Al. 2022 Exercise, Diet and Weight Management During Cancer Treatment - ASCO GuidelineJasmyn KimNo ratings yet
- Radiol 2019182354Document9 pagesRadiol 2019182354Adarsh GhoshNo ratings yet
- The ASMBS Textbook of Bariatric Surgery: Volume 1: Bariatric SurgeryFrom EverandThe ASMBS Textbook of Bariatric Surgery: Volume 1: Bariatric SurgeryNo ratings yet
- Wolfe Et Al., 2016 - BSDocument23 pagesWolfe Et Al., 2016 - BSJulia SCNo ratings yet
- Graessler 2012Document9 pagesGraessler 2012dora guzmanNo ratings yet
- Does Sleeve Shape Make A Difference in Outcomes?Document7 pagesDoes Sleeve Shape Make A Difference in Outcomes?JOTACENo ratings yet
- Arribas 2017Document8 pagesArribas 2017anajessicanutricionistaNo ratings yet
- Management of Lifestyle Factors in Individuals With Cirrhosis: A Pragmatic ReviewDocument9 pagesManagement of Lifestyle Factors in Individuals With Cirrhosis: A Pragmatic ReviewsavitageraNo ratings yet
- SMN012 01 01 PDFDocument6 pagesSMN012 01 01 PDFvaloranthakam10No ratings yet
- 2 Can Exercise Promote Additional Benefits On Body CompositionDocument23 pages2 Can Exercise Promote Additional Benefits On Body CompositionJuan Luis RuizNo ratings yet
- Effects of A Meal Replacement On Body CompositionDocument10 pagesEffects of A Meal Replacement On Body CompositionGiffariNo ratings yet
- Weight Recid. Paper Obes Surg 2016 (Published E-Offprint)Document7 pagesWeight Recid. Paper Obes Surg 2016 (Published E-Offprint)AymanNo ratings yet
- 2018 Article 892-Dy7nDocument12 pages2018 Article 892-Dy7nCaroline Ruffo FogassaNo ratings yet
- Practiceguidelines: Received: 4 May 2017 Accepted: 22 May 2017 DOI: 10.1002/hed.24866Document7 pagesPracticeguidelines: Received: 4 May 2017 Accepted: 22 May 2017 DOI: 10.1002/hed.24866MdacNo ratings yet
- 2452 4549 Revistacirugia 75 05 0368Document11 pages2452 4549 Revistacirugia 75 05 0368p.espindola.ramirezNo ratings yet
- Predictive Factors of Weight Regain Following Laparoscopic Rouxen-Y Gastric BypassDocument7 pagesPredictive Factors of Weight Regain Following Laparoscopic Rouxen-Y Gastric BypassLuis RodriguezNo ratings yet
- Lepto Spiros IsDocument11 pagesLepto Spiros IsRana RaydianNo ratings yet
- 02 ASMBS & AHS Consensus Guidelines On Bariatric Surgery & Hernia SurgeryDocument12 pages02 ASMBS & AHS Consensus Guidelines On Bariatric Surgery & Hernia SurgeryRony RonyNo ratings yet
- Gastroesophagealreflux Diseaseafterbariatric Procedures: Maria S. Altieri,, Aurora D. PryorDocument13 pagesGastroesophagealreflux Diseaseafterbariatric Procedures: Maria S. Altieri,, Aurora D. PryormaryNo ratings yet
- LSG Vs LGB Vs RYGBDocument7 pagesLSG Vs LGB Vs RYGBRadu MiricaNo ratings yet
- Outcomes, Satiety, and Adverse Upper Gastrointestinal Symptoms Following Laparoscopic Adjustable Gastric BandingDocument8 pagesOutcomes, Satiety, and Adverse Upper Gastrointestinal Symptoms Following Laparoscopic Adjustable Gastric BandingAna Claudia AndradeNo ratings yet
- Brief, Four-Session Group CBT Reduces Binge Eating Behaviors Among Bariatric Surgery CandidatesDocument6 pagesBrief, Four-Session Group CBT Reduces Binge Eating Behaviors Among Bariatric Surgery CandidatesRoberto Cabrera TorresNo ratings yet
- JCSM 8 437Document10 pagesJCSM 8 437anggi larasatiNo ratings yet
- SJV 008Document16 pagesSJV 008Cynthia Denisse González LópezNo ratings yet
- NIH Public Access: Author ManuscriptDocument14 pagesNIH Public Access: Author ManuscriptKarina UtariNo ratings yet
- Nutritional Pyramid For Post-Gastric Bypass Patients: Current StatusDocument9 pagesNutritional Pyramid For Post-Gastric Bypass Patients: Current StatusvcaguiarNo ratings yet
- 14 Disordered Eating After Bariatric Surgery Clinical Aspects - Maggi ORDocument10 pages14 Disordered Eating After Bariatric Surgery Clinical Aspects - Maggi ORFrancisco MtzNo ratings yet
- Sleeve Gastrectomy - A Potential Successor To The Lap RYGB?Document30 pagesSleeve Gastrectomy - A Potential Successor To The Lap RYGB?John LiuNo ratings yet
- Waist Circumference and Cardiometabolic Risk: S K, D B. A, S B. H, D E. K, R L. L, C N, R KDocument6 pagesWaist Circumference and Cardiometabolic Risk: S K, D B. A, S B. H, D E. K, R L. L, C N, R KJoni WitziNo ratings yet
- Endoscopic Sleeve Gastroplasty As An Early Tool Against Obesity: A Multicenter International Study On An Overweight PopulationDocument6 pagesEndoscopic Sleeve Gastroplasty As An Early Tool Against Obesity: A Multicenter International Study On An Overweight PopulationduranaxelNo ratings yet
- Revisional Bariatric Surgery Due To Complications Indications and OutcomesDocument10 pagesRevisional Bariatric Surgery Due To Complications Indications and Outcomesnatty yumi22No ratings yet
- Clinical Nutritional Assessment Methods and Their Progress in Hepatocellular Carcinoma PatientsDocument4 pagesClinical Nutritional Assessment Methods and Their Progress in Hepatocellular Carcinoma PatientsPaul HartingNo ratings yet
- Patient SummaryDocument1 pagePatient Summaryapi-265063071No ratings yet
- RFH - NPT Borhofen2016Document9 pagesRFH - NPT Borhofen2016pamela UrrutiaNo ratings yet
- Abdominal Massage May Decrease Gastric Residual Volumes and Abdominal Circumference in Critically Ill PatientsDocument2 pagesAbdominal Massage May Decrease Gastric Residual Volumes and Abdominal Circumference in Critically Ill PatientsDiah PermatasariNo ratings yet
- Activated Charcoal For Acute OverdoseDocument6 pagesActivated Charcoal For Acute OverdoseTony ChuNo ratings yet
- English Test - 11 Form Level VIIDocument4 pagesEnglish Test - 11 Form Level VIIsofiaNo ratings yet
- 671 2916 1 PB1Document5 pages671 2916 1 PB1Dr. Ziad AlabdallahNo ratings yet
- Gas Valves Interstage Pressure Between SRV and GCV high-SEP10 PDFDocument4 pagesGas Valves Interstage Pressure Between SRV and GCV high-SEP10 PDFsanjeevchhabraNo ratings yet
- Jhs 800s Service Manual (3rd)Document172 pagesJhs 800s Service Manual (3rd)492rvtpzgsNo ratings yet
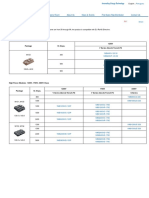
- IGBT Modules 1-Pack Fuji Electric AmericaDocument1 pageIGBT Modules 1-Pack Fuji Electric AmericaSergio MuriloNo ratings yet
- Mobility Training For The Young AthleteDocument8 pagesMobility Training For The Young AthletePedro GouveiaNo ratings yet
- Price List E-Catalog Docare 2023Document2 pagesPrice List E-Catalog Docare 2023PT. Aditya FarmatamaNo ratings yet
- Phil.. Cartoon'sDocument17 pagesPhil.. Cartoon'sKaye Anthonette VedadNo ratings yet
- Preliminary Report - NCAL PDFDocument21 pagesPreliminary Report - NCAL PDFRecordTrac - City of OaklandNo ratings yet
- Perbandingan Harga Apotek Vs PBFDocument3 pagesPerbandingan Harga Apotek Vs PBFRidho SaputraNo ratings yet
- Nervous SystemDocument55 pagesNervous SystemRhesa SesucaNo ratings yet
- Technical Query: Ajaokuta Kaduna Kano Gas Pipeline ProjectDocument4 pagesTechnical Query: Ajaokuta Kaduna Kano Gas Pipeline ProjectArunNo ratings yet
- Clv2050 Masterplan PDFDocument268 pagesClv2050 Masterplan PDFZNo ratings yet
- Sea Water Corrosion Resisting SteelDocument8 pagesSea Water Corrosion Resisting SteelCarlos PadillaNo ratings yet
- STI SP001 - SP031 Repairs 5th Edition GuidelinesDocument33 pagesSTI SP001 - SP031 Repairs 5th Edition GuidelinesJade Geronimo80% (5)
- TCM Course Holland 2019-2020Document88 pagesTCM Course Holland 2019-2020Alejandra Guerrero100% (1)
- List of Best NGOs in Hyderabad - Genuine Charitable OrganisationsDocument3 pagesList of Best NGOs in Hyderabad - Genuine Charitable OrganisationsKataboina HariCharanNo ratings yet
- HyponatremiaDocument40 pagesHyponatremiaarchana p sNo ratings yet
- Final Exam Cookery Nc2Document3 pagesFinal Exam Cookery Nc2rhodefrancestuazon100% (1)
- Sort and Remove Unnecessary ItemsDocument4 pagesSort and Remove Unnecessary ItemsAnthony GozoNo ratings yet
- Qur'an and The BrainDocument7 pagesQur'an and The BrainFatin Farhana RahamanNo ratings yet
- T24 ACM ManualDocument9 pagesT24 ACM ManualabnicolescuNo ratings yet
- Hyde Park Ultrasonic Sensors - VM1PNOQDocument2 pagesHyde Park Ultrasonic Sensors - VM1PNOQKharlaSotoNo ratings yet
- Microcontroller Based Heart Rate Monitor: Sharanabasappa Sali, Pooja Durge, Monika Pokar, Namrata KasgeDocument4 pagesMicrocontroller Based Heart Rate Monitor: Sharanabasappa Sali, Pooja Durge, Monika Pokar, Namrata Kasgemahavarun3096No ratings yet