
Geriatric Nursing
Geriatric Nursing
You might also like
- Jaws - The Story of A Hidden EpidemicDocument13 pagesJaws - The Story of A Hidden EpidemicrudraNo ratings yet
- Gateway B2 Test 6B 1-3 PDFDocument3 pagesGateway B2 Test 6B 1-3 PDFlourdes67% (3)
- Mayo Clinic on Better Hearing and Balance: Strategies to Restore Hearing, Manage Dizziness and Much MoreFrom EverandMayo Clinic on Better Hearing and Balance: Strategies to Restore Hearing, Manage Dizziness and Much MoreNo ratings yet
- Age and Hearing Health, The Life Course ApproachDocument12 pagesAge and Hearing Health, The Life Course ApproachDerwin CahyadiNo ratings yet
- Sataloff Chs 6-11 - 2Document79 pagesSataloff Chs 6-11 - 2Dwiki GumelarNo ratings yet
- Hearing Loss in The ElderlyDocument12 pagesHearing Loss in The ElderlyPaola C. Diaz CruzNo ratings yet
- Dailey Formal Writing 1Document11 pagesDailey Formal Writing 1api-314770661No ratings yet
- Hearing Loss and Depression in Older Adults A Systematic Review and Meta AnalysisDocument18 pagesHearing Loss and Depression in Older Adults A Systematic Review and Meta Analysisnajibhibatullah50No ratings yet
- The Circle of Care For Older Adults With Hearing Loss and Comorbidities: A Case Study of A Geriatric Audiology ClinicDocument21 pagesThe Circle of Care For Older Adults With Hearing Loss and Comorbidities: A Case Study of A Geriatric Audiology ClinicAbYy Aravena CruzNo ratings yet
- Presbycusis: Sang Hoon Kim, Seung Geun YeoDocument6 pagesPresbycusis: Sang Hoon Kim, Seung Geun YeoLuluk AisyahNo ratings yet
- DD PresbikusisDocument3 pagesDD PresbikusisJ KrystalNo ratings yet
- Hearingloss: The Silent Risk For Psychiatric Disorders in Late LifeDocument9 pagesHearingloss: The Silent Risk For Psychiatric Disorders in Late LifeDhino Armand Quispe SánchezNo ratings yet
- Hearing LossDocument21 pagesHearing LossErsya MuslihNo ratings yet
- Geriatric Otolaryngology Author Hinrich StaeckerDocument22 pagesGeriatric Otolaryngology Author Hinrich StaeckerSHERIF ZAHERNo ratings yet
- A Holistic ApproachDocument13 pagesA Holistic ApproachsepthyaniNo ratings yet
- Rehab AnswerDocument8 pagesRehab AnswerFardeen RafiqueNo ratings yet
- Kwame Nkrumah University of Science and Technology: College of Health Sciences School of Medical SciencesDocument25 pagesKwame Nkrumah University of Science and Technology: College of Health Sciences School of Medical SciencesEmmanuel DanquahNo ratings yet
- Voicedisordersinthe Elderly: Karen M. Kost,, Robert T. SataloffDocument13 pagesVoicedisordersinthe Elderly: Karen M. Kost,, Robert T. SataloffFernanda MerichesNo ratings yet
- GOTB - Group 7 - Geriatric WorldDocument3 pagesGOTB - Group 7 - Geriatric WorldReza Afif FebriansyahNo ratings yet
- Cerebral Palsy and The Effects On The Oral Cavity: Jessica Heberlie Dhyg Iv - L. HeblDocument7 pagesCerebral Palsy and The Effects On The Oral Cavity: Jessica Heberlie Dhyg Iv - L. Heblapi-546773895No ratings yet
- Approach To Hearing LossDocument7 pagesApproach To Hearing LossAlexandros GidarakosNo ratings yet
- 02 Review PDFDocument10 pages02 Review PDFDanan LaksetyaNo ratings yet
- Pérdida Auditiva y Uso de Los Servicios de Salud Un Estudio Transversal de Base Poblacional Entre Adultos Mayores FinlandesesDocument11 pagesPérdida Auditiva y Uso de Los Servicios de Salud Un Estudio Transversal de Base Poblacional Entre Adultos Mayores FinlandesesMARTIN NICOLAS MORA STAGNONo ratings yet
- Swanepoel Telehealth (2010) PDFDocument24 pagesSwanepoel Telehealth (2010) PDFRoberta VianaNo ratings yet
- The Aging Voice: Presented by Anastasia Serbalik Presented To Rebecca L. Gould, MSC, CCC-SLPDocument32 pagesThe Aging Voice: Presented by Anastasia Serbalik Presented To Rebecca L. Gould, MSC, CCC-SLPAtri AmmuluNo ratings yet
- 114 Barera CsDocument15 pages114 Barera Cskaloydiaz09No ratings yet
- AphasiaDocument28 pagesAphasiaEmilio Emmanué Escobar CruzNo ratings yet
- Dapus 9 Referat 1Document6 pagesDapus 9 Referat 1Akramanto RidwanNo ratings yet
- Recent Advancements in The Regeneration of Auditory Hair Cells and Hearing RestorationDocument16 pagesRecent Advancements in The Regeneration of Auditory Hair Cells and Hearing RestorationRana Sabouni TabariNo ratings yet
- 2021 - Aja 21 00006 3Document14 pages2021 - Aja 21 00006 3Melissa MorenoNo ratings yet
- High-Frequency Audiometry For Early Detection of Hearing Loss: A Narrative ReviewDocument13 pagesHigh-Frequency Audiometry For Early Detection of Hearing Loss: A Narrative ReviewJennifer ArévaloNo ratings yet
- Presbycusi S: By: April Fischer CSD 771 Case StudyDocument26 pagesPresbycusi S: By: April Fischer CSD 771 Case Studyminal madcapNo ratings yet
- Presbycusis JournalDocument11 pagesPresbycusis JournalJairah CandaoNo ratings yet
- Medicina: The Importance of Early Genetic Diagnostics of Hearing Loss in ChildrenDocument13 pagesMedicina: The Importance of Early Genetic Diagnostics of Hearing Loss in ChildrenAsniar RNo ratings yet
- Hearing Aid For AdultsDocument25 pagesHearing Aid For Adultssathsh kumarNo ratings yet
- Kasus PresbycusDocument29 pagesKasus PresbycusSMA N 1 TOROHNo ratings yet
- Current Concepts: Review ArticleDocument7 pagesCurrent Concepts: Review ArticleMia Mia MiaNo ratings yet
- Dementia Assignment 2022 Podcast Script FinalDocument4 pagesDementia Assignment 2022 Podcast Script Finalindraneel570No ratings yet
- Otosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOtosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- What Is PresbycusisDocument4 pagesWhat Is PresbycusisNisa UcilNo ratings yet
- Article and Reflection Care of Older AdultDocument1 pageArticle and Reflection Care of Older AdultSHAMAE FAITH FARRENNo ratings yet
- SJ BDJ 2008 850Document13 pagesSJ BDJ 2008 850Mostafa FayadNo ratings yet
- Ijsrp p1486Document6 pagesIjsrp p1486Sandeep KumarNo ratings yet
- Geriatric Health Paper Copy 2Document7 pagesGeriatric Health Paper Copy 2api-400900026No ratings yet
- Kja 17 45 PDFDocument5 pagesKja 17 45 PDFAgnice SimanjuntakNo ratings yet
- Cause and Effect of BruxismDocument3 pagesCause and Effect of BruxismEnrica Melissa PanjaitanNo ratings yet
- Hearing Loss and Psychiatric DisordersDocument1 pageHearing Loss and Psychiatric Disordersapi-655240427No ratings yet
- Turning Down The Noise - The Benefit of Musical Training On The Aging Auditory BrainDocument12 pagesTurning Down The Noise - The Benefit of Musical Training On The Aging Auditory BrainJeanYanNo ratings yet
- Meniere's Disease and Tinnitus in Nursing PractiseDocument5 pagesMeniere's Disease and Tinnitus in Nursing PractiseLizbeth MarinahNo ratings yet
- PIIS0896627320306103Document12 pagesPIIS0896627320306103gabriel.lps2608No ratings yet
- Deaf Mute PaperDocument11 pagesDeaf Mute PaperneviNo ratings yet
- Part C.3 and AnsDocument10 pagesPart C.3 and AnsKhang VõNo ratings yet
- Reflection FinalDocument10 pagesReflection FinalRichardTangNo ratings yet
- CURRENT Diagnosis & Treatment in Otolaryngology-Head & Neck Surgery, 3eDocument3 pagesCURRENT Diagnosis & Treatment in Otolaryngology-Head & Neck Surgery, 3eStephanie Vania EmbangNo ratings yet
- Tinnitus 2019Document20 pagesTinnitus 2019Leslie Lindsay AlvarezNo ratings yet
- Amplification: The Treatment of Choice For Presbycusis: Eye & Ear DiseasesDocument3 pagesAmplification: The Treatment of Choice For Presbycusis: Eye & Ear DiseasesAyu Putri Firda NNo ratings yet
- DTSCH Arztebl Int-117 0690Document12 pagesDTSCH Arztebl Int-117 0690CoAsst MuhammadNuhAlhudawyNo ratings yet
- Presbyphoniaandminimal Glotticinsufficiency: David E. Rosow,, Debbie R. PanDocument9 pagesPresbyphoniaandminimal Glotticinsufficiency: David E. Rosow,, Debbie R. PanANA CRISTINA MENDEZ DIAZNo ratings yet
- Noise Induced Hearing Loss: Could Easily Be PreventedDocument1 pageNoise Induced Hearing Loss: Could Easily Be PreventedHidayadNo ratings yet
- Research Proposal First Draft (Adamu Moti)Document25 pagesResearch Proposal First Draft (Adamu Moti)ODAA TUBENo ratings yet
- Tacrolimus in DermatologyDocument4 pagesTacrolimus in DermatologyDimas PrajagoptaNo ratings yet
- Sheet - Respiratory ExaminationDocument11 pagesSheet - Respiratory ExaminationbakesamiNo ratings yet
- Lapsus Fraktur Neck FemurDocument32 pagesLapsus Fraktur Neck FemurZóélkårnåín PhåntómhívéNo ratings yet
- Surgical Hip Dislocation Is More Powerful Than Arthro - 2019 - Orthopaedics - TRDocument6 pagesSurgical Hip Dislocation Is More Powerful Than Arthro - 2019 - Orthopaedics - TRIuliana MoiseNo ratings yet
- Hsu Et Al 2014 - ArticleDocument10 pagesHsu Et Al 2014 - ArticleBishara WilsonNo ratings yet
- Quick Guide For OTs People Recovering From COVID-19Document17 pagesQuick Guide For OTs People Recovering From COVID-19Mihaela SerbanNo ratings yet
- Immunology Notes From Uworld, DR-KYDocument16 pagesImmunology Notes From Uworld, DR-KYLayan MohammadNo ratings yet
- Q3 S10 Week 1 Lecture or NotesDocument5 pagesQ3 S10 Week 1 Lecture or NotesJuben OdalNo ratings yet
- Drug Study and LaboratoryDocument13 pagesDrug Study and LaboratoryGEOMHAI CATBAGANNo ratings yet
- Fnut 09 1063510Document15 pagesFnut 09 1063510PriawanIndraNo ratings yet
- HormonesDocument25 pagesHormonesapi-309893409No ratings yet
- Marcella Kennedy Curriculum VitaeDocument3 pagesMarcella Kennedy Curriculum Vitaemarcikennedy1010No ratings yet
- Teleconference 23 Juli 2019Document11 pagesTeleconference 23 Juli 2019Vita DesriantiNo ratings yet
- Nervous System ProformaDocument10 pagesNervous System ProformaEBNo ratings yet
- Notice: Meetings: Recognized Standards List Modifications (Recognition List Number 018)Document12 pagesNotice: Meetings: Recognized Standards List Modifications (Recognition List Number 018)Justia.comNo ratings yet
- Plastic Surgery - Taboo TopicsDocument2 pagesPlastic Surgery - Taboo TopicsSahil MohammadNo ratings yet
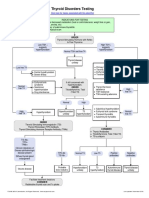
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmRezi HelperNo ratings yet
- NCP FinalDocument6 pagesNCP FinalWanwan PraybeytNo ratings yet
- SDCEP MADP Consultation DraftDocument58 pagesSDCEP MADP Consultation DraftLisa Pramitha SNo ratings yet
- English Final CoursDocument223 pagesEnglish Final CourspopeataNo ratings yet
- Neurovascular Interactions in Dental PulpDocument6 pagesNeurovascular Interactions in Dental PulpSaraMAminNo ratings yet
- Low Back PainDocument17 pagesLow Back PainRamon Salinas AguileraNo ratings yet
- Pancreatic Cancer Early Detection, Diagnosis, and StagingDocument29 pagesPancreatic Cancer Early Detection, Diagnosis, and StagingDokter LinggauNo ratings yet
- Daftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10Document10 pagesDaftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10kartianiNo ratings yet
- Product Catalogue Diagnostic Systems 2014Document197 pagesProduct Catalogue Diagnostic Systems 2014DJNo ratings yet
- HEALTH K 12 Curriculum GuideDocument47 pagesHEALTH K 12 Curriculum GuideMarcia Cristina A. LopezNo ratings yet
- Rcsi Mini Med ProgrammeDocument1 pageRcsi Mini Med Programmeapi-531313826No ratings yet
- Treating Canine Distemper VirusDocument23 pagesTreating Canine Distemper VirusJack HollandNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- Jaws - The Story of A Hidden EpidemicDocument13 pagesJaws - The Story of A Hidden EpidemicrudraNo ratings yet
- Gateway B2 Test 6B 1-3 PDFDocument3 pagesGateway B2 Test 6B 1-3 PDFlourdes67% (3)
- Mayo Clinic on Better Hearing and Balance: Strategies to Restore Hearing, Manage Dizziness and Much MoreFrom EverandMayo Clinic on Better Hearing and Balance: Strategies to Restore Hearing, Manage Dizziness and Much MoreNo ratings yet
- Age and Hearing Health, The Life Course ApproachDocument12 pagesAge and Hearing Health, The Life Course ApproachDerwin CahyadiNo ratings yet
- Sataloff Chs 6-11 - 2Document79 pagesSataloff Chs 6-11 - 2Dwiki GumelarNo ratings yet
- Hearing Loss in The ElderlyDocument12 pagesHearing Loss in The ElderlyPaola C. Diaz CruzNo ratings yet
- Dailey Formal Writing 1Document11 pagesDailey Formal Writing 1api-314770661No ratings yet
- Hearing Loss and Depression in Older Adults A Systematic Review and Meta AnalysisDocument18 pagesHearing Loss and Depression in Older Adults A Systematic Review and Meta Analysisnajibhibatullah50No ratings yet
- The Circle of Care For Older Adults With Hearing Loss and Comorbidities: A Case Study of A Geriatric Audiology ClinicDocument21 pagesThe Circle of Care For Older Adults With Hearing Loss and Comorbidities: A Case Study of A Geriatric Audiology ClinicAbYy Aravena CruzNo ratings yet
- Presbycusis: Sang Hoon Kim, Seung Geun YeoDocument6 pagesPresbycusis: Sang Hoon Kim, Seung Geun YeoLuluk AisyahNo ratings yet
- DD PresbikusisDocument3 pagesDD PresbikusisJ KrystalNo ratings yet
- Hearingloss: The Silent Risk For Psychiatric Disorders in Late LifeDocument9 pagesHearingloss: The Silent Risk For Psychiatric Disorders in Late LifeDhino Armand Quispe SánchezNo ratings yet
- Hearing LossDocument21 pagesHearing LossErsya MuslihNo ratings yet
- Geriatric Otolaryngology Author Hinrich StaeckerDocument22 pagesGeriatric Otolaryngology Author Hinrich StaeckerSHERIF ZAHERNo ratings yet
- A Holistic ApproachDocument13 pagesA Holistic ApproachsepthyaniNo ratings yet
- Rehab AnswerDocument8 pagesRehab AnswerFardeen RafiqueNo ratings yet
- Kwame Nkrumah University of Science and Technology: College of Health Sciences School of Medical SciencesDocument25 pagesKwame Nkrumah University of Science and Technology: College of Health Sciences School of Medical SciencesEmmanuel DanquahNo ratings yet
- Voicedisordersinthe Elderly: Karen M. Kost,, Robert T. SataloffDocument13 pagesVoicedisordersinthe Elderly: Karen M. Kost,, Robert T. SataloffFernanda MerichesNo ratings yet
- GOTB - Group 7 - Geriatric WorldDocument3 pagesGOTB - Group 7 - Geriatric WorldReza Afif FebriansyahNo ratings yet
- Cerebral Palsy and The Effects On The Oral Cavity: Jessica Heberlie Dhyg Iv - L. HeblDocument7 pagesCerebral Palsy and The Effects On The Oral Cavity: Jessica Heberlie Dhyg Iv - L. Heblapi-546773895No ratings yet
- Approach To Hearing LossDocument7 pagesApproach To Hearing LossAlexandros GidarakosNo ratings yet
- 02 Review PDFDocument10 pages02 Review PDFDanan LaksetyaNo ratings yet
- Pérdida Auditiva y Uso de Los Servicios de Salud Un Estudio Transversal de Base Poblacional Entre Adultos Mayores FinlandesesDocument11 pagesPérdida Auditiva y Uso de Los Servicios de Salud Un Estudio Transversal de Base Poblacional Entre Adultos Mayores FinlandesesMARTIN NICOLAS MORA STAGNONo ratings yet
- Swanepoel Telehealth (2010) PDFDocument24 pagesSwanepoel Telehealth (2010) PDFRoberta VianaNo ratings yet
- The Aging Voice: Presented by Anastasia Serbalik Presented To Rebecca L. Gould, MSC, CCC-SLPDocument32 pagesThe Aging Voice: Presented by Anastasia Serbalik Presented To Rebecca L. Gould, MSC, CCC-SLPAtri AmmuluNo ratings yet
- 114 Barera CsDocument15 pages114 Barera Cskaloydiaz09No ratings yet
- AphasiaDocument28 pagesAphasiaEmilio Emmanué Escobar CruzNo ratings yet
- Dapus 9 Referat 1Document6 pagesDapus 9 Referat 1Akramanto RidwanNo ratings yet
- Recent Advancements in The Regeneration of Auditory Hair Cells and Hearing RestorationDocument16 pagesRecent Advancements in The Regeneration of Auditory Hair Cells and Hearing RestorationRana Sabouni TabariNo ratings yet
- 2021 - Aja 21 00006 3Document14 pages2021 - Aja 21 00006 3Melissa MorenoNo ratings yet
- High-Frequency Audiometry For Early Detection of Hearing Loss: A Narrative ReviewDocument13 pagesHigh-Frequency Audiometry For Early Detection of Hearing Loss: A Narrative ReviewJennifer ArévaloNo ratings yet
- Presbycusi S: By: April Fischer CSD 771 Case StudyDocument26 pagesPresbycusi S: By: April Fischer CSD 771 Case Studyminal madcapNo ratings yet
- Presbycusis JournalDocument11 pagesPresbycusis JournalJairah CandaoNo ratings yet
- Medicina: The Importance of Early Genetic Diagnostics of Hearing Loss in ChildrenDocument13 pagesMedicina: The Importance of Early Genetic Diagnostics of Hearing Loss in ChildrenAsniar RNo ratings yet
- Hearing Aid For AdultsDocument25 pagesHearing Aid For Adultssathsh kumarNo ratings yet
- Kasus PresbycusDocument29 pagesKasus PresbycusSMA N 1 TOROHNo ratings yet
- Current Concepts: Review ArticleDocument7 pagesCurrent Concepts: Review ArticleMia Mia MiaNo ratings yet
- Dementia Assignment 2022 Podcast Script FinalDocument4 pagesDementia Assignment 2022 Podcast Script Finalindraneel570No ratings yet
- Otosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOtosclerosis, (Thickened Ear Bones) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- What Is PresbycusisDocument4 pagesWhat Is PresbycusisNisa UcilNo ratings yet
- Article and Reflection Care of Older AdultDocument1 pageArticle and Reflection Care of Older AdultSHAMAE FAITH FARRENNo ratings yet
- SJ BDJ 2008 850Document13 pagesSJ BDJ 2008 850Mostafa FayadNo ratings yet
- Ijsrp p1486Document6 pagesIjsrp p1486Sandeep KumarNo ratings yet
- Geriatric Health Paper Copy 2Document7 pagesGeriatric Health Paper Copy 2api-400900026No ratings yet
- Kja 17 45 PDFDocument5 pagesKja 17 45 PDFAgnice SimanjuntakNo ratings yet
- Cause and Effect of BruxismDocument3 pagesCause and Effect of BruxismEnrica Melissa PanjaitanNo ratings yet
- Hearing Loss and Psychiatric DisordersDocument1 pageHearing Loss and Psychiatric Disordersapi-655240427No ratings yet
- Turning Down The Noise - The Benefit of Musical Training On The Aging Auditory BrainDocument12 pagesTurning Down The Noise - The Benefit of Musical Training On The Aging Auditory BrainJeanYanNo ratings yet
- Meniere's Disease and Tinnitus in Nursing PractiseDocument5 pagesMeniere's Disease and Tinnitus in Nursing PractiseLizbeth MarinahNo ratings yet
- PIIS0896627320306103Document12 pagesPIIS0896627320306103gabriel.lps2608No ratings yet
- Deaf Mute PaperDocument11 pagesDeaf Mute PaperneviNo ratings yet
- Part C.3 and AnsDocument10 pagesPart C.3 and AnsKhang VõNo ratings yet
- Reflection FinalDocument10 pagesReflection FinalRichardTangNo ratings yet
- CURRENT Diagnosis & Treatment in Otolaryngology-Head & Neck Surgery, 3eDocument3 pagesCURRENT Diagnosis & Treatment in Otolaryngology-Head & Neck Surgery, 3eStephanie Vania EmbangNo ratings yet
- Tinnitus 2019Document20 pagesTinnitus 2019Leslie Lindsay AlvarezNo ratings yet
- Amplification: The Treatment of Choice For Presbycusis: Eye & Ear DiseasesDocument3 pagesAmplification: The Treatment of Choice For Presbycusis: Eye & Ear DiseasesAyu Putri Firda NNo ratings yet
- DTSCH Arztebl Int-117 0690Document12 pagesDTSCH Arztebl Int-117 0690CoAsst MuhammadNuhAlhudawyNo ratings yet
- Presbyphoniaandminimal Glotticinsufficiency: David E. Rosow,, Debbie R. PanDocument9 pagesPresbyphoniaandminimal Glotticinsufficiency: David E. Rosow,, Debbie R. PanANA CRISTINA MENDEZ DIAZNo ratings yet
- Noise Induced Hearing Loss: Could Easily Be PreventedDocument1 pageNoise Induced Hearing Loss: Could Easily Be PreventedHidayadNo ratings yet
- Research Proposal First Draft (Adamu Moti)Document25 pagesResearch Proposal First Draft (Adamu Moti)ODAA TUBENo ratings yet
- Tacrolimus in DermatologyDocument4 pagesTacrolimus in DermatologyDimas PrajagoptaNo ratings yet
- Sheet - Respiratory ExaminationDocument11 pagesSheet - Respiratory ExaminationbakesamiNo ratings yet
- Lapsus Fraktur Neck FemurDocument32 pagesLapsus Fraktur Neck FemurZóélkårnåín PhåntómhívéNo ratings yet
- Surgical Hip Dislocation Is More Powerful Than Arthro - 2019 - Orthopaedics - TRDocument6 pagesSurgical Hip Dislocation Is More Powerful Than Arthro - 2019 - Orthopaedics - TRIuliana MoiseNo ratings yet
- Hsu Et Al 2014 - ArticleDocument10 pagesHsu Et Al 2014 - ArticleBishara WilsonNo ratings yet
- Quick Guide For OTs People Recovering From COVID-19Document17 pagesQuick Guide For OTs People Recovering From COVID-19Mihaela SerbanNo ratings yet
- Immunology Notes From Uworld, DR-KYDocument16 pagesImmunology Notes From Uworld, DR-KYLayan MohammadNo ratings yet
- Q3 S10 Week 1 Lecture or NotesDocument5 pagesQ3 S10 Week 1 Lecture or NotesJuben OdalNo ratings yet
- Drug Study and LaboratoryDocument13 pagesDrug Study and LaboratoryGEOMHAI CATBAGANNo ratings yet
- Fnut 09 1063510Document15 pagesFnut 09 1063510PriawanIndraNo ratings yet
- HormonesDocument25 pagesHormonesapi-309893409No ratings yet
- Marcella Kennedy Curriculum VitaeDocument3 pagesMarcella Kennedy Curriculum Vitaemarcikennedy1010No ratings yet
- Teleconference 23 Juli 2019Document11 pagesTeleconference 23 Juli 2019Vita DesriantiNo ratings yet
- Nervous System ProformaDocument10 pagesNervous System ProformaEBNo ratings yet
- Notice: Meetings: Recognized Standards List Modifications (Recognition List Number 018)Document12 pagesNotice: Meetings: Recognized Standards List Modifications (Recognition List Number 018)Justia.comNo ratings yet
- Plastic Surgery - Taboo TopicsDocument2 pagesPlastic Surgery - Taboo TopicsSahil MohammadNo ratings yet
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmRezi HelperNo ratings yet
- NCP FinalDocument6 pagesNCP FinalWanwan PraybeytNo ratings yet
- SDCEP MADP Consultation DraftDocument58 pagesSDCEP MADP Consultation DraftLisa Pramitha SNo ratings yet
- English Final CoursDocument223 pagesEnglish Final CourspopeataNo ratings yet
- Neurovascular Interactions in Dental PulpDocument6 pagesNeurovascular Interactions in Dental PulpSaraMAminNo ratings yet
- Low Back PainDocument17 pagesLow Back PainRamon Salinas AguileraNo ratings yet
- Pancreatic Cancer Early Detection, Diagnosis, and StagingDocument29 pagesPancreatic Cancer Early Detection, Diagnosis, and StagingDokter LinggauNo ratings yet
- Daftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10Document10 pagesDaftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10kartianiNo ratings yet
- Product Catalogue Diagnostic Systems 2014Document197 pagesProduct Catalogue Diagnostic Systems 2014DJNo ratings yet
- HEALTH K 12 Curriculum GuideDocument47 pagesHEALTH K 12 Curriculum GuideMarcia Cristina A. LopezNo ratings yet
- Rcsi Mini Med ProgrammeDocument1 pageRcsi Mini Med Programmeapi-531313826No ratings yet
- Treating Canine Distemper VirusDocument23 pagesTreating Canine Distemper VirusJack HollandNo ratings yet