Download as pdf or txt
You might also like
- Understated Dominance - Chapter 1501 To 1540Document114 pagesUnderstated Dominance - Chapter 1501 To 1540voipus12No ratings yet
- Cardiothoracicsurgery McqsDocument352 pagesCardiothoracicsurgery McqsMade Ayu50% (2)
- Lansoprazole For The Prevention of Recurrences of Ulcer Complications From Long-Term Low-Dose Aspirin UseDocument6 pagesLansoprazole For The Prevention of Recurrences of Ulcer Complications From Long-Term Low-Dose Aspirin UseAmalia NandiaNo ratings yet
- Journal of Population Therapeutics & Clinical PharmacologyDocument7 pagesJournal of Population Therapeutics & Clinical PharmacologyEka SetyariniNo ratings yet
- Journal of Population Therapeutics & Clinical PharmacologyDocument6 pagesJournal of Population Therapeutics & Clinical PharmacologyheryanggunNo ratings yet
- Acute Inflammatory: Laparoscopically (Salpingitis)Document7 pagesAcute Inflammatory: Laparoscopically (Salpingitis)Bella Ika LestariNo ratings yet
- Original Research PaperDocument2 pagesOriginal Research Paperيحيى الجبليNo ratings yet
- Artículo 14Document5 pagesArtículo 14Yeid EsquivelNo ratings yet
- Inflammatory: of Ofloxacin The of Laparoscopically DiseaseDocument18 pagesInflammatory: of Ofloxacin The of Laparoscopically DiseaseMuhajir NagallamzNo ratings yet
- Vol24 3-3 PDFDocument7 pagesVol24 3-3 PDFEliasNo ratings yet
- Efficacy of Omeprazole and Amoxicillin With Either Clarithromycin or Metronidazole On Eradication of in Chinese Peptic Ulcer PatientsDocument5 pagesEfficacy of Omeprazole and Amoxicillin With Either Clarithromycin or Metronidazole On Eradication of in Chinese Peptic Ulcer PatientsSyukron MakmunNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofFransisca PekertiNo ratings yet
- Nej Mo A 1507062Document11 pagesNej Mo A 1507062anggiNo ratings yet
- CAP - Risk Factors and TreatmentDocument5 pagesCAP - Risk Factors and Treatmentgrool29rNo ratings yet
- Isoniazid TuberculosisDocument10 pagesIsoniazid TuberculosisAisyah Aftita KamrasyidNo ratings yet
- Ne W Engl and Journal MedicineDocument11 pagesNe W Engl and Journal Medicinea4agarwalNo ratings yet
- Bacteriology and Drug Susceptibility Analysis of PusDocument5 pagesBacteriology and Drug Susceptibility Analysis of PusLuis Miguel Díaz VegaNo ratings yet
- A Prospective Observational Study of Prescribing Patterns in Peptic Ulcer DiseaseDocument40 pagesA Prospective Observational Study of Prescribing Patterns in Peptic Ulcer DiseaseGeet MaanNo ratings yet
- JOURNAL Treating Acute Urinary Tract InfectionsDocument5 pagesJOURNAL Treating Acute Urinary Tract InfectionsKhayelee PalosNo ratings yet
- Anderson01-27-12 Floroquinolone Prophilaxis PDFDocument22 pagesAnderson01-27-12 Floroquinolone Prophilaxis PDFSri WulandahNo ratings yet
- Short-Course Intraabdominal InfectionDocument10 pagesShort-Course Intraabdominal Infectionnicolás idárragaNo ratings yet
- The Role of Antibiotic Prophylaxis in Prevention of Wound Infection After Lichtenstein Open Mesh Repair of Primary Inguinal HerniaDocument7 pagesThe Role of Antibiotic Prophylaxis in Prevention of Wound Infection After Lichtenstein Open Mesh Repair of Primary Inguinal Herniaيحيى الجبليNo ratings yet
- Meningitis 3Document12 pagesMeningitis 3Kelly MuñozNo ratings yet
- Methisoprinol y VPHDocument4 pagesMethisoprinol y VPHAndres Gonzalez Cruz100% (1)
- Dokazano Dejstvo Nigelle Sative (Crnog Kumina) U Eliminaciji Helicobacter PyloriDocument11 pagesDokazano Dejstvo Nigelle Sative (Crnog Kumina) U Eliminaciji Helicobacter PylorirbcollegeNo ratings yet
- Management of The Urologic Sepsis SyndromeDocument10 pagesManagement of The Urologic Sepsis SyndromeNur Syamsiah MNo ratings yet
- Crossm: Efficacy of Doxycycline in The Treatment of SyphilisDocument7 pagesCrossm: Efficacy of Doxycycline in The Treatment of SyphilisHerdian KusumaNo ratings yet
- Atorvastatin Improves Sputum Conversion and Chest X-Ray Severity ScoreDocument6 pagesAtorvastatin Improves Sputum Conversion and Chest X-Ray Severity Scorecharmainemargaret.parreno.medNo ratings yet
- Effectiveness of Antacids Reducing Digestive Patients Treated With Prednisone and PrednisoloneDocument5 pagesEffectiveness of Antacids Reducing Digestive Patients Treated With Prednisone and PrednisoloneSantri Akhir ZamanNo ratings yet
- Abcesele FicatuluiDocument4 pagesAbcesele FicatuluiMihaela AlinaNo ratings yet
- Screenshot 2021-06-19 at 21.33.17Document11 pagesScreenshot 2021-06-19 at 21.33.17bagus aldiNo ratings yet
- Tofacitinib As Induction and Maintenance Therapy For Ulcerative ColitisDocument14 pagesTofacitinib As Induction and Maintenance Therapy For Ulcerative Colitismichal ben meronNo ratings yet
- A Non-Operative Treatment of Perforated Peptic Ulcer: A Prospective Study With 50 CasesDocument4 pagesA Non-Operative Treatment of Perforated Peptic Ulcer: A Prospective Study With 50 CasesSake Cinema21No ratings yet
- Single-Dose Azithromycin Versus Benzathine Benzylpenicillin For Treatment of Yaws in Children in Papua New Guinea: An Open-Label, Non-Inferiority, Randomised TrialDocument7 pagesSingle-Dose Azithromycin Versus Benzathine Benzylpenicillin For Treatment of Yaws in Children in Papua New Guinea: An Open-Label, Non-Inferiority, Randomised TrialOlivia Halim KumalaNo ratings yet
- Real-World Data of Helicobacter Pylori Prevalence, Eradicationregimens, and Antibiotic Resistance in Thailand, 2013-201Document5 pagesReal-World Data of Helicobacter Pylori Prevalence, Eradicationregimens, and Antibiotic Resistance in Thailand, 2013-201andi kulokNo ratings yet
- Tubo-Ovarian Abscess - Contemporary Approach To ManagementDocument9 pagesTubo-Ovarian Abscess - Contemporary Approach To ManagementDanny. JayNo ratings yet
- Jur DingDocument11 pagesJur DingI'am AjhaNo ratings yet
- Azithromycin in Rheumatic FeverDocument4 pagesAzithromycin in Rheumatic Feverhussien abd elwahedNo ratings yet
- Comparative Study On The Efficacy of Non-Steroidal, Steroid and Non-Use Anti Inflammatory in The Treatment of Epidemic ConjungtivitisDocument6 pagesComparative Study On The Efficacy of Non-Steroidal, Steroid and Non-Use Anti Inflammatory in The Treatment of Epidemic ConjungtivitisVisakha VidyadeviNo ratings yet
- EsomeprazoleDocument7 pagesEsomeprazoleSanjay NavaleNo ratings yet
- The Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioDocument7 pagesThe Epidemiology, Antibiotic Resistance and Post-Discharge Course of Peritonsillar Abscesses in London, OntarioMaharaniNo ratings yet
- Rcse9505 345Document4 pagesRcse9505 345Swekshya PandeyNo ratings yet
- Nebul Nacl 3Document7 pagesNebul Nacl 3Arif RSNo ratings yet
- The Clinical Relevance of Microbiology Specimens in Head and Neck Space Infections of Odontogenic OriginDocument3 pagesThe Clinical Relevance of Microbiology Specimens in Head and Neck Space Infections of Odontogenic OriginkaarlaamendezNo ratings yet
- Haron 1989Document8 pagesHaron 1989georgios031No ratings yet
- Corticosteroids For Bacterial Meningitis in Adults in Sub-Saharan AfricaDocument10 pagesCorticosteroids For Bacterial Meningitis in Adults in Sub-Saharan AfricaMutiara KhalishNo ratings yet
- 43 Pukar EtalDocument3 pages43 Pukar EtaleditorijmrhsNo ratings yet
- Helicobacter Pylori Triple Versus Dual Therapy For EradicatingDocument7 pagesHelicobacter Pylori Triple Versus Dual Therapy For EradicatingAna Lívia AzevedoNo ratings yet
- Tugas RCT SenaDocument10 pagesTugas RCT SenaArfad El HabibieNo ratings yet
- Critical Apprisal of A Prospective StudyDocument7 pagesCritical Apprisal of A Prospective StudyVK LabasanNo ratings yet
- Early Use of TIPS in Cirrhosis and Variceal BleedingDocument10 pagesEarly Use of TIPS in Cirrhosis and Variceal Bleedingray liNo ratings yet
- 10 1016@j Bja 2020 05 003Document10 pages10 1016@j Bja 2020 05 003Robert ChristevenNo ratings yet
- Bacterial Tonsillar Microbiota and Antibiogram in Recurrent TonsillitisDocument5 pagesBacterial Tonsillar Microbiota and Antibiogram in Recurrent TonsillitisResianaPutriNo ratings yet
- Management of Perforated Appendicitis in Children: A Decade of Aggressive TreatmentDocument5 pagesManagement of Perforated Appendicitis in Children: A Decade of Aggressive Treatmentapi-308365861No ratings yet
- Enema. Jal. Pancha Bhuta-323Document6 pagesEnema. Jal. Pancha Bhuta-323Shree GaneshNo ratings yet
- Zhu 2017Document3 pagesZhu 2017Muchamad Wisuda RiswantoNo ratings yet
- Trial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionDocument10 pagesTrial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionMeygan CórdovaNo ratings yet
- Analysis of Antibiotics Selection in Patients Undergoing Appendectomy in A Chinese Tertiary Care HospitalDocument5 pagesAnalysis of Antibiotics Selection in Patients Undergoing Appendectomy in A Chinese Tertiary Care HospitalYuanico LiraukaNo ratings yet
- Apendik KoesnadiDocument4 pagesApendik KoesnadiUbay'z DillahNo ratings yet
- RF - Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Treatment UpdateDocument2 pagesRF - Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Treatment Updatedoc.kentoNo ratings yet
- Gulati 2020Document14 pagesGulati 2020Anisha MDNo ratings yet
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Study of Radiographic Features of Renal Osteodystrophy in Chronic Kidney Disease (CKD) and Their Correlation With Clinical and Biochemical ParametersDocument10 pagesStudy of Radiographic Features of Renal Osteodystrophy in Chronic Kidney Disease (CKD) and Their Correlation With Clinical and Biochemical ParametersIJAR JOURNALNo ratings yet
- Reivew On Equine Colic With Special Attention To Its Diagnosis and TreatmentDocument45 pagesReivew On Equine Colic With Special Attention To Its Diagnosis and TreatmentTola dinkuNo ratings yet
- Positive Affect Treatment For Depression and Anxiety Workbook Alicia E Meuret All ChapterDocument67 pagesPositive Affect Treatment For Depression and Anxiety Workbook Alicia E Meuret All Chapterkaren.dixon505100% (9)
- Medical+language+practice+ NotesDocument7 pagesMedical+language+practice+ NotesmanethNo ratings yet
- WORKSHEET 6 Breath Spray PCOS111 PH3Y2 1 LABDocument8 pagesWORKSHEET 6 Breath Spray PCOS111 PH3Y2 1 LABAngelica PaguintoNo ratings yet
- CNS Related DiseasesDocument4 pagesCNS Related DiseasesYzabelle EncoyNo ratings yet
- FULL Download Ebook PDF Health Psychology 10th Edition PDF EbookDocument41 pagesFULL Download Ebook PDF Health Psychology 10th Edition PDF Ebooklawrence.kibbe472100% (44)
- CHN Family Assessment Interview GuideDocument9 pagesCHN Family Assessment Interview GuideBianca Denise RopilaNo ratings yet
- The Cure For All DiseasesDocument888 pagesThe Cure For All Diseasesmihai968100% (1)
- Aily Equirements: Case: Patient With Tuberculosis General Objectives (5pts)Document31 pagesAily Equirements: Case: Patient With Tuberculosis General Objectives (5pts)janna mae patriarcaNo ratings yet
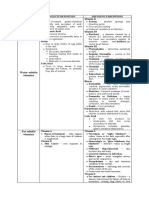
- Water Soluble Vitamins: Vitamins Toxicity/Definition Deficiency/Definition Niacin Vitamin ADocument3 pagesWater Soluble Vitamins: Vitamins Toxicity/Definition Deficiency/Definition Niacin Vitamin ARoshin TejeroNo ratings yet
- WWW - Reliancegeneral.co - In: Important Note: This Is An Electronically Generated Document and Requires No Seal / StampDocument1 pageWWW - Reliancegeneral.co - In: Important Note: This Is An Electronically Generated Document and Requires No Seal / StampdhanishlNo ratings yet
- Radiology Primary Pq.Document34 pagesRadiology Primary Pq.AbosedeNo ratings yet
- Strep A Infection Guidance For Parents and CarersDocument2 pagesStrep A Infection Guidance For Parents and CarersnaziaNo ratings yet
- Article On Prevalence of Substance AbuseDocument32 pagesArticle On Prevalence of Substance AbuseJanice ScatesNo ratings yet
- 10-OBGYN-Glory GroupDocument46 pages10-OBGYN-Glory Groupanmar alkhudhriNo ratings yet
- Occupational Lung DiseasesDocument3 pagesOccupational Lung DiseasesDjdjjd SiisusNo ratings yet
- (05 - 27 - 23) GI DISORDERS - PUD Continuation and GI CancerDocument6 pages(05 - 27 - 23) GI DISORDERS - PUD Continuation and GI CancerMarcus Andrei J RamosNo ratings yet
- Case-Based Textbook of Echocardiography (PDFDrive)Document572 pagesCase-Based Textbook of Echocardiography (PDFDrive)Ringo StoneNo ratings yet
- Psych Nursing Post Test 2 Doc F PDFDocument5 pagesPsych Nursing Post Test 2 Doc F PDFTrisha Mae MarquezNo ratings yet
- Helping Patient With WoundDocument3 pagesHelping Patient With WoundSevina Eka ChannelNo ratings yet
- Module 12Document24 pagesModule 12dasilvashleyNo ratings yet
- Formulation Stabilisation and Encapsulation of Bacteriophage For Phage TherapyDocument34 pagesFormulation Stabilisation and Encapsulation of Bacteriophage For Phage TherapyGerman GodiNo ratings yet
- الوصفة الطبية للعلاج بالتغذية جيمس ف. بالش المكتبة نتDocument705 pagesالوصفة الطبية للعلاج بالتغذية جيمس ف. بالش المكتبة نتDy UwoNo ratings yet
- 1700 Questions Not in PLABABLEDocument131 pages1700 Questions Not in PLABABLEDaniah Marwan Dawood DAWOODNo ratings yet
- FC MS3 (SC)Document8 pagesFC MS3 (SC)madlahuddindayangNo ratings yet
- A Psychobiological Perspective On The Personality Disorders: LarryDocument12 pagesA Psychobiological Perspective On The Personality Disorders: LarryDrobota MirunaNo ratings yet
- Understanding The Six Stages of Disease - Maharishi AyurVedaDocument9 pagesUnderstanding The Six Stages of Disease - Maharishi AyurVedaAlbar MattaNo ratings yet