Download as docx, pdf, or txt
You might also like
- Bigger Than This - Fabian Geyrhalter - 1Document8 pagesBigger Than This - Fabian Geyrhalter - 1abas004No ratings yet
- 12 - 7 - 20 Restoring Mobility Confidence in Amputees Abstract and OutlineDocument5 pages12 - 7 - 20 Restoring Mobility Confidence in Amputees Abstract and OutlineAnca SuciuNo ratings yet
- Case Study IqraDocument7 pagesCase Study IqraIqra ZulfiqarNo ratings yet
- WorddocDocument3 pagesWorddocLakshmi SarvaniNo ratings yet
- Simulation and Design of An Active Orthosis For AnDocument15 pagesSimulation and Design of An Active Orthosis For AnNoor SultanNo ratings yet
- Report Ro 1Document8 pagesReport Ro 1HamzahNo ratings yet
- Novel Soft Bending Actuator-Based Power Augmentation Hand Exoskeleton Controlled by Human IntentionDocument22 pagesNovel Soft Bending Actuator-Based Power Augmentation Hand Exoskeleton Controlled by Human IntentionAlemeNo ratings yet
- Secure Microprocessor-Controlled Prosthetic Leg For Elderly Amputees: Preliminary ResultsDocument15 pagesSecure Microprocessor-Controlled Prosthetic Leg For Elderly Amputees: Preliminary ResultsNada GhammemNo ratings yet
- Effects of Visual and Proprioceptive Motion Feedback On Human Control of Targeted MovementDocument12 pagesEffects of Visual and Proprioceptive Motion Feedback On Human Control of Targeted MovementmacNo ratings yet
- Conexión Directa ANTIGUA (2009) Entre El Cerebro y Protesisdirect - Neural - Sensory - Feedback - and - Control - of - A - Prosthetic - ArmDocument5 pagesConexión Directa ANTIGUA (2009) Entre El Cerebro y Protesisdirect - Neural - Sensory - Feedback - and - Control - of - A - Prosthetic - ArmAERMNo ratings yet
- Closed-Loop Control of Grasping With A Myoelectric Hand Prosthesis: Which Are The Relevant Feedback Variables For Force Control?Document12 pagesClosed-Loop Control of Grasping With A Myoelectric Hand Prosthesis: Which Are The Relevant Feedback Variables For Force Control?alejasoto17No ratings yet
- Mech Biomechatronic HandDocument16 pagesMech Biomechatronic HandDeviprasad MNo ratings yet
- TMP DBE7Document6 pagesTMP DBE7FrontiersNo ratings yet
- Sensors - Editorial Sensor Fusion-2020Document3 pagesSensors - Editorial Sensor Fusion-2020SamuelsonNo ratings yet
- Prosthetic Hand Research PaperDocument5 pagesProsthetic Hand Research Papergpxmlevkg100% (1)
- Prosthesis 05 00084 v2Document26 pagesProsthesis 05 00084 v2A MohanNo ratings yet
- 4545 PDFDocument9 pages4545 PDFRogerDelaCernaNo ratings yet
- Journal of Biomechanics: Josh R. Baxter, Todd J. Hullfish, Wen ChaoDocument5 pagesJournal of Biomechanics: Josh R. Baxter, Todd J. Hullfish, Wen ChaoEma.diazNo ratings yet
- An Osseointegrated Human-Machine Gateway For Long-Term Sensory Feedback and Motor Control of Artificial LimbsDocument9 pagesAn Osseointegrated Human-Machine Gateway For Long-Term Sensory Feedback and Motor Control of Artificial LimbsRogerDelaCernaNo ratings yet
- The Evolution of Prosthetic Devices: A Patent History A Prosthesis (Also Called A Prosthetic Limb, Artificial Limb, or Limb "Replacement"Document4 pagesThe Evolution of Prosthetic Devices: A Patent History A Prosthesis (Also Called A Prosthetic Limb, Artificial Limb, or Limb "Replacement"Эльман МамедовNo ratings yet
- Biomechatronics StudentDocument4 pagesBiomechatronics StudentRebelandarrowNo ratings yet
- Predicting The Performance and Adaptation of Artificial Elbow Due To Effective Forces Using Deep LearningDocument7 pagesPredicting The Performance and Adaptation of Artificial Elbow Due To Effective Forces Using Deep LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Development and Testing of A Human Machine Interface For A Mobile Medical ExoskeletonDocument6 pagesThe Development and Testing of A Human Machine Interface For A Mobile Medical ExoskeletonArsyad Zanadin RamadhanNo ratings yet
- InTech-Lower Limb Wearable ExoskeletonDocument28 pagesInTech-Lower Limb Wearable ExoskeletonJuan Guillermo Patiño VengoecheaNo ratings yet
- An Actuated Finger Exoskeleton For Hand Rehabilitation Following Stroke 2007Document6 pagesAn Actuated Finger Exoskeleton For Hand Rehabilitation Following Stroke 2007newkid2202No ratings yet
- Chapter One 1.0Document32 pagesChapter One 1.0Victor ImehNo ratings yet
- Development of An Upper Limb Exoskeleton For Rehabilitation With Feedback From EMG and IMU SensorDocument7 pagesDevelopment of An Upper Limb Exoskeleton For Rehabilitation With Feedback From EMG and IMU SensorkeerthiNo ratings yet
- @an Exoneuromusculoskeleton For Self-Help Upper LimbDocument22 pages@an Exoneuromusculoskeleton For Self-Help Upper Limbdreams.kuetNo ratings yet
- Lower-Limb Wearable ExoskeletonDocument29 pagesLower-Limb Wearable ExoskeletonMayra MoreiraNo ratings yet
- 10 1016@j JHT 2020 03 024Document10 pages10 1016@j JHT 2020 03 024eduar yecid duarte gomezNo ratings yet
- Chen 2017 A Wearable Exoskeleton Suit For MotDocument12 pagesChen 2017 A Wearable Exoskeleton Suit For MotJUAN RICARDO CASTAÑEDA BELTRANNo ratings yet
- Exo-Glove: A Soft Wearable Robotic Hand For Stroke SurvivorsDocument7 pagesExo-Glove: A Soft Wearable Robotic Hand For Stroke SurvivorsmaheshNo ratings yet
- Design of A Flexible Fluidic Actuation System For A Hybrid ElbowDocument5 pagesDesign of A Flexible Fluidic Actuation System For A Hybrid Elbowdreams.kuetNo ratings yet
- Muri 2013 J. Phys. Conf. Ser. 477 012041Document9 pagesMuri 2013 J. Phys. Conf. Ser. 477 012041JINAL PRAFULKUMAR SHETHNo ratings yet
- Oscillator-Based Assistance of Cyclical Movements: Model-Based and Model-Free ApproachesDocument13 pagesOscillator-Based Assistance of Cyclical Movements: Model-Based and Model-Free Approaches李磊No ratings yet
- Journal of Neuroengineering and RehabilitationDocument16 pagesJournal of Neuroengineering and RehabilitationFikri DzakyNo ratings yet
- 2016 Biorob DesignandEvaluationofAVibrotactileFeedbackSystemtoImproveVolitionalMyoelectricControlforRoboticTranstibialProsthesesDocument7 pages2016 Biorob DesignandEvaluationofAVibrotactileFeedbackSystemtoImproveVolitionalMyoelectricControlforRoboticTranstibialProsthesesTrésor NaraNo ratings yet
- Chapter-1: Neural ProstheticsDocument11 pagesChapter-1: Neural ProstheticsHarshithHarshithNo ratings yet
- BioengineeringDocument17 pagesBioengineeringAdrian ZunigaNo ratings yet
- Sensors of Prosthetic Arm and Its ApplicationsDocument5 pagesSensors of Prosthetic Arm and Its ApplicationsNEHA RAJPUTNo ratings yet
- 2016 - Upper-Limb Stroke Rehabilitation Using Electrode-Array Based Functional Electrical Stimulation With Sensing and Control InnovationsDocument14 pages2016 - Upper-Limb Stroke Rehabilitation Using Electrode-Array Based Functional Electrical Stimulation With Sensing and Control InnovationsAlexandra NistorNo ratings yet
- Exoskeleton ArmDocument5 pagesExoskeleton Armc214ocNo ratings yet
- Unit 1: Rehabilitation EngineeringDocument12 pagesUnit 1: Rehabilitation EngineeringPrasidha PrabhuNo ratings yet
- Movement Biomechanics Goes Upwards-From The Leg To The ArmDocument10 pagesMovement Biomechanics Goes Upwards-From The Leg To The ArmMuhammad FahmyNo ratings yet
- Isolated Calcaneocuboid Instability - A Unique DiagDocument18 pagesIsolated Calcaneocuboid Instability - A Unique Diagvijaypatel4282No ratings yet
- Rehabilitation: Rajalakshmi Engineering CollegeDocument7 pagesRehabilitation: Rajalakshmi Engineering Collegenanthini priyaNo ratings yet
- Automation of Upper Limb Prostheses Using Shape Memory AlloysDocument8 pagesAutomation of Upper Limb Prostheses Using Shape Memory AlloysÁSädKHänNo ratings yet
- Presented By, K.Kavin Kumar (I-BE-MECH) S.Sangeeth (I-BE-MECH)Document15 pagesPresented By, K.Kavin Kumar (I-BE-MECH) S.Sangeeth (I-BE-MECH)Kavin RKNo ratings yet
- Neuro MEMsDocument15 pagesNeuro MEMsDevika KishnanNo ratings yet
- Motion Analysis and Postural Stability of Transtibial Prosthesis UsersDocument6 pagesMotion Analysis and Postural Stability of Transtibial Prosthesis UsersMady BuzeaNo ratings yet
- International Journal of Physical Medicine & RehabilitationDocument4 pagesInternational Journal of Physical Medicine & RehabilitationDebbieNo ratings yet
- Design of A Patient-Tailored Active Knee-Ankle-Foot Orthosis To Assist The Gait of Spinal Cord Injured SubjectsDocument2 pagesDesign of A Patient-Tailored Active Knee-Ankle-Foot Orthosis To Assist The Gait of Spinal Cord Injured SubjectsAlexandru NituNo ratings yet
- Self-Contained Neuromusculoskeletal Arm Prostheses: Brief ReportDocument7 pagesSelf-Contained Neuromusculoskeletal Arm Prostheses: Brief ReportGaspar ContrerasNo ratings yet
- An Emg-Controlled Hand Exoskeleton For Natural Pinching: Lenny Lucas, Matthew Dicicco, and Yoky MatsuokaDocument7 pagesAn Emg-Controlled Hand Exoskeleton For Natural Pinching: Lenny Lucas, Matthew Dicicco, and Yoky MatsuokasachinNo ratings yet
- Design and Simulation of Bionic Glove For Rehabilitation of The ParalyticsDocument7 pagesDesign and Simulation of Bionic Glove For Rehabilitation of The ParalyticsAdi CrişanNo ratings yet
- AD - 3. Short Q & ADocument4 pagesAD - 3. Short Q & AVasanth VasanthNo ratings yet
- Design and Modeling of An Upper Extremity ExoskeletonDocument5 pagesDesign and Modeling of An Upper Extremity Exoskeletondreams.kuetNo ratings yet
- Bionic Limb ReconstructionFrom EverandBionic Limb ReconstructionOskar C. AszmannNo ratings yet
- Design of A Flexible Fluidic Actuation System For A Hybrid Elbow OrthosisDocument5 pagesDesign of A Flexible Fluidic Actuation System For A Hybrid Elbow OrthosisRTC NISERNo ratings yet
- Walking Simulation Model of Lower Limb Exoskeleton Robot DesignDocument11 pagesWalking Simulation Model of Lower Limb Exoskeleton Robot Designandersson benito herrera100% (1)
- Biomechanics Actuation and Multi-Level Control str1Document29 pagesBiomechanics Actuation and Multi-Level Control str1daniyal chNo ratings yet
- Zero Variance-Problem StatementDocument4 pagesZero Variance-Problem StatementR N Guru50% (2)
- DN Diametre Nominal-NPS Size ChartDocument5 pagesDN Diametre Nominal-NPS Size ChartSankar CdmNo ratings yet
- Tractive EffortDocument5 pagesTractive EffortVarshith RapellyNo ratings yet
- Instant Coffee With Natural Aroma by Spray-Drying.: January 1993Document8 pagesInstant Coffee With Natural Aroma by Spray-Drying.: January 1993Nhan NguyenNo ratings yet
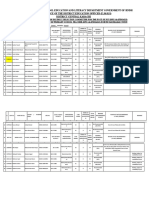
- School Education and Literacy Department Government of Sindh Office of The District Education Officer (E, S&H.S) District Central KarachiDocument15 pagesSchool Education and Literacy Department Government of Sindh Office of The District Education Officer (E, S&H.S) District Central KarachiNaya PakistanNo ratings yet
- PD Lesson 5 Coping With Stress in Middle and Late AdolescenceDocument16 pagesPD Lesson 5 Coping With Stress in Middle and Late AdolescenceEL FuentesNo ratings yet
- Content Extraction From Marketing Flyers: (Ignazio - Gallo, A.zamberletti, Lucia - Noce) @uninsubria - ItDocument2 pagesContent Extraction From Marketing Flyers: (Ignazio - Gallo, A.zamberletti, Lucia - Noce) @uninsubria - ItcYbernaTIc enHancENo ratings yet
- Pakistan Petroleum Limited ProjectDocument6 pagesPakistan Petroleum Limited ProjectRandum PirsonNo ratings yet
- CH 2 - Electrostatic Potential - MCQDocument2 pagesCH 2 - Electrostatic Potential - MCQDeepali MalhotraNo ratings yet
- Developmental Language Disorder Is Psycholinguistic Injustice: Tagalog Knowledge From A Philippine ContextDocument38 pagesDevelopmental Language Disorder Is Psycholinguistic Injustice: Tagalog Knowledge From A Philippine ContextMarie Adrienne RoblesNo ratings yet
- Xi TGB 1 Kelompok 5Document29 pagesXi TGB 1 Kelompok 5windaNo ratings yet
- Modern Methods of Diaphragm Walls Design: SustainabilityDocument13 pagesModern Methods of Diaphragm Walls Design: SustainabilitymattNo ratings yet
- Jurnal Mina Sains ISSN: 2407-9030 Volume 2 Nomor 2, Oktober 2016 71Document9 pagesJurnal Mina Sains ISSN: 2407-9030 Volume 2 Nomor 2, Oktober 2016 71yudhoNo ratings yet
- Computer Graphics - Course OutlineDocument3 pagesComputer Graphics - Course OutlineasamenekNo ratings yet
- Import ManagementDocument26 pagesImport ManagementPavle ArsicNo ratings yet
- Operations Research Summer 2019Document2 pagesOperations Research Summer 2019Diksha PatilNo ratings yet
- Architectural Research MethodsDocument4 pagesArchitectural Research MethodsMemoona SheesNo ratings yet
- FINAL Shivani Confined Space PermitDocument1 pageFINAL Shivani Confined Space PermitVimal SinghNo ratings yet
- Electrical Power Supply and DistributionDocument122 pagesElectrical Power Supply and Distributionmmalamuti9325100% (4)
- GEM2xxxManualEN RevD1Document73 pagesGEM2xxxManualEN RevD1Aldo Germán Pavez MoraNo ratings yet
- Footing Cutting List: Mark Length Width Thickness Spacing Bar Diameter Top&Botom Clear CoverDocument3 pagesFooting Cutting List: Mark Length Width Thickness Spacing Bar Diameter Top&Botom Clear CoverJohn Rhey Almojallas BenedictoNo ratings yet
- Samsung Ua40c6200uf Ua46c6200uf Ua55c6200uf Ua32c6900vf Ua40c6900vf Ua46c6900vf Ua55c6900vf Chassis N96a Led PDFDocument121 pagesSamsung Ua40c6200uf Ua46c6200uf Ua55c6200uf Ua32c6900vf Ua40c6900vf Ua46c6900vf Ua55c6900vf Chassis N96a Led PDFNina SeimeniNo ratings yet
- Kirchhoff S LawsDocument35 pagesKirchhoff S LawsCzarina Jane PeregrinNo ratings yet
- 2018 - 2019 Environmental Engineering EnvirEng Syllabus IEDocument5 pages2018 - 2019 Environmental Engineering EnvirEng Syllabus IEImogen YstNo ratings yet
- Triangles - Class 10 - Notes - PANTOMATHDocument8 pagesTriangles - Class 10 - Notes - PANTOMATHsourav9823100% (1)
- IC5 Level Intro - Scope - and - SequenceDocument4 pagesIC5 Level Intro - Scope - and - Sequencematerial didacticoNo ratings yet
- PointLink - Release Notes - R2.4.0.0 Rev.ADocument27 pagesPointLink - Release Notes - R2.4.0.0 Rev.AManuel MolinaNo ratings yet
- LIMITSMains PDFDocument18 pagesLIMITSMains PDFBhavadip VamjaNo ratings yet
- Soal (1) (Repaired)Document9 pagesSoal (1) (Repaired)Inda AlwanNo ratings yet