Download as pdf or txt
You might also like
- Module - Partially - Edited22 PDFDocument174 pagesModule - Partially - Edited22 PDFashe zinab80% (5)
- Fetal SkullDocument17 pagesFetal SkullCham_Aley100% (1)
- Professional Diploma in Sports Nutrition: Lesson 4Document31 pagesProfessional Diploma in Sports Nutrition: Lesson 4Jomari ServanoNo ratings yet
- 3D-Printed Masks As A New Approach For ImmobilizatDocument9 pages3D-Printed Masks As A New Approach For ImmobilizatRinku BalwadaNo ratings yet
- Ultrasound Imaging ThesisDocument7 pagesUltrasound Imaging Thesisbrendazerrindependence100% (2)
- Ijerph 18 13131Document10 pagesIjerph 18 13131Mohamed EL OULKINo ratings yet
- RT CR ESPINAL RapidArc 2011Document7 pagesRT CR ESPINAL RapidArc 2011Raul Matute MartinNo ratings yet
- PIIS0009926020302324Document4 pagesPIIS0009926020302324Jhonny RomeroNo ratings yet
- Igrt ThesisDocument8 pagesIgrt Thesislisanetkowiczerie100% (1)
- Vestibular Schwannoma Results of HypofractionatedDocument14 pagesVestibular Schwannoma Results of HypofractionatedTimothy CaldwellNo ratings yet
- SRS Linac Based Clinical ImplementationDocument9 pagesSRS Linac Based Clinical ImplementationPablo Castro PenaNo ratings yet
- 508 - 7 CardiologyDocument9 pages508 - 7 CardiologymlinaballerinaNo ratings yet
- Radiodiagnosis Thesis TopicsDocument8 pagesRadiodiagnosis Thesis Topicsjmvnqiikd100% (2)
- A Domestic Porcine Model For Studying The Effects of Radiation On Head and Neck CancersDocument8 pagesA Domestic Porcine Model For Studying The Effects of Radiation On Head and Neck CancersdaruNo ratings yet
- Scatter and Staff Dose Level in Paediatric Intervencionism PDFDocument8 pagesScatter and Staff Dose Level in Paediatric Intervencionism PDFsebastian CarrascoNo ratings yet
- Thesis RadiotherapyDocument6 pagesThesis Radiotherapylakeishajonesjackson100% (2)
- Research Proposal FinalDocument4 pagesResearch Proposal Finalapi-480222490No ratings yet
- Deep Learning and Artificial Intelligence in Radiology: Current Applications and Future DirectionsDocument4 pagesDeep Learning and Artificial Intelligence in Radiology: Current Applications and Future DirectionsFadhilWNo ratings yet
- Roder 2014Document8 pagesRoder 2014Carlos VidalNo ratings yet
- Somatom Sessions 31 Final Rsna Not Us-00556396Document60 pagesSomatom Sessions 31 Final Rsna Not Us-005563962vjNo ratings yet
- Intracranial Stereotactic Radiotherapy With A JawlDocument8 pagesIntracranial Stereotactic Radiotherapy With A JawlG WNo ratings yet
- Brain Tumor ThesisDocument5 pagesBrain Tumor Thesisdwpeprje100% (2)
- Research Paper On Radiation TherapyDocument8 pagesResearch Paper On Radiation Therapyfveec9sx100% (1)
- 4digital Chest Radiography An Update On Modern Technology, Dose Containment and Control of Image QualityDocument13 pages4digital Chest Radiography An Update On Modern Technology, Dose Containment and Control of Image QualityKarl SturausNo ratings yet
- Multi-Center MRI Carotid Plaque Component Segmentation Using Feature Normalization and Transfer LearningDocument12 pagesMulti-Center MRI Carotid Plaque Component Segmentation Using Feature Normalization and Transfer LearningganeshNo ratings yet
- Comparison of Coplanar and Non - Coplanarvmat For Brain Cancer by Using The Dosimetrical and Radiobiological IndicesDocument20 pagesComparison of Coplanar and Non - Coplanarvmat For Brain Cancer by Using The Dosimetrical and Radiobiological IndicesIJAR JOURNALNo ratings yet
- Intraoperative Radiotherapy During Awake Craniotomies - Preliminary Results of A Single-Center Case SeriesDocument7 pagesIntraoperative Radiotherapy During Awake Craniotomies - Preliminary Results of A Single-Center Case Seriesuyenminh2802No ratings yet
- FiltrationDocument16 pagesFiltrationjojokawayNo ratings yet
- Automatic Treatment Planning For VMAT-based TotalDocument12 pagesAutomatic Treatment Planning For VMAT-based TotalAmra IbrahimovicNo ratings yet
- LawsonDocument7 pagesLawsonrodolfo gorveñaNo ratings yet
- Intraop Feedback and Quality ControlDocument12 pagesIntraop Feedback and Quality Controllaljadeff12No ratings yet
- TAC en TraumaDocument9 pagesTAC en Traumasamuelfdiaz.0103No ratings yet
- Automated Segmentation of Head CT Scans for Computerassisted Craniomaxillofacial Surgery Applying a Hierarchical Patchbased Stack of Convolutional Neural NetworksInternational Journal of Computer Assisted RadiologyDocument9 pagesAutomated Segmentation of Head CT Scans for Computerassisted Craniomaxillofacial Surgery Applying a Hierarchical Patchbased Stack of Convolutional Neural NetworksInternational Journal of Computer Assisted Radiologyhajar.outaybiNo ratings yet
- TERTIARY X-RADIATIONâ A PROBLEM FOR STAFF PROTECTION - (Radiation Protection Dosimetry) (2020)Document8 pagesTERTIARY X-RADIATIONâ A PROBLEM FOR STAFF PROTECTION - (Radiation Protection Dosimetry) (2020)Piotr JankowskiNo ratings yet
- A Paediatric X-Ray Exposure ChartDocument11 pagesA Paediatric X-Ray Exposure Chartdddemourita9249No ratings yet
- A Paediatric X-Ray Exposure ChartDocument11 pagesA Paediatric X-Ray Exposure ChartMarco Jimenez HerreraNo ratings yet
- Klatt 2013Document4 pagesKlatt 2013Sung Soon ChangNo ratings yet
- State-Of-The-Art On Cone Beam CT Imaging For Preoperative Planning of Implant PlacementDocument7 pagesState-Of-The-Art On Cone Beam CT Imaging For Preoperative Planning of Implant Placementanimeilove3No ratings yet
- Scheimpflug Corneal Densitometry Changes After TrabeculectomyDocument7 pagesScheimpflug Corneal Densitometry Changes After TrabeculectomyFernando MartínezNo ratings yet
- 17.PLDD Vs Surgery RCTDocument9 pages17.PLDD Vs Surgery RCTBeata SviantickaNo ratings yet
- Lee2017 PDFDocument12 pagesLee2017 PDFian3yeung-2No ratings yet
- Landry Imasim FrontiersBiomedPhys 13Document8 pagesLandry Imasim FrontiersBiomedPhys 13ChiLdish GEe HAhNo ratings yet
- PLDD&MicrodiscectomyLeiden NL 2015Document9 pagesPLDD&MicrodiscectomyLeiden NL 2015YAŞAR TÜRKNo ratings yet
- Cone Beam RadiazioniDocument4 pagesCone Beam RadiazioniWaheed MidoNo ratings yet
- 19MCB0010 Paper - 130321Document6 pages19MCB0010 Paper - 130321Godwin EmmanuelNo ratings yet
- Clinical Application CTDocument40 pagesClinical Application CTWalaa MajeedNo ratings yet
- Intelligence-Based MedicineDocument15 pagesIntelligence-Based MedicineGustavo ColimbaNo ratings yet
- 1 s2.0 S2468294221000605 MainDocument7 pages1 s2.0 S2468294221000605 MainVishal BasuNo ratings yet
- Tongue Tumor Detection in Hyperspectral Images Using Deep Learning Semantic SegmentationDocument11 pagesTongue Tumor Detection in Hyperspectral Images Using Deep Learning Semantic Segmentationanchal18052001No ratings yet
- Margret Jensdottir Learning Curve Analysis and AdverseDocument9 pagesMargret Jensdottir Learning Curve Analysis and AdverseJesus PerezNo ratings yet
- Medical Image AnalysisDocument18 pagesMedical Image AnalysisJawwad SamiNo ratings yet
- Radiation Doses of Indirect and Direct Digital Cephalometric RadiographyDocument4 pagesRadiation Doses of Indirect and Direct Digital Cephalometric RadiographyMarilyn GonzalesNo ratings yet
- J Ejmp 2020 02 017Document2 pagesJ Ejmp 2020 02 017Camilo SotomayorNo ratings yet
- 10.1186@1748 717X 1 17.pdfMUNTER PDFDocument6 pages10.1186@1748 717X 1 17.pdfMUNTER PDFpaolaNo ratings yet
- Plowman 1999Document3 pagesPlowman 1999Sarly FebrianaNo ratings yet
- Deep Convolutional Neural Networks For Lung Nodule Detection: Improvement in Small Nodule IdentificationDocument9 pagesDeep Convolutional Neural Networks For Lung Nodule Detection: Improvement in Small Nodule Identificationdreadrebirth2342No ratings yet
- Shielding Requirements in Helical Tomotherapy: Home Search Collections Journals About Contact Us My IopscienceDocument12 pagesShielding Requirements in Helical Tomotherapy: Home Search Collections Journals About Contact Us My IopscienceSayan DasNo ratings yet
- Research Article: Automated Quantification of Pneumothorax in CTDocument8 pagesResearch Article: Automated Quantification of Pneumothorax in CTAnnisa HidayatiNo ratings yet
- 1-IsRS Technical Guidelines For StereotacticDocument12 pages1-IsRS Technical Guidelines For Stereotactictaharount.amel20No ratings yet
- Automated Brain Tumor Detection of MRI Image Based On Hybrid Image Processing TechniquesDocument10 pagesAutomated Brain Tumor Detection of MRI Image Based On Hybrid Image Processing TechniquesTELKOMNIKANo ratings yet
- Comparison of Different Number of Beams in Intensity Modulated Radiotherapy in Head and Neck CancerDocument11 pagesComparison of Different Number of Beams in Intensity Modulated Radiotherapy in Head and Neck CancerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Brain Tumor Classification Using Hybrid Single Image Super-Resolution Technique With ResNext101!32!8d and VGG19 PRDocument14 pagesBrain Tumor Classification Using Hybrid Single Image Super-Resolution Technique With ResNext101!32!8d and VGG19 PRthanugaduputiNo ratings yet
- Sudan STEPwise SURVEY Final 2016Document148 pagesSudan STEPwise SURVEY Final 2016Abubakar BusatiNo ratings yet
- Jespersen Et Al-2022-Cochrane Database of Systematic ReviewsDocument78 pagesJespersen Et Al-2022-Cochrane Database of Systematic ReviewsQuan VuNo ratings yet
- Principles of Healthcare Reimbursement: Sixth EditionDocument20 pagesPrinciples of Healthcare Reimbursement: Sixth EditionDestiny HayesNo ratings yet
- Focusing - Jund and GendlingDocument10 pagesFocusing - Jund and GendlingAriel Pollak100% (1)
- Case Note 9Document2 pagesCase Note 9BINCYNo ratings yet
- Civ 2 DigestDocument20 pagesCiv 2 DigestGabrielAblolaNo ratings yet
- How To Write A Plant Operating ManualDocument11 pagesHow To Write A Plant Operating ManualZia AbbasiNo ratings yet
- Sugar - The White DeathDocument4 pagesSugar - The White DeathSyncOrSwimNo ratings yet
- HLTWHS001 Assessment 3 Risk Assessment (Fixed) by Rachael-Lyn AndersonDocument2 pagesHLTWHS001 Assessment 3 Risk Assessment (Fixed) by Rachael-Lyn AndersonAndrea AndersonNo ratings yet
- Data Peserta Event Seminar & Workshop Pit Idi SumedangDocument3 pagesData Peserta Event Seminar & Workshop Pit Idi SumedangDerri HafaNo ratings yet
- List of Participand in The UnicepDocument9 pagesList of Participand in The UnicepdangthanhnghiNo ratings yet
- Use of Ethno-Veterinary Medicine For Therapy of Reprod DisordersDocument11 pagesUse of Ethno-Veterinary Medicine For Therapy of Reprod DisordersgnpobsNo ratings yet
- BIQ Manual-4Document8 pagesBIQ Manual-4Pavithra ChinnaiyanNo ratings yet
- Sex Selection: Any Taker?Document10 pagesSex Selection: Any Taker?Czar SJ100% (1)
- PsychologyDocument2 pagesPsychologymdw_wellsNo ratings yet
- MSRA For Cable Tray InstallationDocument8 pagesMSRA For Cable Tray InstallationRAMY ABOU AL DAHABNo ratings yet
- The Impact of Gingivitis On The Quality of Life in Pregnant WomanDocument13 pagesThe Impact of Gingivitis On The Quality of Life in Pregnant WomanYasinta JusufNo ratings yet
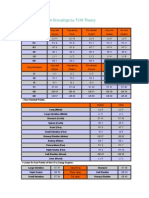
- Acupuncture Point Groupings by TCM TheoryDocument5 pagesAcupuncture Point Groupings by TCM TheoryDhandayuthapaniJawaharlal100% (2)
- 100 Years of Excellance For Saint Louis University School of Medicine Department of Internal MedicineDocument4 pages100 Years of Excellance For Saint Louis University School of Medicine Department of Internal MedicineSlusom WebNo ratings yet
- Emotional Stability Among College YouthDocument4 pagesEmotional Stability Among College YouthAllen Lois LanuzaNo ratings yet
- Parasitology in The Atharva Veda - Rulia Ram KashyapDocument22 pagesParasitology in The Atharva Veda - Rulia Ram KashyapArun KanthNo ratings yet
- SPC Septobar Effervescent GranulesDocument3 pagesSPC Septobar Effervescent GranulesAia Hassan100% (1)
- OrientationDocument11 pagesOrientationCarissa De Luzuriaga-Balaria0% (1)
- Stock 15 FebDocument15 pagesStock 15 FebnaelarizqiNo ratings yet
- Applied Ergonomics: D.C. Tappin, A. Vitalis, T.A. BentleyDocument9 pagesApplied Ergonomics: D.C. Tappin, A. Vitalis, T.A. Bentleykhuram gillNo ratings yet
- Dairy Processing PlantsDocument9 pagesDairy Processing PlantsRohit SinghNo ratings yet
- CASE Presentation Psychia Holy Child College of DavaoDocument45 pagesCASE Presentation Psychia Holy Child College of DavaoMonemah Essa Francisco Martinez100% (2)