
ESMO 2023 Management of Breast Cancer During Pregnancy 3
ESMO 2023 Management of Breast Cancer During Pregnancy 3
You might also like
- Libro R. Khandpur-Biomedical Instrumentation - Technology and Applications-McGraw-Hill Professional (2004)Document943 pagesLibro R. Khandpur-Biomedical Instrumentation - Technology and Applications-McGraw-Hill Professional (2004)Dulcina Tucuman100% (18)
- Medical Network English JORDAN 1Document342 pagesMedical Network English JORDAN 1Sandhya KhannaNo ratings yet
- Breast Cancer ScreeningDocument21 pagesBreast Cancer ScreeningBolivar Isea100% (1)
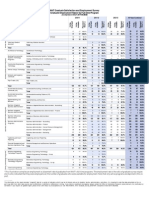
- NAIT - Graduate Employment Rates by Full-Time Program PDFDocument5 pagesNAIT - Graduate Employment Rates by Full-Time Program PDFpauloednNo ratings yet
- Manejo Cancer de Mama y EmbarazoDocument10 pagesManejo Cancer de Mama y EmbarazoLaura LealNo ratings yet
- Advances in Screening, Diagnosis, and Treatment ofDocument7 pagesAdvances in Screening, Diagnosis, and Treatment ofBastomy EkaNo ratings yet
- Jmri 26654Document14 pagesJmri 26654marizal saputraNo ratings yet
- Untitled PDFDocument9 pagesUntitled PDFFaruq AbdanNo ratings yet
- Cervical Conization and The Risk of Preterm DeliveryDocument11 pagesCervical Conization and The Risk of Preterm DeliveryGelo ConcepcionNo ratings yet
- Roe 2018Document11 pagesRoe 2018mohamaed abbasNo ratings yet
- J of Obstet and Gynaecol - 2023 - - Update Management of Cervical Precancer LesionDocument12 pagesJ of Obstet and Gynaecol - 2023 - - Update Management of Cervical Precancer Lesionzakiah11No ratings yet
- Colposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Document155 pagesColposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Annca RoXanna100% (1)
- Cervical Cancer - A Global Health CrisisDocument9 pagesCervical Cancer - A Global Health Crisispb.nakulaNo ratings yet
- 242 FullDocument5 pages242 FullsarahNo ratings yet
- Captura de Pantalla 2021-10-08 A La(s) 7.52.39 A. M.Document10 pagesCaptura de Pantalla 2021-10-08 A La(s) 7.52.39 A. M.LINA MARIA CAMELO COLORADONo ratings yet
- Cervical CADocument10 pagesCervical CAAby ShauNo ratings yet
- Correlation of PAP Smear Findings With Clinical Findings and Cervical BiopsyDocument7 pagesCorrelation of PAP Smear Findings With Clinical Findings and Cervical BiopsyKavita Saxena KhareNo ratings yet
- Journal of The National Cancer Center: A R T I C L e I N F o A B S T R A C TDocument8 pagesJournal of The National Cancer Center: A R T I C L e I N F o A B S T R A C TCirugia SolcaNo ratings yet
- Density and Tailored Breast Cancer Screening: Practice and Prediction - An OverviewDocument12 pagesDensity and Tailored Breast Cancer Screening: Practice and Prediction - An Overviewelisabeth harahapNo ratings yet
- Jco 18 00378Document11 pagesJco 18 00378Valéria CruzNo ratings yet
- Greenwood 2019Document13 pagesGreenwood 2019Ottofianus Hewick KalangiNo ratings yet
- Ijcmr 1184 Dec 28Document3 pagesIjcmr 1184 Dec 28BayuHernawanRahmatMuhariaNo ratings yet
- Tiwari 2017Document3 pagesTiwari 2017Dewa OkaNo ratings yet
- Cervicalcancerprevention: Immunization and Screening 2015Document9 pagesCervicalcancerprevention: Immunization and Screening 2015behanges71No ratings yet
- Diagnosis and Treatment of Cervical Cancer in Pregnant WomenDocument6 pagesDiagnosis and Treatment of Cervical Cancer in Pregnant WomenSofi PiñaNo ratings yet
- The Diagnostic Value of Ultrasound and Mammography in Detection of Breast Cancer in AlbaniaDocument10 pagesThe Diagnostic Value of Ultrasound and Mammography in Detection of Breast Cancer in AlbaniaIJPHSNo ratings yet
- Breast Fine Needle Aspiration Cytology Reporting Icet13i2p54Document6 pagesBreast Fine Needle Aspiration Cytology Reporting Icet13i2p54salijanstarNo ratings yet
- PIIS2213398422000902Document7 pagesPIIS2213398422000902Manas BhatiaNo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 5Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 5EDWIN WIJAYANo ratings yet
- Figo 2018Document15 pagesFigo 2018EJ CMNo ratings yet
- Seminars in Oncology NursingDocument9 pagesSeminars in Oncology NursingangelitostorresitosNo ratings yet
- Effect of Cervicitis On Visual Inspection With Acetic AcidDocument5 pagesEffect of Cervicitis On Visual Inspection With Acetic AcidmonicamoniccNo ratings yet
- Editorial: Molecular Imaging in Breast CancerDocument4 pagesEditorial: Molecular Imaging in Breast CancerKurnia AlkatiriNo ratings yet
- CBEDocument17 pagesCBElovtetaNo ratings yet
- Background Parenchymal Enhancement in Breast MriDocument19 pagesBackground Parenchymal Enhancement in Breast Mridr.elahe.babantaherNo ratings yet
- Cervical Cancer: Prevention, Diagnosis, and TherapeuticsDocument23 pagesCervical Cancer: Prevention, Diagnosis, and TherapeuticsranggadrNo ratings yet
- Poster Session II: ObjectiveDocument1 pagePoster Session II: ObjectivefujimeisterNo ratings yet
- FIGO 2018 - Cervical CADocument15 pagesFIGO 2018 - Cervical CAJP RecioNo ratings yet
- PIIS0002937821019992Document2 pagesPIIS0002937821019992made dharmaNo ratings yet
- Society For Maternal-Fetal Medicine (SMFM) Consult Series #49: Cesarean Scar PregnancyDocument13 pagesSociety For Maternal-Fetal Medicine (SMFM) Consult Series #49: Cesarean Scar PregnancyTandyo TriasmoroNo ratings yet
- Hippokratia 11 063Document4 pagesHippokratia 11 063Wiedya kristiantiNo ratings yet
- 33 - 6507 - e (C) - F (T) - PF1 (VP - SH) - Pfa (H) - Pfa (P)Document3 pages33 - 6507 - e (C) - F (T) - PF1 (VP - SH) - Pfa (H) - Pfa (P)Satish SinghNo ratings yet
- KarsinomaDocument12 pagesKarsinomaWahyudi Pratama HarliNo ratings yet
- Summary of Data: Cervical Cancer and ScreeningDocument10 pagesSummary of Data: Cervical Cancer and Screeningpalomazul007No ratings yet
- Screen-and-Treat Approaches For Cervical Cancer Prevention in Low-Resource SettingsDocument9 pagesScreen-and-Treat Approaches For Cervical Cancer Prevention in Low-Resource SettingsSaddam FuadNo ratings yet
- Cost Effective, Portable, Patient Dedicated Three Dimensional Automated Breast Ultrasound For Point of Care Breast Cancer ScreeningDocument16 pagesCost Effective, Portable, Patient Dedicated Three Dimensional Automated Breast Ultrasound For Point of Care Breast Cancer ScreeningCabbagePotatoNo ratings yet
- Comparison of Ultrasound and Mammography For Early DiagnosisDocument8 pagesComparison of Ultrasound and Mammography For Early Diagnosishdh1224No ratings yet
- Malignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalDocument8 pagesMalignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalorriNo ratings yet
- Screeningforcervical Cancer: Terresa J. Eun,, Rebecca B. PerkinsDocument16 pagesScreeningforcervical Cancer: Terresa J. Eun,, Rebecca B. PerkinsLis RibeiroNo ratings yet
- Cervical Cancer Research 1Document9 pagesCervical Cancer Research 1tivaNo ratings yet
- Cervical Cancer - An Overview of Pathophysiology and ManagementDocument9 pagesCervical Cancer - An Overview of Pathophysiology and ManagementIndah 15No ratings yet
- Will HPV Vaccination Prevent Cervical Cancer?: Claire P Rees, Petra Brhlikova and Allyson M PollockDocument15 pagesWill HPV Vaccination Prevent Cervical Cancer?: Claire P Rees, Petra Brhlikova and Allyson M PollockGina Ionescu AnculeteNo ratings yet
- Professional Med J Q 2012 19 5 620 624Document5 pagesProfessional Med J Q 2012 19 5 620 624monica_elysabethNo ratings yet
- Accuracy of Triple Test Score in The Diagnosis of Palpable Breast LumpDocument4 pagesAccuracy of Triple Test Score in The Diagnosis of Palpable Breast LumpBmu CarreonNo ratings yet
- Ca Cervix y Emb 2Document14 pagesCa Cervix y Emb 2Nathalia M.No ratings yet
- Iva Screening2Document9 pagesIva Screening2ponekNo ratings yet
- Peprah 2018Document7 pagesPeprah 2018Dewa OkaNo ratings yet
- Meijers Heijboer2001Document6 pagesMeijers Heijboer2001Market PlusNo ratings yet
- The Management and Prevention of Anal Squamous Cell CarcinomaDocument10 pagesThe Management and Prevention of Anal Squamous Cell CarcinomaGabriela LemNo ratings yet
- Neoplasia Vaginal, Abril 2022Document6 pagesNeoplasia Vaginal, Abril 2022rafael martinezNo ratings yet
- EMBASE Cowden BreastDocument17 pagesEMBASE Cowden BreastCiudadano “Citizen Dick” VolanteNo ratings yet
- Medip, IJRCOG-5630 O PDFDocument5 pagesMedip, IJRCOG-5630 O PDFSuraj NagarajNo ratings yet
- Atypical Breast Proliferative Lesions and Benign Breast DiseaseFrom EverandAtypical Breast Proliferative Lesions and Benign Breast DiseaseFarin AmersiNo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 17Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 17EDWIN WIJAYANo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 16Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 16EDWIN WIJAYANo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 18Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 18EDWIN WIJAYANo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 7Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 7EDWIN WIJAYANo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 2Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 2EDWIN WIJAYANo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 6Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 6EDWIN WIJAYANo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 14Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 14EDWIN WIJAYANo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 18Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 18EDWIN WIJAYANo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 1Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 1EDWIN WIJAYANo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 2Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 2EDWIN WIJAYANo ratings yet
- Vitamin D and Bone Health 6Document1 pageVitamin D and Bone Health 6EDWIN WIJAYANo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 3Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 3EDWIN WIJAYANo ratings yet
- Vitamin D and Bone Health 5Document1 pageVitamin D and Bone Health 5EDWIN WIJAYANo ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument24 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusEDWIN WIJAYANo ratings yet
- Vitamin D and Bone Health 4Document1 pageVitamin D and Bone Health 4EDWIN WIJAYANo ratings yet
- Insulin Therapy in Type 2 Diabetes MellitusDocument40 pagesInsulin Therapy in Type 2 Diabetes MellitusEDWIN WIJAYANo ratings yet
- Apollo HospitalDocument106 pagesApollo HospitalNoor Ibne SalehinNo ratings yet
- Surface Guided Radiation TherapyDocument515 pagesSurface Guided Radiation TherapyEduardo RodriguezNo ratings yet
- Notes Extention ListDocument16 pagesNotes Extention ListShivani YadavNo ratings yet
- Ultrasound GuidedDocument6 pagesUltrasound GuidedsaminNo ratings yet
- Principles of Radiation OncologyDocument21 pagesPrinciples of Radiation Oncologydinu_maria95No ratings yet
- Brochure ACUSON ASPENDocument2 pagesBrochure ACUSON ASPENWolaé Mathurin Edmond AmegandjinNo ratings yet
- University Institute of Radiological Medical Imaging TechnologyDocument1 pageUniversity Institute of Radiological Medical Imaging TechnologyV KookNo ratings yet
- Fo23rm Report FULL 2019Document4 pagesFo23rm Report FULL 2019amir_heroNo ratings yet
- A BERT Encoding With Recurrent Neural Network and Long-Short Term Memory For Breast Cancer Image Classification - 1-s2.0-S2772662223000176-MainDocument15 pagesA BERT Encoding With Recurrent Neural Network and Long-Short Term Memory For Breast Cancer Image Classification - 1-s2.0-S2772662223000176-MainSrinitish SrinivasanNo ratings yet
- Philips Healthcare (Suzhou) Co., LTDDocument4 pagesPhilips Healthcare (Suzhou) Co., LTDAli R.MNo ratings yet
- Lower ExtremityDocument1 pageLower ExtremityAmir mushtaqNo ratings yet
- Spinal Tuberculosis A Comprehensive Review For The Modern SpineDocument13 pagesSpinal Tuberculosis A Comprehensive Review For The Modern SpineRaunik BansodNo ratings yet
- 2012 DI Accessories CatalogDocument256 pages2012 DI Accessories CatalogchavanikhilNo ratings yet
- Cerebral Palsy: An Overview: The Centers For Disease ControlDocument8 pagesCerebral Palsy: An Overview: The Centers For Disease ControlAlma PradiftaNo ratings yet
- Professor List For International Students (2021)Document4 pagesProfessor List For International Students (2021)Abrar HamimNo ratings yet
- Physics ProjectDocument17 pagesPhysics ProjectLance ShahNo ratings yet
- ID Perhitungan Nilai Dosis Dan Kontras CitrDocument9 pagesID Perhitungan Nilai Dosis Dan Kontras CitrNur cholisNo ratings yet
- Aquilion PRIMEDocument22 pagesAquilion PRIMEvitapabloNo ratings yet
- Rajiv Gandhi University of Health Sciences, KarnatakaDocument16 pagesRajiv Gandhi University of Health Sciences, KarnatakaSanthana PriyaNo ratings yet
- Radiographic Image Analysis 4Document562 pagesRadiographic Image Analysis 4Jessica Ugalde Mata100% (2)
- Value of Chest Ultrasound in Diagnosis of Community Acquired PneumoniaDocument5 pagesValue of Chest Ultrasound in Diagnosis of Community Acquired PneumoniaHarlan SiMarmutNo ratings yet
- Ebook A Selection of Image Processing Techniques From Fundamental To Research Front 1St Edition Yu Jin Zhang Online PDF All ChapterDocument70 pagesEbook A Selection of Image Processing Techniques From Fundamental To Research Front 1St Edition Yu Jin Zhang Online PDF All Chapterwalter.dyer746100% (12)
- List of Hospitals and Diagnostic Centers Empanelled With CGHS, Delhi W.e.f.01.11Document8 pagesList of Hospitals and Diagnostic Centers Empanelled With CGHS, Delhi W.e.f.01.11sudhanshupandey9No ratings yet
- Lumbar Disc Herniation: Evidence-Based Guidelines-A Review: The Indian Practitioner March 2016Document7 pagesLumbar Disc Herniation: Evidence-Based Guidelines-A Review: The Indian Practitioner March 2016Lee제노No ratings yet
- Point of Care NHJMDocument9 pagesPoint of Care NHJMFernanda Araújo AvendanhaNo ratings yet
- 10 - Brosura Lot 72 - Canon - SemnatDocument24 pages10 - Brosura Lot 72 - Canon - Semnattrinh xuan sonNo ratings yet
- MS UrologyDocument73 pagesMS UrologyZeeshan AliNo ratings yet








































































































Download as pdf or txt
You might also like
- Libro R. Khandpur-Biomedical Instrumentation - Technology and Applications-McGraw-Hill Professional (2004)Document943 pagesLibro R. Khandpur-Biomedical Instrumentation - Technology and Applications-McGraw-Hill Professional (2004)Dulcina Tucuman100% (18)
- Medical Network English JORDAN 1Document342 pagesMedical Network English JORDAN 1Sandhya KhannaNo ratings yet
- Breast Cancer ScreeningDocument21 pagesBreast Cancer ScreeningBolivar Isea100% (1)
- NAIT - Graduate Employment Rates by Full-Time Program PDFDocument5 pagesNAIT - Graduate Employment Rates by Full-Time Program PDFpauloednNo ratings yet
- Manejo Cancer de Mama y EmbarazoDocument10 pagesManejo Cancer de Mama y EmbarazoLaura LealNo ratings yet
- Advances in Screening, Diagnosis, and Treatment ofDocument7 pagesAdvances in Screening, Diagnosis, and Treatment ofBastomy EkaNo ratings yet
- Jmri 26654Document14 pagesJmri 26654marizal saputraNo ratings yet
- Untitled PDFDocument9 pagesUntitled PDFFaruq AbdanNo ratings yet
- Cervical Conization and The Risk of Preterm DeliveryDocument11 pagesCervical Conization and The Risk of Preterm DeliveryGelo ConcepcionNo ratings yet
- Roe 2018Document11 pagesRoe 2018mohamaed abbasNo ratings yet
- J of Obstet and Gynaecol - 2023 - - Update Management of Cervical Precancer LesionDocument12 pagesJ of Obstet and Gynaecol - 2023 - - Update Management of Cervical Precancer Lesionzakiah11No ratings yet
- Colposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Document155 pagesColposcopy, Cervical Screening, and HPV, An Issue of Obstetrics and Gynecology Clinics (The Clinics - Internal Medicine)Annca RoXanna100% (1)
- Cervical Cancer - A Global Health CrisisDocument9 pagesCervical Cancer - A Global Health Crisispb.nakulaNo ratings yet
- 242 FullDocument5 pages242 FullsarahNo ratings yet
- Captura de Pantalla 2021-10-08 A La(s) 7.52.39 A. M.Document10 pagesCaptura de Pantalla 2021-10-08 A La(s) 7.52.39 A. M.LINA MARIA CAMELO COLORADONo ratings yet
- Cervical CADocument10 pagesCervical CAAby ShauNo ratings yet
- Correlation of PAP Smear Findings With Clinical Findings and Cervical BiopsyDocument7 pagesCorrelation of PAP Smear Findings With Clinical Findings and Cervical BiopsyKavita Saxena KhareNo ratings yet
- Journal of The National Cancer Center: A R T I C L e I N F o A B S T R A C TDocument8 pagesJournal of The National Cancer Center: A R T I C L e I N F o A B S T R A C TCirugia SolcaNo ratings yet
- Density and Tailored Breast Cancer Screening: Practice and Prediction - An OverviewDocument12 pagesDensity and Tailored Breast Cancer Screening: Practice and Prediction - An Overviewelisabeth harahapNo ratings yet
- Jco 18 00378Document11 pagesJco 18 00378Valéria CruzNo ratings yet
- Greenwood 2019Document13 pagesGreenwood 2019Ottofianus Hewick KalangiNo ratings yet
- Ijcmr 1184 Dec 28Document3 pagesIjcmr 1184 Dec 28BayuHernawanRahmatMuhariaNo ratings yet
- Tiwari 2017Document3 pagesTiwari 2017Dewa OkaNo ratings yet
- Cervicalcancerprevention: Immunization and Screening 2015Document9 pagesCervicalcancerprevention: Immunization and Screening 2015behanges71No ratings yet
- Diagnosis and Treatment of Cervical Cancer in Pregnant WomenDocument6 pagesDiagnosis and Treatment of Cervical Cancer in Pregnant WomenSofi PiñaNo ratings yet
- The Diagnostic Value of Ultrasound and Mammography in Detection of Breast Cancer in AlbaniaDocument10 pagesThe Diagnostic Value of Ultrasound and Mammography in Detection of Breast Cancer in AlbaniaIJPHSNo ratings yet
- Breast Fine Needle Aspiration Cytology Reporting Icet13i2p54Document6 pagesBreast Fine Needle Aspiration Cytology Reporting Icet13i2p54salijanstarNo ratings yet
- PIIS2213398422000902Document7 pagesPIIS2213398422000902Manas BhatiaNo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 5Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 5EDWIN WIJAYANo ratings yet
- Figo 2018Document15 pagesFigo 2018EJ CMNo ratings yet
- Seminars in Oncology NursingDocument9 pagesSeminars in Oncology NursingangelitostorresitosNo ratings yet
- Effect of Cervicitis On Visual Inspection With Acetic AcidDocument5 pagesEffect of Cervicitis On Visual Inspection With Acetic AcidmonicamoniccNo ratings yet
- Editorial: Molecular Imaging in Breast CancerDocument4 pagesEditorial: Molecular Imaging in Breast CancerKurnia AlkatiriNo ratings yet
- CBEDocument17 pagesCBElovtetaNo ratings yet
- Background Parenchymal Enhancement in Breast MriDocument19 pagesBackground Parenchymal Enhancement in Breast Mridr.elahe.babantaherNo ratings yet
- Cervical Cancer: Prevention, Diagnosis, and TherapeuticsDocument23 pagesCervical Cancer: Prevention, Diagnosis, and TherapeuticsranggadrNo ratings yet
- Poster Session II: ObjectiveDocument1 pagePoster Session II: ObjectivefujimeisterNo ratings yet
- FIGO 2018 - Cervical CADocument15 pagesFIGO 2018 - Cervical CAJP RecioNo ratings yet
- PIIS0002937821019992Document2 pagesPIIS0002937821019992made dharmaNo ratings yet
- Society For Maternal-Fetal Medicine (SMFM) Consult Series #49: Cesarean Scar PregnancyDocument13 pagesSociety For Maternal-Fetal Medicine (SMFM) Consult Series #49: Cesarean Scar PregnancyTandyo TriasmoroNo ratings yet
- Hippokratia 11 063Document4 pagesHippokratia 11 063Wiedya kristiantiNo ratings yet
- 33 - 6507 - e (C) - F (T) - PF1 (VP - SH) - Pfa (H) - Pfa (P)Document3 pages33 - 6507 - e (C) - F (T) - PF1 (VP - SH) - Pfa (H) - Pfa (P)Satish SinghNo ratings yet
- KarsinomaDocument12 pagesKarsinomaWahyudi Pratama HarliNo ratings yet
- Summary of Data: Cervical Cancer and ScreeningDocument10 pagesSummary of Data: Cervical Cancer and Screeningpalomazul007No ratings yet
- Screen-and-Treat Approaches For Cervical Cancer Prevention in Low-Resource SettingsDocument9 pagesScreen-and-Treat Approaches For Cervical Cancer Prevention in Low-Resource SettingsSaddam FuadNo ratings yet
- Cost Effective, Portable, Patient Dedicated Three Dimensional Automated Breast Ultrasound For Point of Care Breast Cancer ScreeningDocument16 pagesCost Effective, Portable, Patient Dedicated Three Dimensional Automated Breast Ultrasound For Point of Care Breast Cancer ScreeningCabbagePotatoNo ratings yet
- Comparison of Ultrasound and Mammography For Early DiagnosisDocument8 pagesComparison of Ultrasound and Mammography For Early Diagnosishdh1224No ratings yet
- Malignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalDocument8 pagesMalignancies in Pregnancy Multiple 2016 Best Practice Research ClinicalorriNo ratings yet
- Screeningforcervical Cancer: Terresa J. Eun,, Rebecca B. PerkinsDocument16 pagesScreeningforcervical Cancer: Terresa J. Eun,, Rebecca B. PerkinsLis RibeiroNo ratings yet
- Cervical Cancer Research 1Document9 pagesCervical Cancer Research 1tivaNo ratings yet
- Cervical Cancer - An Overview of Pathophysiology and ManagementDocument9 pagesCervical Cancer - An Overview of Pathophysiology and ManagementIndah 15No ratings yet
- Will HPV Vaccination Prevent Cervical Cancer?: Claire P Rees, Petra Brhlikova and Allyson M PollockDocument15 pagesWill HPV Vaccination Prevent Cervical Cancer?: Claire P Rees, Petra Brhlikova and Allyson M PollockGina Ionescu AnculeteNo ratings yet
- Professional Med J Q 2012 19 5 620 624Document5 pagesProfessional Med J Q 2012 19 5 620 624monica_elysabethNo ratings yet
- Accuracy of Triple Test Score in The Diagnosis of Palpable Breast LumpDocument4 pagesAccuracy of Triple Test Score in The Diagnosis of Palpable Breast LumpBmu CarreonNo ratings yet
- Ca Cervix y Emb 2Document14 pagesCa Cervix y Emb 2Nathalia M.No ratings yet
- Iva Screening2Document9 pagesIva Screening2ponekNo ratings yet
- Peprah 2018Document7 pagesPeprah 2018Dewa OkaNo ratings yet
- Meijers Heijboer2001Document6 pagesMeijers Heijboer2001Market PlusNo ratings yet
- The Management and Prevention of Anal Squamous Cell CarcinomaDocument10 pagesThe Management and Prevention of Anal Squamous Cell CarcinomaGabriela LemNo ratings yet
- Neoplasia Vaginal, Abril 2022Document6 pagesNeoplasia Vaginal, Abril 2022rafael martinezNo ratings yet
- EMBASE Cowden BreastDocument17 pagesEMBASE Cowden BreastCiudadano “Citizen Dick” VolanteNo ratings yet
- Medip, IJRCOG-5630 O PDFDocument5 pagesMedip, IJRCOG-5630 O PDFSuraj NagarajNo ratings yet
- Atypical Breast Proliferative Lesions and Benign Breast DiseaseFrom EverandAtypical Breast Proliferative Lesions and Benign Breast DiseaseFarin AmersiNo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 17Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 17EDWIN WIJAYANo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 16Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 16EDWIN WIJAYANo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 18Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 18EDWIN WIJAYANo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 7Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 7EDWIN WIJAYANo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 2Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 2EDWIN WIJAYANo ratings yet
- ESMO 2023 Management of Breast Cancer During Pregnancy 6Document1 pageESMO 2023 Management of Breast Cancer During Pregnancy 6EDWIN WIJAYANo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 14Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 14EDWIN WIJAYANo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 18Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 18EDWIN WIJAYANo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 1Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 1EDWIN WIJAYANo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 2Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 2EDWIN WIJAYANo ratings yet
- Vitamin D and Bone Health 6Document1 pageVitamin D and Bone Health 6EDWIN WIJAYANo ratings yet
- ESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 3Document1 pageESMO 2022 EGFR Mutant Non-Small-Cell Lung Cancer 3EDWIN WIJAYANo ratings yet
- Vitamin D and Bone Health 5Document1 pageVitamin D and Bone Health 5EDWIN WIJAYANo ratings yet
- General Principles of Insulin Therapy in Diabetes MellitusDocument24 pagesGeneral Principles of Insulin Therapy in Diabetes MellitusEDWIN WIJAYANo ratings yet
- Vitamin D and Bone Health 4Document1 pageVitamin D and Bone Health 4EDWIN WIJAYANo ratings yet
- Insulin Therapy in Type 2 Diabetes MellitusDocument40 pagesInsulin Therapy in Type 2 Diabetes MellitusEDWIN WIJAYANo ratings yet
- Apollo HospitalDocument106 pagesApollo HospitalNoor Ibne SalehinNo ratings yet
- Surface Guided Radiation TherapyDocument515 pagesSurface Guided Radiation TherapyEduardo RodriguezNo ratings yet
- Notes Extention ListDocument16 pagesNotes Extention ListShivani YadavNo ratings yet
- Ultrasound GuidedDocument6 pagesUltrasound GuidedsaminNo ratings yet
- Principles of Radiation OncologyDocument21 pagesPrinciples of Radiation Oncologydinu_maria95No ratings yet
- Brochure ACUSON ASPENDocument2 pagesBrochure ACUSON ASPENWolaé Mathurin Edmond AmegandjinNo ratings yet
- University Institute of Radiological Medical Imaging TechnologyDocument1 pageUniversity Institute of Radiological Medical Imaging TechnologyV KookNo ratings yet
- Fo23rm Report FULL 2019Document4 pagesFo23rm Report FULL 2019amir_heroNo ratings yet
- A BERT Encoding With Recurrent Neural Network and Long-Short Term Memory For Breast Cancer Image Classification - 1-s2.0-S2772662223000176-MainDocument15 pagesA BERT Encoding With Recurrent Neural Network and Long-Short Term Memory For Breast Cancer Image Classification - 1-s2.0-S2772662223000176-MainSrinitish SrinivasanNo ratings yet
- Philips Healthcare (Suzhou) Co., LTDDocument4 pagesPhilips Healthcare (Suzhou) Co., LTDAli R.MNo ratings yet
- Lower ExtremityDocument1 pageLower ExtremityAmir mushtaqNo ratings yet
- Spinal Tuberculosis A Comprehensive Review For The Modern SpineDocument13 pagesSpinal Tuberculosis A Comprehensive Review For The Modern SpineRaunik BansodNo ratings yet
- 2012 DI Accessories CatalogDocument256 pages2012 DI Accessories CatalogchavanikhilNo ratings yet
- Cerebral Palsy: An Overview: The Centers For Disease ControlDocument8 pagesCerebral Palsy: An Overview: The Centers For Disease ControlAlma PradiftaNo ratings yet
- Professor List For International Students (2021)Document4 pagesProfessor List For International Students (2021)Abrar HamimNo ratings yet
- Physics ProjectDocument17 pagesPhysics ProjectLance ShahNo ratings yet
- ID Perhitungan Nilai Dosis Dan Kontras CitrDocument9 pagesID Perhitungan Nilai Dosis Dan Kontras CitrNur cholisNo ratings yet
- Aquilion PRIMEDocument22 pagesAquilion PRIMEvitapabloNo ratings yet
- Rajiv Gandhi University of Health Sciences, KarnatakaDocument16 pagesRajiv Gandhi University of Health Sciences, KarnatakaSanthana PriyaNo ratings yet
- Radiographic Image Analysis 4Document562 pagesRadiographic Image Analysis 4Jessica Ugalde Mata100% (2)
- Value of Chest Ultrasound in Diagnosis of Community Acquired PneumoniaDocument5 pagesValue of Chest Ultrasound in Diagnosis of Community Acquired PneumoniaHarlan SiMarmutNo ratings yet
- Ebook A Selection of Image Processing Techniques From Fundamental To Research Front 1St Edition Yu Jin Zhang Online PDF All ChapterDocument70 pagesEbook A Selection of Image Processing Techniques From Fundamental To Research Front 1St Edition Yu Jin Zhang Online PDF All Chapterwalter.dyer746100% (12)
- List of Hospitals and Diagnostic Centers Empanelled With CGHS, Delhi W.e.f.01.11Document8 pagesList of Hospitals and Diagnostic Centers Empanelled With CGHS, Delhi W.e.f.01.11sudhanshupandey9No ratings yet
- Lumbar Disc Herniation: Evidence-Based Guidelines-A Review: The Indian Practitioner March 2016Document7 pagesLumbar Disc Herniation: Evidence-Based Guidelines-A Review: The Indian Practitioner March 2016Lee제노No ratings yet
- Point of Care NHJMDocument9 pagesPoint of Care NHJMFernanda Araújo AvendanhaNo ratings yet
- 10 - Brosura Lot 72 - Canon - SemnatDocument24 pages10 - Brosura Lot 72 - Canon - Semnattrinh xuan sonNo ratings yet
- MS UrologyDocument73 pagesMS UrologyZeeshan AliNo ratings yet