Download as pdf or txt
You might also like
- Breast Cancer Case StudyDocument3 pagesBreast Cancer Case Studyyohans TeferiNo ratings yet
- Impact of Induction Chemotherapy On Resectability in Locally Advanced Oral Cavity CarcinomasDocument10 pagesImpact of Induction Chemotherapy On Resectability in Locally Advanced Oral Cavity CarcinomasManoj KumarNo ratings yet
- JCB Art 30512-10 PDFDocument7 pagesJCB Art 30512-10 PDFMed MedNo ratings yet
- Cancers 13 04912Document12 pagesCancers 13 04912mirzaNo ratings yet
- Jkaoms 42 325Document2 pagesJkaoms 42 325shehla khanNo ratings yet
- Oral Cavity TumoursDocument5 pagesOral Cavity TumoursMirza Khizar HameedNo ratings yet
- IJOHNS. 3D Nasopharingeal AngiofibromaDocument10 pagesIJOHNS. 3D Nasopharingeal AngiofibromaMelissa Garcia LezamaNo ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document8 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Research ParkNo ratings yet
- Onam 2022Document24 pagesOnam 2022Elvia Maria Rios BeltranNo ratings yet
- Evaluation of Quality of Endodontic Re Treatment and Changes inDocument4 pagesEvaluation of Quality of Endodontic Re Treatment and Changes inGinna Estefania TutasigNo ratings yet
- Differential Pharmacology and Clinical Utility of Sonidegib in Advanced Basal Cell CarcinomaDocument6 pagesDifferential Pharmacology and Clinical Utility of Sonidegib in Advanced Basal Cell CarcinomaAbdullah Khaerul AzzamNo ratings yet
- 17-Potential Medicolegal RisksDocument1 page17-Potential Medicolegal RisksSUSANNo ratings yet
- Ijri - IJRI 286 19Document13 pagesIjri - IJRI 286 19krishnasantana1988No ratings yet
- Endodontia BPsDocument6 pagesEndodontia BPsIsteicy CortezNo ratings yet
- Dentistry 12 00083Document13 pagesDentistry 12 00083adiNo ratings yet
- JOMFP 19 267bDocument4 pagesJOMFP 19 267bThái BìnhNo ratings yet
- Annals of Medicine and SurgeryDocument7 pagesAnnals of Medicine and SurgeryInggitaDarmawanNo ratings yet
- Mic Coli 2017Document6 pagesMic Coli 2017Orlando CervantesNo ratings yet
- PIIS2212440318300920Document12 pagesPIIS2212440318300920EmiliaAndreeaBalanNo ratings yet
- Japanese Dental Science Review: Yumiko Kawashita, Sakiko Soutome, Masahiro Umeda, Toshiyuki SaitoDocument6 pagesJapanese Dental Science Review: Yumiko Kawashita, Sakiko Soutome, Masahiro Umeda, Toshiyuki SaitoYeni PuspitasariNo ratings yet
- Delayed Management of Squamous Cell Carcinoma of Soft Palate: Case Report and Review of LiteratureDocument11 pagesDelayed Management of Squamous Cell Carcinoma of Soft Palate: Case Report and Review of LiteratureIJAR JOURNALNo ratings yet
- CR 4Document4 pagesCR 4Fitrah AndiNo ratings yet
- EBM 2018 - Head and CancersDocument136 pagesEBM 2018 - Head and CancersChandramohan SettyNo ratings yet
- CranioDocument9 pagesCranioYusuf BrilliantNo ratings yet
- Parakeratinized Odontogenic Keratocyst: A Case Report With 8 Years Follow-UpDocument4 pagesParakeratinized Odontogenic Keratocyst: A Case Report With 8 Years Follow-UpIJAR JOURNALNo ratings yet
- 2021 MO Laser CCEODocument8 pages2021 MO Laser CCEOAndressa A.No ratings yet
- Survival Analysis of Nasopharyngeal Carcinoma in Hasan Sadikin HospitalDocument4 pagesSurvival Analysis of Nasopharyngeal Carcinoma in Hasan Sadikin HospitalRobert ChristevenNo ratings yet
- Survival Analysis of Nasopharyngeal Carcinoma in Hasan Sadikin HospitalDocument4 pagesSurvival Analysis of Nasopharyngeal Carcinoma in Hasan Sadikin Hospitalairin shabrinaNo ratings yet
- Male Breast Cancer: An Institutional ExperienceDocument5 pagesMale Breast Cancer: An Institutional ExperienceIJAR JOURNALNo ratings yet
- 2006 4 Oral - Cancer PDFDocument225 pages2006 4 Oral - Cancer PDFAnonymous ENwjWryNo ratings yet
- WJCC 2 432Document8 pagesWJCC 2 432Noceiba Ben HassenNo ratings yet
- Improvement of Oral Cancer Screening Quality and Reach: The Promise of Artificial IntelligenceDocument4 pagesImprovement of Oral Cancer Screening Quality and Reach: The Promise of Artificial IntelligenceHarisankar BNo ratings yet
- Ejd - Ejd 261 16Document5 pagesEjd - Ejd 261 16Neggy YudibrataNo ratings yet
- Relationship of Adherence To Cervical Cancer Treatment Guideline Towards Patients' Five-Year Survival: Systematic Review of Follow-Up TrialsDocument7 pagesRelationship of Adherence To Cervical Cancer Treatment Guideline Towards Patients' Five-Year Survival: Systematic Review of Follow-Up TrialsBelén SifuentesNo ratings yet
- Staged Surgery For Advanced Thyroid Cancers: Safety and Oncologic Outcomes of Neural Monitored SurgeryDocument6 pagesStaged Surgery For Advanced Thyroid Cancers: Safety and Oncologic Outcomes of Neural Monitored SurgeryAprilihardini LaksmiNo ratings yet
- Hypofractionation in The Real World Rodin 2021Document8 pagesHypofractionation in The Real World Rodin 2021Gloribel BolívarNo ratings yet
- Cáncer de Páncreas.-Kathya Cuevas Méndez.Document15 pagesCáncer de Páncreas.-Kathya Cuevas Méndez.Kathy Cuevas MéndezNo ratings yet
- ANZ Journal of Surgery - 2021 - Yang - Outcomes of Patients With Metastatic Cutaneous Squamous Cell Carcinoma To The Axilla PDFDocument8 pagesANZ Journal of Surgery - 2021 - Yang - Outcomes of Patients With Metastatic Cutaneous Squamous Cell Carcinoma To The Axilla PDFRong LiuNo ratings yet
- Oral Field CancerizationDocument7 pagesOral Field CancerizationFarah UlyaNo ratings yet
- Jced 12 E821Document9 pagesJced 12 E821Tien Li AnNo ratings yet
- Clinical Oral Implants Res - 2020 - Neckel - Influence of Implant Specific Radiation Doses On Peri Implant Hard and SoftDocument13 pagesClinical Oral Implants Res - 2020 - Neckel - Influence of Implant Specific Radiation Doses On Peri Implant Hard and SoftFelix SchweppeNo ratings yet
- Osteonecrosis of The Jaws 2022 Update-1Document24 pagesOsteonecrosis of The Jaws 2022 Update-1Christian BalladaresNo ratings yet
- Carranza's Clinical Periodontology 2002Document6 pagesCarranza's Clinical Periodontology 2002Lia Optimeze Alwayz100% (1)
- (Ajomr)Document10 pages(Ajomr)MuhasbirNo ratings yet
- Gland CarcinomaDocument6 pagesGland CarcinomaVicko PratamaNo ratings yet
- JOralMaxillofacPathol23119-9376184 023616Document9 pagesJOralMaxillofacPathol23119-9376184 023616porkodi sudhaNo ratings yet
- Long Term (10 Year) Outcomes and Prognostic FactorDocument8 pagesLong Term (10 Year) Outcomes and Prognostic FactorNICOLÁS DANIEL SANCHEZ HERNANDEZNo ratings yet
- PIIS0360301622000049Document2 pagesPIIS0360301622000049FNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- A Clinicopathological Study of Supraglottic Malignancy at A Tertiary Care Centre in Central India - May - 2023 - 1448516048 - 6309584Document3 pagesA Clinicopathological Study of Supraglottic Malignancy at A Tertiary Care Centre in Central India - May - 2023 - 1448516048 - 6309584surgeonforlifeNo ratings yet
- Pjms 29 1112Document4 pagesPjms 29 1112Diana IancuNo ratings yet
- Application of Manual Therapy For Dysphagia in Head and Neck Cancer PatientDocument8 pagesApplication of Manual Therapy For Dysphagia in Head and Neck Cancer PatientpoppyNo ratings yet
- PIIS2212440322008513Document1 pagePIIS2212440322008513Karen RodríguezNo ratings yet
- JHeadNeckPhysiciansSurg4129-194289 052348Document6 pagesJHeadNeckPhysiciansSurg4129-194289 052348Javeria MNo ratings yet
- Treatment Evaluation of Odontogenic Keratocyst by Using CBCTDocument6 pagesTreatment Evaluation of Odontogenic Keratocyst by Using CBCTShinta PurnamasariNo ratings yet
- Factors Influencing The Recurrence of KeratocystsDocument8 pagesFactors Influencing The Recurrence of KeratocystsRocio CacñahuarayNo ratings yet
- Unique Presentation of Submandibular Gland Adenoid Cystic Carcinoma: Case Report and Review of LiteratureDocument4 pagesUnique Presentation of Submandibular Gland Adenoid Cystic Carcinoma: Case Report and Review of LiteratureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Head Neck - 2023 - Weaver - A Molecular Guide To Systemic Therapy in Salivary Gland CarcinomaDocument12 pagesHead Neck - 2023 - Weaver - A Molecular Guide To Systemic Therapy in Salivary Gland CarcinomaafissaNo ratings yet
- Epithelial DysplasiaDocument9 pagesEpithelial DysplasiaS HNo ratings yet
- Elective Versus Therapeutic Neck Dissection in Node-Negative Oral Cancer PDFDocument9 pagesElective Versus Therapeutic Neck Dissection in Node-Negative Oral Cancer PDFluxmansrikanthaNo ratings yet
- Cancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondFrom EverandCancer Regional Therapy: HAI, HIPEC, HILP, ILI, PIPAC and BeyondNo ratings yet
- Patil 2014Document5 pagesPatil 2014Guma KipaNo ratings yet
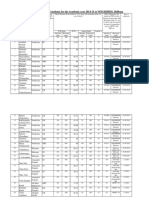
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Document10 pagesAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaNo ratings yet
- e-Hospital@NIC Govt. of IndiaDocument1 pagee-Hospital@NIC Govt. of IndiaGuma KipaNo ratings yet
- Allotment List PCB 8 7 14Document3 pagesAllotment List PCB 8 7 14Guma KipaNo ratings yet
- Neet MDS20Document678 pagesNeet MDS20Guma Kipa0% (1)
- Colon Rectum ResectionDocument28 pagesColon Rectum ResectionAnca TomaNo ratings yet
- Chiara Leo Canine Lymphoma TherapyDocument18 pagesChiara Leo Canine Lymphoma TherapyCabinet VeterinarNo ratings yet
- CA A Cancer J Clinicians - 2024 - Siegel - Cancer Statistics 2024Document38 pagesCA A Cancer J Clinicians - 2024 - Siegel - Cancer Statistics 2024Camilly CampanharoNo ratings yet
- Quality ProjectDocument37 pagesQuality Projectmuhammed shamaaNo ratings yet
- Understanding Ovarian Cancer BookletDocument76 pagesUnderstanding Ovarian Cancer BookletRomina DatuNo ratings yet
- Advocacies of Miss Universe Philippines 2021 CandidatesDocument1 pageAdvocacies of Miss Universe Philippines 2021 CandidatesPauleen PalwaNo ratings yet
- A Review On Anticancer Potential of Some Pyranocarbazole Alkaloids and Its DerivativesDocument10 pagesA Review On Anticancer Potential of Some Pyranocarbazole Alkaloids and Its DerivativesIJAR JOURNALNo ratings yet
- Lesson Plan On Breast Cancer Pathology 2nd Year Bsc. Nursing.Document17 pagesLesson Plan On Breast Cancer Pathology 2nd Year Bsc. Nursing.Suman Pandey100% (1)
- AML Landscape in Asia-Pacific - 2021Document9 pagesAML Landscape in Asia-Pacific - 2021fikriafisNo ratings yet
- W11363 PDF EngDocument8 pagesW11363 PDF EngSaksham AgrawalNo ratings yet
- Task 7 - Final ExamDocument8 pagesTask 7 - Final ExamEdwin MoralesNo ratings yet
- English Articles Test 001 PDFDocument3 pagesEnglish Articles Test 001 PDFroxanaNo ratings yet
- Breast Conditions Other Than Breast CancerDocument2 pagesBreast Conditions Other Than Breast Cancersina bayat shahbaziNo ratings yet
- Verrucous CarcinomaDocument12 pagesVerrucous Carcinomaanatomimanusia100% (1)
- Malignant Tumors of Oral CavityDocument144 pagesMalignant Tumors of Oral CavitySivakumar LakshminarayananNo ratings yet
- Bank Soal Bahasa Inggris TGL 24Document10 pagesBank Soal Bahasa Inggris TGL 24Du SikNo ratings yet
- AHAQualityAdvvisoryEtO 111919Document4 pagesAHAQualityAdvvisoryEtO 111919sabNo ratings yet
- Tanning BedsDocument12 pagesTanning Bedsapi-610404545No ratings yet
- Set 2Document6 pagesSet 2atiqah90No ratings yet
- Gra ViolaDocument8 pagesGra ViolaAnthony SullivanNo ratings yet
- Grammar TestsDocument11 pagesGrammar TestsGeorgina Elizabeth Hernández VilchisNo ratings yet
- Visible Light, Ultraviolet, X-Rays, Gamma Rays Ppt. LessonDocument19 pagesVisible Light, Ultraviolet, X-Rays, Gamma Rays Ppt. LessonJhan Michael Dumandan MahinayNo ratings yet
- Benign and Malignant Tumors of CervixDocument37 pagesBenign and Malignant Tumors of CervixFirifan DiribaNo ratings yet
- Nejmoa 2312117Document14 pagesNejmoa 2312117Carlos SteccaNo ratings yet
- Daftar Pustaka: Universitas Kristen MaranathaDocument9 pagesDaftar Pustaka: Universitas Kristen MaranathaErica ValenciaNo ratings yet
- Monticciolo ACRHiRiskScrDocument29 pagesMonticciolo ACRHiRiskScrCesar ProJimenezNo ratings yet
- Dresslier Supporting The Leukaemia FoundationDocument1 pageDresslier Supporting The Leukaemia FoundationDavroeNo ratings yet
- Cghs Empaneled Hcos Signed Mou With Nha - 240622Document94 pagesCghs Empaneled Hcos Signed Mou With Nha - 240622AnkitNo ratings yet
- MammographyDocument2 pagesMammographyKimoy MacabungaNo ratings yet